 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 7, No. 2, Aug, 2003 pp. 57-73 Improving Quality of Care and Use of Contraceptives in Senegal Diouratié Sanogo1, Saumya RamaRao1, Heidi Jones1, Penda N'diaye1, Bineta M'bow2 and Cheikh Bamba Diop2 1Population Council, 2Service Nationale de la Sante
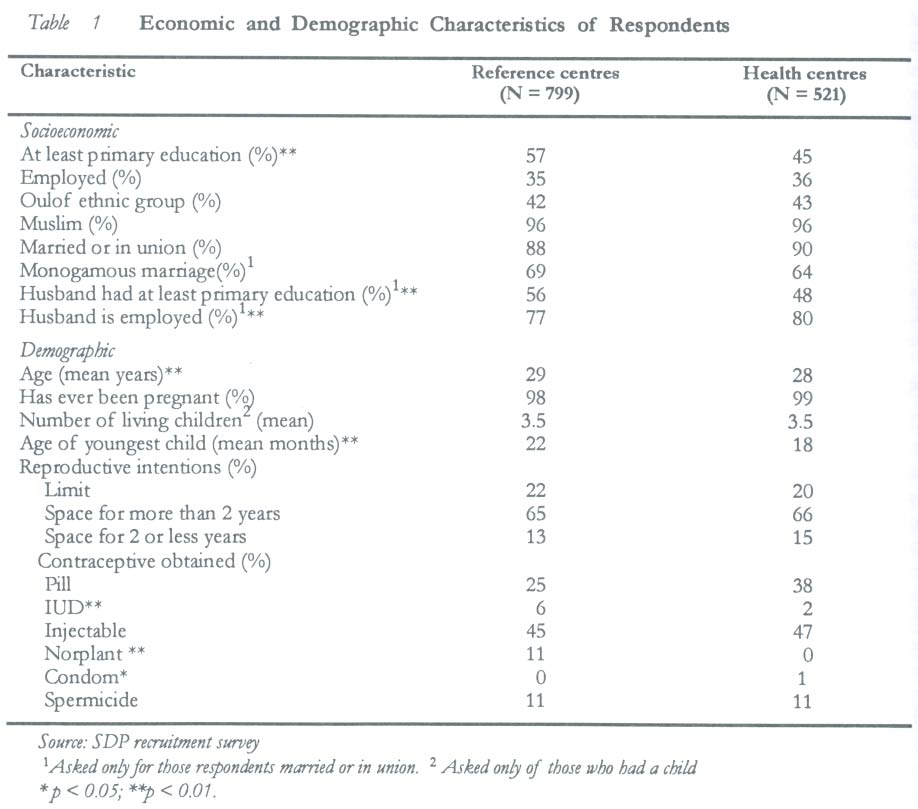
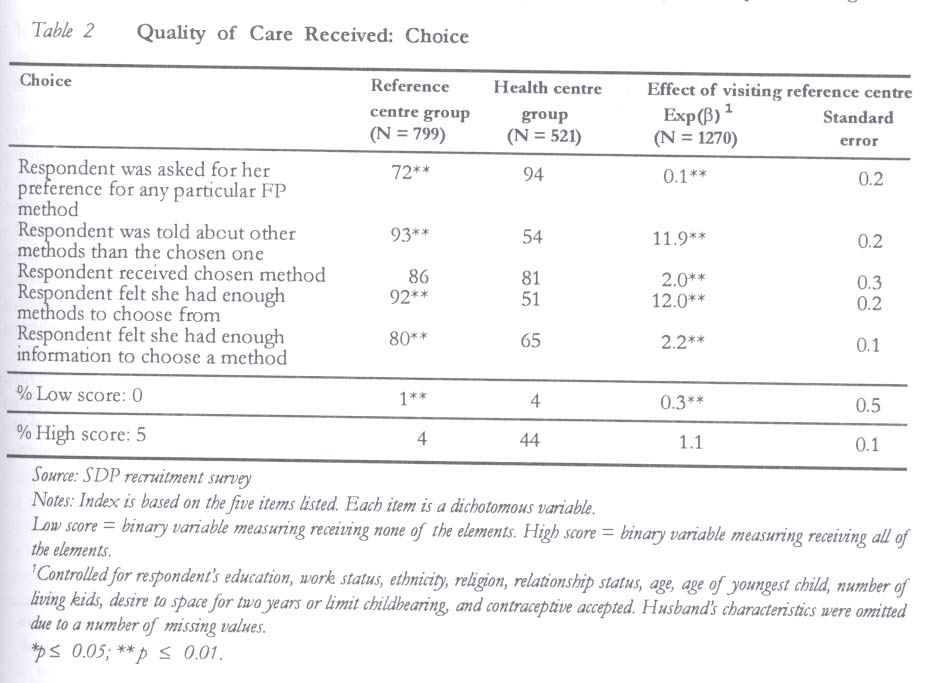
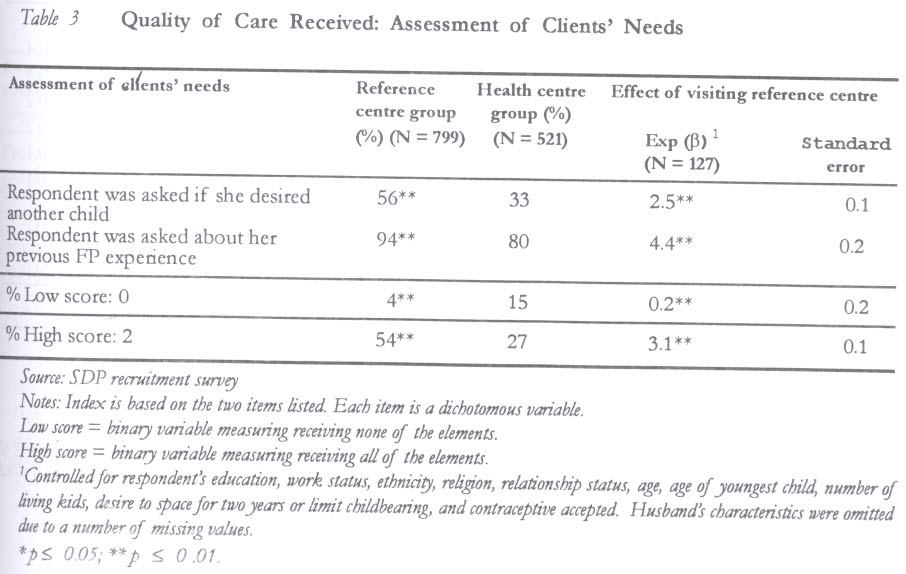
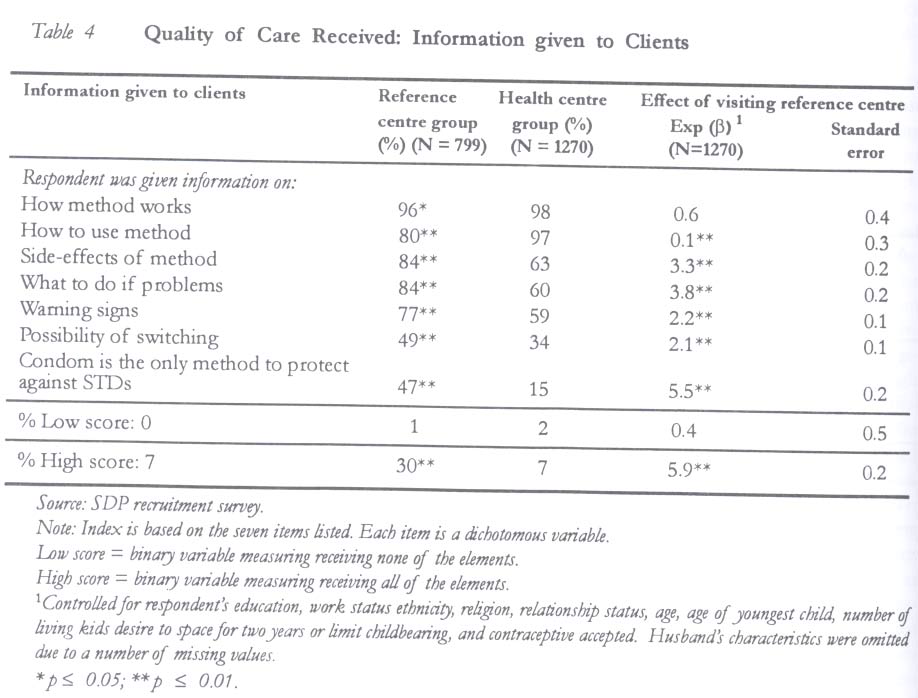
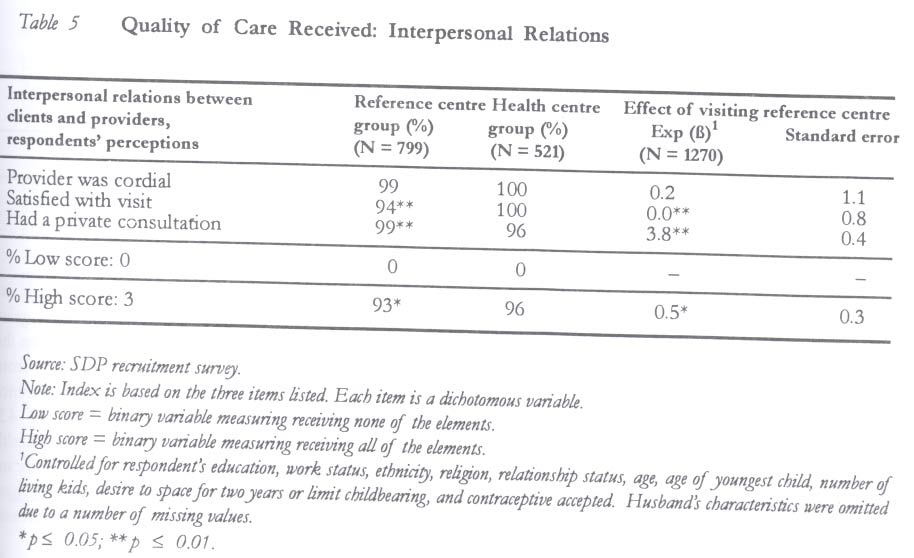
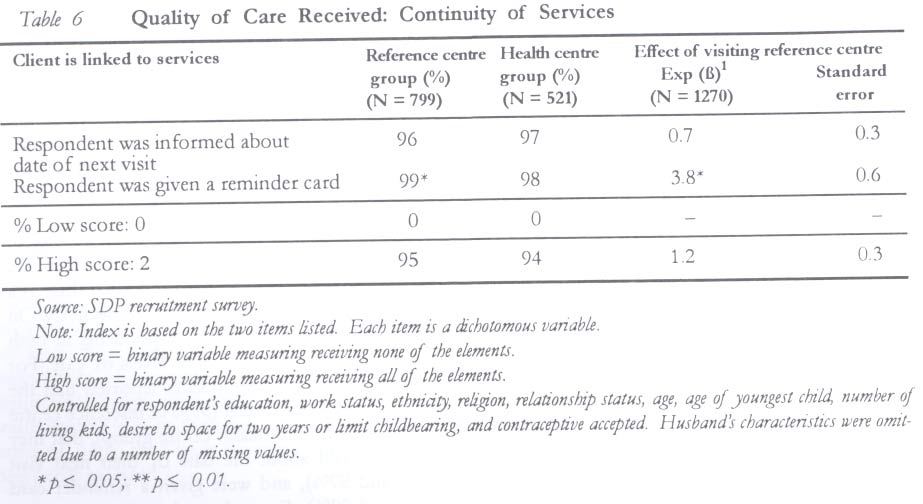
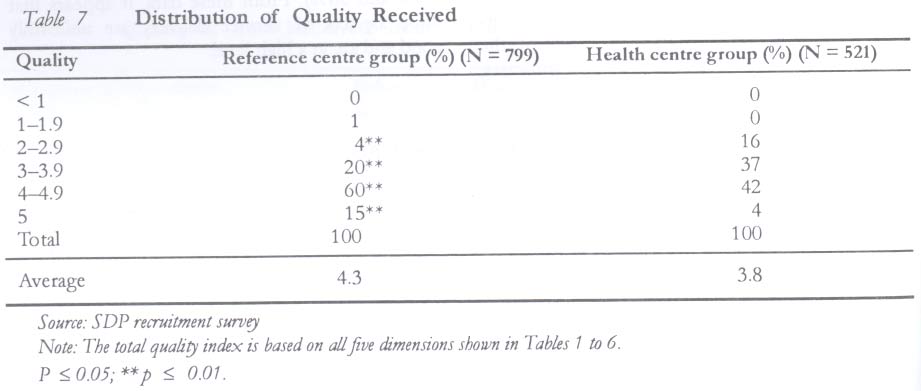
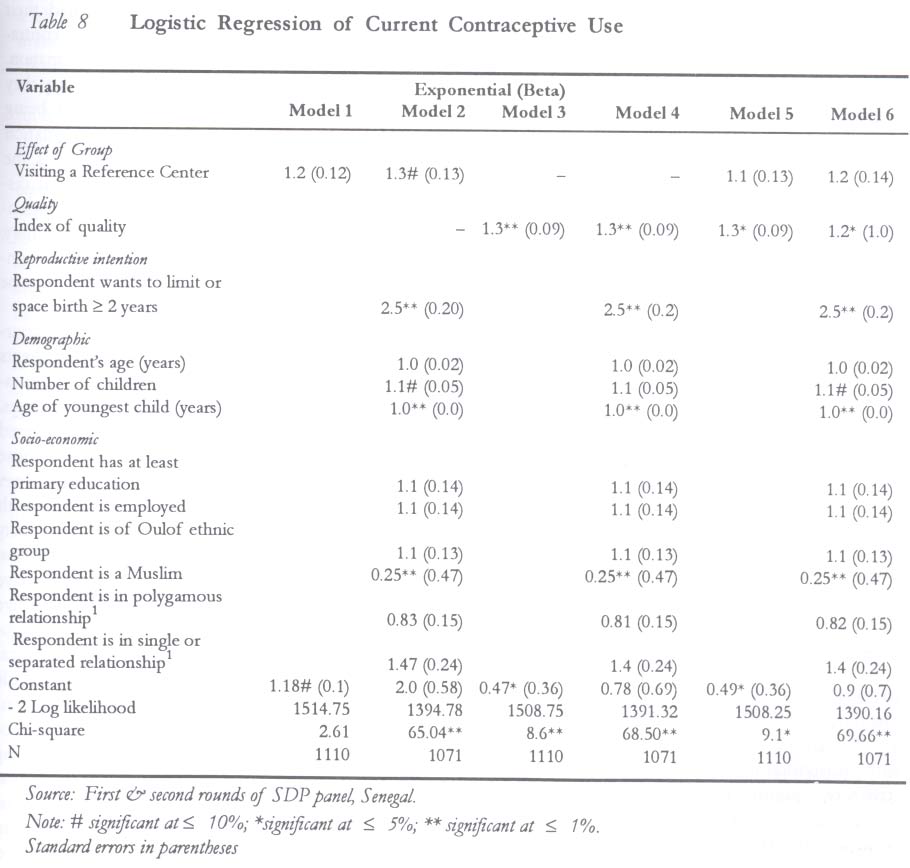
Reproductive (SNSR), Senegal Code Number: rh03024 ABSTRACT In the 1990s, the government of Senegal implemented a series of policy changes for the provision of family planning services through the public sector. A strategy to provide high quality services through reference centres was adopted. This paper presents findings from a longitudinal survey of 1,320 Senegalese women who had sought family planning services at ten public sector facilities - five reference centres and five health centres. Information was collected on the quality of care they received at the time they adopted family planning. One thousand one hundred and ten of the respondents were followed up sixteen months later to ascertain their contraceptive status. The first principal finding was that attendees at reference centres reported receiving relative better care than those who attended health centres. On average, clients at reference centres received 4.3 out of five units of care, compared to 3.8 units as reported by health centre clients. Second, multivariate analyses indicated that quality of care received at the time of adopting a contraceptive has a significant influence on subsequent contraceptive use. Those who received good care were 1.3 times more likely to be using a method than others. (Afr J Reprod Health 2003; 7[2]: 57-73) RÉSUMÉ Amélioration de la qualité et l'utilisation du contraceptif au Sénégal. Au cours des années 1990, le gouvernment sénégalais a mis en ouvre une série de modifications dans la politique pour la prestation des services de planification familiale à travers le secteur public. On a adopté une stratégie pour mettre en place des services de haute qualité à travers des centres de référence. Cette étude présente les résultats d'une enquète longitudinale auprès de 1,320 femmes sénégalaises qui avaient recherché des services de planification familiale auprès de dix établissements du secteur public, cinq centres de référence et cinq centres de santé. On a collecté des données sur la qualité de soin qu'elles ont eu au moment où elles ont adopté la planification familiale. Mille cent dix femmes interrogées ont été suivies seize mois après pour vérifier leur état de contraceptif. La première trouvaille majeure était que celles qui fréquentaient des centres de référence ont signalé avoir été mieux traitée que celles qui fréquentaient les centres de santé. En moyenne, les clientes aux centres de référence ont obtenu 4,3 sur 5 untiés de soin par rapport au 3,8 unités chez les clientes de centres de santé. Deuxiement, des analyses