 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
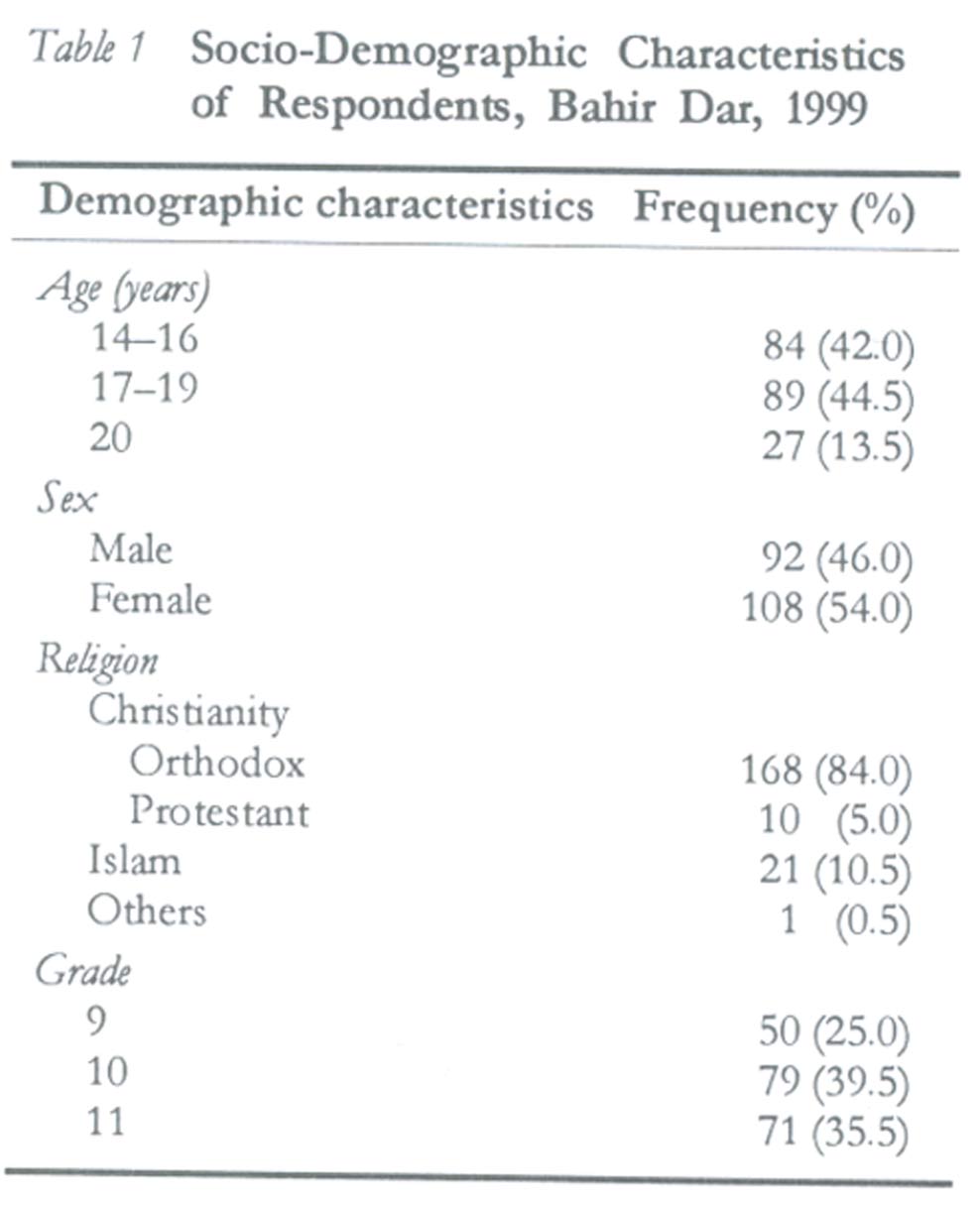
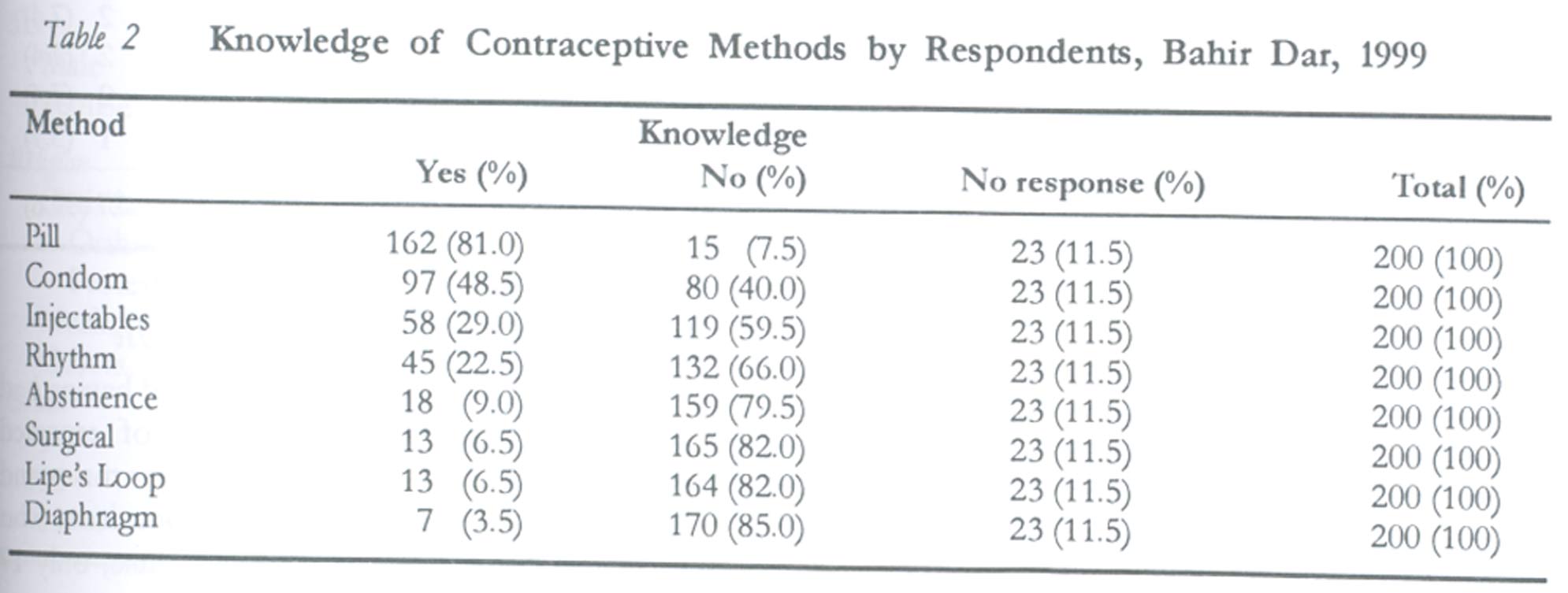
African Journal of Reproductive Health, Vol. 7, No. 2, Aug, 2003 pp. 39-45 Reproductive Health Knowledge, Attitude and Practice among High School Students in Bahir Dar, Ethiopia Mulugeta Kibret Correspondence: Mulugeta Kibret, Department of Biology, Bahir Dar University, P.O. Box 79, Bahir Dar, Ethiopia. Tel: ++251 8 200143 Fax: ++251 8 202025 E-mail: mulugeta64@yahoo.com Code Number: rh03022 ABSTRACT This study was carried out to investigate the reproductive health knowledge, attitude and practice of high school students in Bahir Dar, Ethiopia. Data were collected using self-administered questionnaire and focus group discussions. The study revealed that the students had high level knowledge of contraceptives and where to obtain contraceptive services; however, level of use was low. Some of the reasons given for not using contraceptives include lack of access to services, carelessness, unplanned sexual intercourse and pressure from sexual partner. The study indicates that young people engage in sexual relationships at an early age without protection or with unsafe non-conventional methods. There was no significant difference between the demographic variables and contraceptive use at first intercourse. Educational level of the respondents was the only demographic variable that had significant association with sexual experience (p < 0.05). We recommend improved access to family planning information and services and family life education programmes based on the needs and experience of these young people as a potential solution to alleviate their reproductive health problems. (Afr J Reprod Health 2003; 7[2]: 39-45) RÉSUMÉ Connaissance, attitude et pratique de la santé reproductive chez les lycéens à Bahir Dar, Ethiopie. Cette étude avait pour but d'enquêter sur la connaissance, l'attitude et la pratique de la santé reproductive des lycéens à Bahir Dar, en Ethiopie. Les données ont été recueillies à l'aide des questionnaires auto-administrés ainsi que des discussions à groupe cible. L'étude a révélé que les étudiants avaient un bon niveau de connaissance des contraceptifs et savent là où les procurer; neanmoins, il y avait un faible niveau d'utilisation. Parmi les raisons pour lesquelles ils n'utilisent pas les contraceptifs, selon eux, comprennent le manque d'accès aux services, la négligence, des rapports sexuels non-prévus et la pression de la part du partenaire sexuel. L'étude constate que les jeunes gens s'engagent tôt dans la vie dans les rapports sexuels sans protection ou bien ils utilisent des méthodes non-conventionnelles et dangereuses. Il n'y avait pas de différences remarquables entre les variables démographiques et l'utilisation du contraceptif pendant le rapport sexuel initial. Le niveau d'instruction des enquêtés était la seule variable démographique était liée de manière significative à l'expérience sexuelle (p < 0,05). Nous proposons qu'il y ait un meilleur accès à l'information et aux services en ce qui concerne la planification familiale et les programmes de l'éducation familiale basés sur les besoins et l'éxperience de ces jeunes gens, comme une solution capable d'améliorer leurs problèmes de la santé reproductive. (Rev Afr Santé Reprod 2003; 7[2]: 39-45) KEY WORDS: Adolescents, contraceptive, pregnancy, sexually transmitted diseases INTRODUCTION More than 50% of the world population is less than 25 years old, with one in three people aged 10-24 years.1 In many countries, more than 50% of the population has unprotected penetrative sex before the age of 16, without contemplating the consequences and without accurate information or contraceptive protection. Five million out of an estimated total of 50 million induced abortions worldwide occur in women aged 15-19 years. More than half of women in African countries have their first marriage and begin childbearing be fore the age of 20.1 Reports from studies conducted in Ethiopia also show that women get married before the age of 20.2-4 More than 50% of the people who are infected with HIV/AIDS worldwide are under age 25.5 Pubescent and post-pubescent youths undergo a host of normal physiological and psychological changes that cause them to desire sexual intercourse and take risks. With limited access to information about sex and sexual development, and no access to counselling or sympathetic family planning services as well as sexually transmitted diseases (STDs) clinics, adolescents end up with many un wanted pregnancies and contract myriad of STDs.6,7 Pregnancy and childbirth are more hazardous for girls under 16 years. Hypertension, anaemia, obstructed labour, toxaemia and haemorrhage are more common among teenagers than women aged 20-34 years, and teenagers seeking abortion are more likely to delay finding a provider or to try inducing the abortion themselves. Pregnant teenagers often leave school early and are more likely to be poor.8 The expression of adolescent sexuality has economic and social consequences. Young unmarried women who become pregnant are less likely to complete their education, face greater marital instability, and have fewer assets and lower incomes later in life than women who delay their pregnancy are. Women who get married as teenagers are more likely to dissolve their marriage than those who marry later. Women who first give birth as teenagers are most likely to drop out of school than those who delay motherhood. Lack of education, family instability and lower incomes lead to more adolescent childbearing in successive generations, maintaining the vicious circle.6,9 An urgent need, therefore, exists for young people to protect themselves against HIV/AIDS, other STDs, unwanted pregnancy, and experience safe and healthy sexual development. Efforts aimed at reaching adolescents are more promising than those intended to reach adults. This is because adolescents lack knowledge and skills to prevent pregnancy and STDs, they constitute the majority of the population, they represent a more sensible and important investment in the future for reducing fertility than fertile mothers. Information, education and communication (IEC) programme aimed at achieving behaviour and attitude change among young people is one of the strategies designed to protect young people from STDs, unintended pregnancy and abortion. In order to design optimal IEC programmes, research on the reproductive health of adolescents is needed, results of which could be used to carry out intervention programmes that are appropriate for them. This calls for investigation of the needs and concerns of young people. There is paucity of information on knowledge of