multivariées ont montré que la qualité de soin reçu au moment d'adopter le contraceptif a une influence importante sur l'utilisation ultérieure des contraceptifs. Celles qui ont reçu du bon soin auront 1,3 fois plus de chance d'utiliser une méthode plutôt que des autres. (Rev Afr Santé Reprod 2003; 7[2]: 57-73) KEY WORDS: Quality of care, contraceptive, family planning, health centre, Senegal BACKGROUND Official family planning programme started relatively recently in Senegal. In the late 1970s, though the government recognised rapid population growth as an important issue, there was no well- defined and comprehensive population policy.1 Access to family planning services was limiteda due to the existence of a 1920 French law banning the distribution and sale of contraceptives. However, the next three decades saw a series of policy changes that has culminated in the public sector provision of a wide range of reproductive health services. Policy developments in the 1980s set the stage for new initiatives in family planning. Change began with a repealing of the French law in the early 80s.2 This single change cleared the way for specific projects funded by donors such as USAID and UNFPA to increase access to family planning across all ten regions of the country. Family planning in the 1980s was characterised by individual donor-assisted projects. The two main projects that moved the programme forward were Projet Santé Familiale et Population (PSFP) and Projet Bien-Etre Familial (PBEF), funded by the USAID and UNFPA respectively. These two projects supported the provision of family planning services through the maternal and child health service delivery system of the public, private and the para-private sectors. Access to family planning services increased dramatically in terms of available clinics and trained personnel. The number of service delivery points in the public sector increased from 20 in 1984 to 150 in 1991 with the assistance of PSFP, and the number of trained midwives increased from 20 in 1984 to 300 in 1991. By the late 1980s, there was sufficient official recognition of the need for a population policy and endorsement of family planning. Thus, in April 1988, the Government of Senegal officially adopted a population policy3 that subsequently led to the creation of the National Family Planning Program (PNPF) in 1991. PNPF played a central role in the coordination and implementation of family planning and maternal and child health activities nationwide. Family planning services were offered at PNPF clinics. The major focus areas were improvement in quality, services for adolescents, management of reproductive tract infections including STDs/AIDS, and infertility services. As part of its strategy to provide high quality family planning services, PNPF established one reference centre in each of the 10 regions of the country. In these clinics, improvements were made in several aspects of their functioning including infrastructure, equipment, staffing, commodities and supplies, supervision and MIS. As in other countries, health services in Senegal are structured from primary care at the community level to tertiary care at the hospital level. Primary care is provided at health posts run by male nurses and community health workers. The next level of care is provided by health centres located at the district level. Health centres are usually staffed by a medical doctor, nurses, midwives and community health workers and provide a range of curative and preventive services including family planning. Reference centres were set up at the next higher level - the region. At the regional level, the only other health facility available is a regional hospital with specialised personnel in every area of medicine. Teaching hospitals and other hospitals exist at the apex or national level. Reference centres are closest in functioning and size to health centres; caseloads are similar at both types of facilities. Typically, reference centres are located in the regional capital while health centres are located in a secondary urban city in the same region. In a number of instances, health centres were upgraded to reference centres. Stated differently, while reference centres received a variety of inputs to improve them as per the policy guidelines described, health centres did not benefit from such inputs.b The reference centre strategy was developed to address several identified problems ranging from lack of trained personnel to provide family planning services, lack of equipment and supplies, stock-outs of contraceptives, to poor supervision.4 Specifically, the reference centres were envisaged to provide a range of reproductive health services including family planning, management of RTIs and STDs, maternal and child health, and infertility. They were also meant to train family planning service providers at sub-regional levels and receive cases referred from the region. In addition, the overarching focus was that improving the quality of services was also a means to increasing contraceptive acceptance and continuation. With this aim, 14 reference centres were established; one in each of the ten regions of Senegal and four in Dakar. The process began in phases in 1995 by upgrading physical infrastructure, an effort that was largely supported by UNFPA and the World Bank. In some cases, existing health centres were renovated and upgraded to reference centres, while others were built. Equipment was provided to all the reference centres to facilitate the delivery of family planning services. These included such items as delivery and examination tables, examination lamps, speculums and IUD insertion kits. Mechanisms for regular and adequate supplies of contraceptives and drugs were set in place.c In addition to provision of equipment and supplies, family planning service providers were trained on a variety of issues, including counselling, contraceptive technology, service delivery, supervision, MIS and logistics. The training of providers was conducted by the Ministry of Health and various international agencies.d Further, Norplant7 was added to the range of methods already available. Addition of Norplant® was accompanied by the requisite training of staff and provision of equipment and supplies to ensure service delivery. All reference centres received an improved management