contraceptives, sexual practices and related issues of adolescents in Bahir Dar. Although there are few educational activities on reproductive health for the young people, they are not research based. This research was conducted to study the knowledge, attitude and practice of reproductive health among senior secondary school students at Bahir Dar. Data from the study would be useful in designing intervention programmes for the young people. METHODS The study was conducted in Bahir Dar, the capital of the Amhara National Regional State. It is located about 500km north-east of Addis Ababa. The city has a population of 96,140. The study involved 245 (113 males and 132 females) grade 9, 10 and 11 students from Tana Haik and Ghion Senior Secondary Schools in Bahir Dar, Ethiopia. They were randomly selected by our research unit leaders and informed about the aim of the study. In each grade, sections were randomly selected and nearly equal numbers of male and female students were selected based on their age. Data were collected from 200 (92 males and 108 females) students using a self-administered questionnaire that contained open and close-ended questions. The questions elicited information on demographic variables, sexual experience, contraceptive knowledge, sources of contraceptive information, contraceptive use, pregnancy and abortion. The questionnaire was pre-tested on 40 students prior to administration. To complement the survey questionnaire and generate qualitative data, six focus group discussions were conducted with 45 students (21 males and 24 females). There were three male only and three female only focus groups, each made up of six to eight participants. The discussions were audiotaped.10 The survey questionnaire was in Amharic, the local language, while the focus groups were conducted in Amharic. The responses were translated to English before analysis. Data analysis was done using Origin, Data Analysis and Technical Graphics Program version 5.0. RESULTS Two hundred copies of the questionnaire were completed and analysed. The demographic characteristics of respondents are shown in Table 1. Their median and mean ages were 17.2 and 17.5 years respectively (range 14-20 years). Regarding religious affiliation the majority (84%) were Christians (orthodox) and none of them was married. Knowledge of Contraceptive Methods and Sources of Contraceptive Information One hundred and seventy seven (88.5%) of the respondents said they had heard of at least one method of contraception. The pill was the most reported method (162 or 91.5%), followed by condom (97 or 54.8%), injectables (58 or 32.8%), rhythm (45 or 25%). Abstinence, sterilisation, Lipe's loop and diaphragm were also mentioned to a lesser extent (Table 2). In addition to these methods, use of roots and leaves of some plants and abortion as means of preventing pregnancy were mentioned during the FGDs. The young people reported that these traditional methods are available from herbalists in the villages. When they were asked to name their sources of contraceptive information, 102 (57%) mentioned hospitals, 90 (50.8%) mentioned schools, and 79 (44.6%) clinics. Similar proportions (76 or 42.9%) claimed that they got information from television or radio, while newspapers, magazines, parents and friends were mentioned by few of them. Sources of Contraceptives When asked where respondents