information system (MIS), which comprised staff training in maintaining the MIS and allocating a separate space for MIS where client records were maintained. A strategy for following up clients using the MIS was also planned. This was a mechanism to categorise family planning users into current users, users who have not revisited the clinics in time and dropouts. Family planning staff were trained to follow-up discontinuers and dropouts. Clients were to be provided with appointment cards that indicated the date of return to the clinic. Therefore, clients who did not return for their re-supply or check-up could be identified and then followed up at home.e Finally, reference centres were envisaged to be regional training centres for family planning service providers in various aspects of service delivery, including counselling, knowledge update and service provision. However, this is not yet fully operational. Thus, reference centres have received considerable inputs, some of which have been directed to improving the readiness of the service environment by removing physical infrastructure and logistic constraints. Others were directed to improving the care that clients receive. In summary, government envisaged that by adopting the reference centre strategy, the problems identified earlier would be solved and that it would result in increased acceptance of contraception and higher continuation. Within the context of rapid changes in policy and programme directionf, government has been keen to assess the effects of some of its strategies. There is particular interest in evaluating the creation of reference centres. This paper documents in an empirical manner two specific aspects of the strategy: (1) whether there has been any improvement in the care received by clients and (2) whether quality improvements have had an effect on the contraceptive use of facility attendees. HYPOTHESES The positive association between quality and contraceptive behaviour has been theorised and has found acceptance largely because of its intuitive appeal. It builds on the notion that quality improvements will assist individuals to use contraception and to do so effectively and for longer periods. In addition, it helps them avoid unintended pregnancies. Quality has many dimensions and includes availability of buildings, personnel and supplies, technical competence of providers, and interpersonal contact between provider and client. These dimensions have been identified by researchers and programme staff through experience and observations.5,6 For example, the experience of introducing new contraceptives into existing public sector programmes has provided many lessons and insights about the importance of quality and its dimensions.7-9 Of all the various dimensions, current programme and research effort focuses on the client-provider interaction, as it is considered an integral part of the care process.g Much has been written about the client-provider interaction and the hypothesised effects of a good interaction on clients.5,10-13 However, empirical evidence to support this hypothesis is only slowly emerging. Some facets of the care giving process have been found