obtained contraceptives, 71 (35.5%) mentioned health centres, 57 (28.5%) hospitals, 46 (23%) clinics and 26 (13%) other places. The focus group discussants also mentioned similar places. However, results of the group discussion revealed that most young people do not go to health centres, hospitals and clinics. They gave a number of reasons such as embarrassment and the assumption that health centres, hospitals and clinics provide services for married couples and prostitutes for not going there. The following perceptions were expressed by some of the young people:
The adolescents were also asked whether there are special services for young unmarried people in the family planning clinics and health centres like special days, hours and places. Some of them said clinics and hospitals do not serve unmarried people at all. One young boy said: I heard that there are no special days and places. I know that they provide services for all people simultaneously. The discussion on service delivery continued with a question: "What then do unmarried young people do if they do not get services at the clinics, health centres or hospitals?" Respondents said young people resort to pharmacies, medicine shops and traditional healers. They feel more confident to visit these places for contraceptives and they can buy contraceptives there secretly. Some respondents expressed their views as follows:
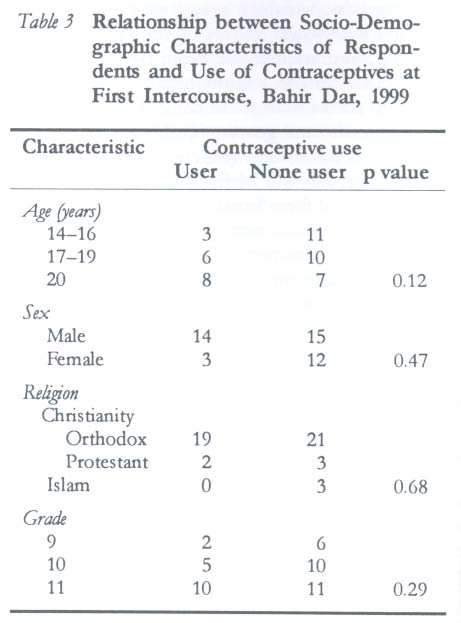
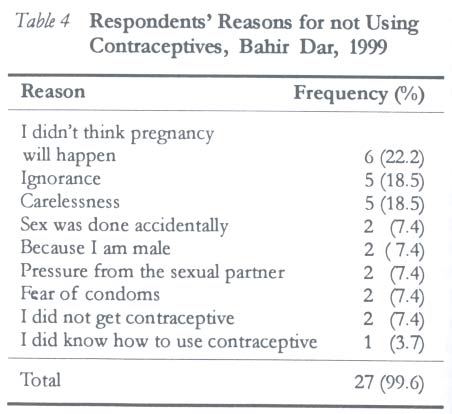
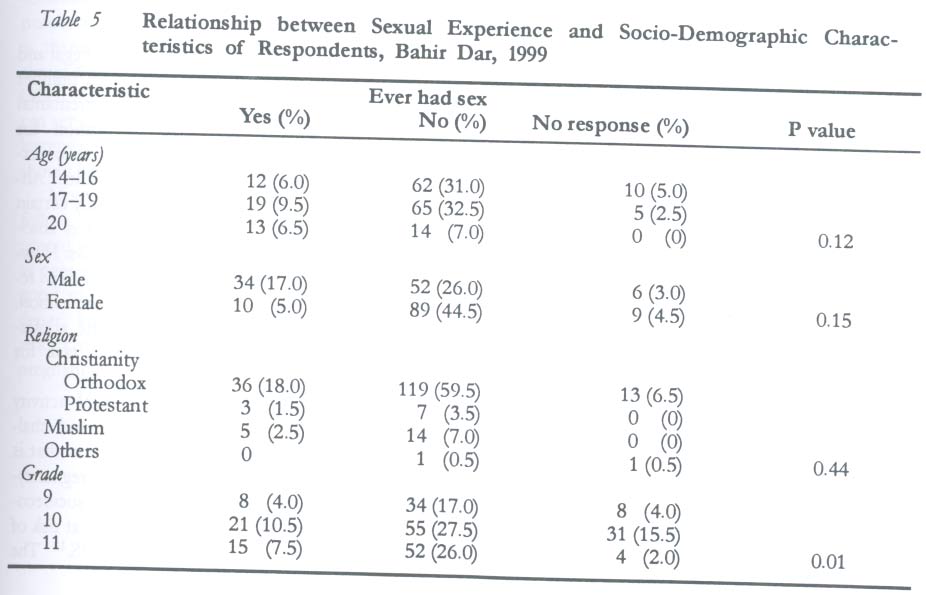
The discussants agreed that to avoid contact with service providers and escape the risks of buying expired contraceptive pills from pharmacies, young people use natural methods of contraception like the rhythm or withdrawal methods and traditional means. Sexual Experience and Contraceptive Use Forty four (22%) respondents reported having had sexual intercourse. The median age of reported first sexual intercourse was 16 years for males and 17 years for females. Of the 44 respondents who reported to have had sexual intercourse, only 17 (8.5%) reported using a contraceptive at first intercourse (Table 3). None of the variables were significantly associated with contraceptive use_ at first intercourse. Out of 17 respondents who reported to have used contraceptives, 7 (15.9%) said they used pills, 5 (11.3%) used condom and 5 (11.3%) used the rhythm or withdrawal methods. Respondents were asked to give their reasons for not using contraceptives and the reasons they gave are shown in Table 4. Results of the focus group discussions indicate that the feeling that some methods are unsafe and fear of losing a partner were responsible for not using contraceptives. Table 5 shows the relationship between sexual experience and demographic characteristics of respondents. No association was found between their age, sex and religion. However, significant differences were found between educational level of respondents and sexual experience (p < 0.05). When they were asked to mention their sexual partner at the first intercourse, 31 (70%) of the 44 respondents reported that they had their first intercourse with a boy/girlfriend, three with prostitutes, while 11 did not mention their sexual partner. Pregnancy and Abortion Regardless of the knowledge of respondents about contraceptives, where to obtain them and level of use many of them still get