to have an effect. For example, being given the contraceptive method of choice, or adequate information, or perceptions of the helpfulness of the provider have been found to be positively associated with contraceptive acceptance and continuation. To elaborate, a follow-up study from Indonesia found that women who were given the contraceptive they chose were significantly more likely to continue contraception a year later than those who were not. The rate of discontinuation was 9% among those who got their method of choice, compared to 72% among those who did not.14 These results were derived from a multivariate analysis with a number of relevant controls and, hence, are convincing in their import. A second factor that has been found to positively influence contraceptive behaviour is being given information especially about side-effects. Three studies from West Africa, China and India document that women who received more information were less likely to discontinue contraception.15-17 For example, the West African study found in Niger and Gambia that discontinuation was higher among women who reported inadequate counselling about side-effects. In Niger, 37% of such women stopped using contraception, compared to 19% of others. Similarly in Gambia, 51% of those who reported inadequate counselling stopped using a method, compared to 14% of the others. Similar results are reported from the Chinese and Indian studies. Though these findings are encouraging, there are methodological issues to contend with. Women who discontinued could also have been more likely to report that they received less information than others. Clients' perceptions of providers and their behaviours also seem to be associated with contraceptive adoption and continuation.18 A study of 3,632 Bangladeshi women reported that clients who perceived their provider to be responsive to inquiries, sensitive about their privacy, helpful with problems, sympathetic to their needs, and provided information were 27% more likely to adopt contraception over the next 30 months. Similar effects were reported among those who were already using contraception. Women who perceived their provider to be providing higher levels of care were 22% and 72% more likely to continue on some methods of contraception, compared to those who rated the provider to be providing low levels of care. Thus, the empirical evidence has identified some aspects of the care giving process such as provision of clients' chosen method, adequate information and humane treatment as being significant factors of contraceptive use. The detection of these relationships leads to the possibility of other factors in the client-provider interaction, which may influence contraceptive use. Recent research from the Philippines analysed the client-provider interaction in its entirety, from whether the client was treated well, had her needs assessed, given sufficient information, provided with a variety of options, to being linked to services in the future. It also combined all these aspects into a single indicator of quality of care.19 The findings indicate a significant and positive effect of quality on contraceptive continuation. This