pregnant. Non-use of contraceptive was not the only reason stated for unintended and unwanted pregnancies. Use of unsafe methods, misunderstanding between partners, ignorance of the consequences of intercourse, rape and unplanned intercourse were the reasons mentioned in the focus groups. Respondents were asked to enumerate what unmarried young girls do when they get pregnant. One hundred and four (52%) of them said they abort the fetus, without stating the method of abortion. Twenty eight (14%) said they abort using traditional methods and 5 (2.5%) said they abort in hospitals. Others said they commit suicide 42 (21%), deliver the child 17 (8.5%), abandon the child and run away from their families, while four (2%) did not give any response. Similar responses were also received from the focus group discussions. However, respondents at the focus group discussions clearly indicated how young people attempt to abort when they get pregnant, as reported in the following comment:
DISCUSSION This study indicates that majority of adolescents have high level knowledge of contraceptive methods, contrary to earlier reports.3,4 The pill and condom as contraceptives were mentioned by many of the respondents. However, level of contraceptive use by young people was low. Many of them know where modern contraceptives are available but do not go there for services. Young people do not view clinics, health centres and hospitals as places where reproductive health services are provided. They feel these places are meant for prostitutes and married people only. Therefore, some resort to such places as pharmacies and shops where counselling is barely present. They rely on natural methods, like the rhythm and withdrawal, which are reported to have high failure rate.11 The problem is also compounded by lack of services. The existing family planning services do not meet the needs of adolescents. Some do not serve adolescents at all, while those that serve both the married and unmarried do so in the same clinic, on the same dates and at the same hours. The young people refrain from going to these clinics because of the fear of service providers and clients. Sometimes the consent of their spouse is required before they are offered contraceptive services. Most of the respondents who reported to have had sexual intercourse were below 19 years of age, majority of which were involved in unprotected intercourse. Ignorance, unintended or unplanned intercourse, carelessness, and lack of access were some additional reasons given for not using contraceptives. Similar barriers to contraceptive use by adolescents have been reported from an earlier survey in Ethiopia3 and other parts of the world.8,11 Although young people may have information about contraception and even have access to services, the extent of communication between partners and the negative traditional perception of premarital sexual activity influence young people's decision-making. None of the demographic variables studied were statistically associated with sexual practice except educational level. Most of the students who reported to have had sex were in grade 10. This calls for great emphasis on awareness programmes for schools. There was also no significant association between contraceptive use at first intercourse and demographic variables. This is in agreement with results from previous studies.3 Respondents had sex with people of their age, while some boys reported having had sex with commercial sex workers. When young people have sex with people of their age they are less likely to use contraceptives and may have unwanted pregnancy. This was clearly pointed out during the focus group discussions.