provides empirical support to the concept that quality includes many dimensions and suggests that research should include as many dimensions of quality as possible and not select elements alone. Accumulation of evidence from a variety of settings and experimentation with a variety of indicators of quality will help identify additional dimensions. All these will be useful for service delivery. STUDY SETTING The research described in this paper was undertaken in five of the ten regions in Senegal. Thies, Kaolack, Saint Louis, Tambacounda and Fatick were selected based on three criteria: the presence of a functioning reference centre in the region, a high family planning client case load, and absence of civil disturbance.h These five regions are similar in many aspects. The areas are inhabited by members of the Ouolof, Serere, Poulaar and Mandingue ethnic groups, and Islam is the predominant religion. Between 33% and 60% of children attend schools. In terms of industrial activity, each region has not more than one or two factories manufacturing salt, sugar, textiles or mining. All the study regions also benefit from the assistance of a number of international collaborating agencies in the delivery of economic, educational and reproductive health services. There are also some marked differences across the regions. Kaolack, Fatick and Tambacounda are mostly rural while Thies and Saint Louis regions are the most urbanised. The extent of urbanisation ranges from 10% in Fatick to 34% in Thies.20 A composite indicator of overall living conditions also suggests that this distinction persists, with the Thies and Saint Louis faring better than the other rural regions. Economic opportunities in the three rural regions tend to be in agriculture, with peanut, cotton and cattle farming, while fishing and tourism are the main activities in Thies and Saint Louis. A second more striking distinction is the accessibility to health and family planning services. Thies and Kaolack have well developed health infrastructure compared to the other three regions. Thus, the selection of these regions provides sufficient variation in pattern of urbanisation, economic opportunities and overall development. The aggregation of these five regions is as close to national representation as possible. METHODOLOGY Data Collection In this paper, we present data from two sources, namely, an interview with contraceptive users at the time they were enrolled into the study and a follow-up interview with the same respondents approximately 16 months later. One thousand three hundred and twenty respondents were enrolled into the panel from ten clinics (five reference centres and five health centres).i They were enrolled between October 1997 and January 1998 when they had visited the facility for service and had consented to be part of the study. As part of the informed consent procedure, every respondent was informed about the objectives and nature of the study, the right of voluntary participation including refusal to answer specific questions, the right to privacy of records and confidentiality of the information provided. They were also informed about the lack of incentives or disincentives related to participation, and phone numbers should respondents seek additional information. Respondents selected for the panel were first time users of contraception, first time users of a specific method, or switchers, and those re-starting after a hiatus. The interview took place in the facilities soon after they had received services. Information was collected from them on their perceptions of the quality of services they received, detailed knowledge of the contraceptive method accepted, their background characteristics, summarised reproductive history and reproductive intentions. Respondents who visited both types of facilities were fairly similar in a number of background characteristics such as ethnicity, religion, marital status and work status (Table 1). However, respondents who visited the reference centres were more likely to be educated, be older, have a slightly older last child, and be on a different contraceptive than those who visited health centres. These differences between the groups are offset by the similarity in the mean number of living children or reproductive intention, which are crucial variables for this study, as they determine future contraceptive and reproductive behaviour. In sum, the respondents are as similar as can be between the two groups. The follow-up interview took place between March and June 1999, approximately 16 months after the first interview either at the facility or at home.j In all, 1110 respondents were followed up. The follow-up rate was 84%: 83% of the respondents who had sought services at reference centres and 86% of those at health centres, with no significant difference in the follow-up between the two groups. Loss to follow-up was 16%. Reasons for loss to follow-up include relocation (52%), inability to locate residence (23%),k missed interview call (17%) and refusal to keep appointment (7%). This interview collected information on the reproductive and contraceptive behaviour as well as experiences with the health care system since the first interview. We checked for selection bias of respondents for the follow-up interview. In general, the extent of selection bias was limited (Table 1). It was not an issue for a variety of respondent characteristics such as education, work status, marital status, type of marriage (monogamy or polygamy), ethnic group, religion, reproductive intention, method obtained at time of recruitment, or age of last child. However, there was selection in terms of the respondent's age, number of children, whether she wanted to cease childbearing, and her husband's education. Respondents in the follow-up had a tendency to be on average 2.4 years older, had on average 0.7 more children, more likely to want to limit childbearing, and more likely to have a husband with at least primary education than those not followed up. However, more importantly, selection did not change the existing distinctions between the two groups. For example, respondents who visited reference centres were older than those who visited health centres, and this remains in the follow-up as well.l In addition, respondents in both groups on average had 3.6 children. Variables