Unintended pregnancy often ends in illegal and unsafe abortion. Victims may also face a number of consequences such as abortion and premarital childbearing, which can disrupt education for girls.12 Adolescents are also more likely to be exposed to STDs and HIV/AIDS than adults.5 Abstinence from sexual intercourse is the only certain way of preventing pregnancy and it confers absolute protection from AIDS and other STDs. However, abstinence was mentioned only by few respondents as a method of pregnancy prevention. During the focus group discussions, the adolescents said abstinence is an impossible task for young people like themselves. Every option after adolescent sexual activity and unwanted pregnancy has its risks and challenges. The girl may end up with abortion that is carried out under unhygienic condition, pregnancy-associated morbidity and mortality and socioeconomic problems, while both partners are at risk of contracting STDs including HIV/AIDS.12 The pregnant young woman may give birth to a child, thus contributing to adolescent fertility. Adolescent fertility is responsible for 15-20% of total births in sub-Saharan Africa13, contribute 12% of total fertility rate in Ethiopia1 and 11.36% of total births in the Amhara region of Ethiopia.14 CONCLUSION It is good public policy to allow young people have access to contraception in order to prevent unwanted pregnancies, avoid abortions and reduce their chances of contracting or transmitting STDs. Family life education programmes in schools and elsewhere should provide adolescents with essential information on how to refrain from sexual intercourse and the benefits of delaying the onset of sexual activity. Such educational programmes should concentrate on reducing unprotected intercourse by addressing abstinence, low risk sexual behaviour and safe sexual practices. For those who are unwilling to refrain from sexual intercourse, programmes should help increase access to affordable contraceptive services that are appropriate in the context of the young people. Clinics that serve adolescents only, youth centres that include contraceptive counselling, and community outreach programmes that use young people as peer educators have all been effective. It is therefore recommended that family planning clinics that serve adolescents only should be established. Alternatively, existing family planning clinics can set special hours and days for attending to adolescent sexuality and contraceptive needs, and they should be adequately informed about it. Most people are often willing to listen to and follow advice from their peers. Trained and supported young men and women can therefore serve as peer educators. Peer education programmes are good to help young people increase their confidence, knowledge and skill so as to reduce their risk of contacting HIV, other STDs and unwanted pregnancy. REFERENCES
Copyright 2003 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh03022t1.jpg] [rh03022t3.jpg] [rh03022t5.jpg] [rh03022t4.jpg] [rh03022t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}