and Analysis There are two parts to the analysis. The first examined whether there were differences in the care that clients received according to the type of facility visited while the second examined outcomes at the client level. It looked at the effect of visiting a reference centre and of quality on clients' subsequent contraceptive behaviour. In the first part, we used data from the first round of interviews with panel respondents and examined the quality of care they reported receiving. This reflects their perceptions and subjective evaluation of the care received. Five different indicators of quality capturing various aspects of the care giving process were used, namely, whether the client was provided choice, had her needs assessed, was provided information, was treated well by the provider, and whether she was linked to future services. These indicators have been chosen on the basis of theoretical and conceptual work, which initiated the field of study on issues of quality5,6, and by the empirical work cited earlier. Each of these indicators was considered to be equally important in the care giving process. Sometimes programme managers ask researchers to rank the indicators in order of importance, but we desist from such exercise as we believe that such ranking is arbitrary and is the subjective choice of individual researchers. Also, relying on solely empirical evidence can be misleading as they can be devoid of theoretical meaning and content. Each indicator comprised several items that reflected a specific dimension. For example, the indicator of choice was made up of five dichotomous items, each of which represented a unique dimension. These were whether the client was asked her preference for any method, whether she was told of methods other than the one she chose, whether she received her method of choice, whether she felt that there were sufficient methods for her to make a choice, and whether she felt she had enough information to make a choice. As the number of items comprising an indicator varies from two to seven, in order to ensure equal weighting of each indicator, we have normalised each to unity. Hence, the quality indicator, which is the totality of the five dimensions, ranges in value from zero to a maximum of five. As the analysis focused on finding differences between the groups visiting the two types of facilities, we used bivariate techniques. Chi-square tests were used to distinguish similarities or differences between the two groups. We further tested if visiting a reference centre affected any aspect of care received in a multivariate logistic model, where a number of controls were introduced for the respondent's socio-economic background. The second part of the analysis tested the following hypotheses: (a) respondents who visited reference centres would be more likely to use a contraceptive than those who visited health centres due to specific efforts to improve quality in the former, and (b) respondents who had received better care, irrespective of the treatment group they belonged to, would be more likely to use contraceptives than those who did not. For these analyses, respondents were linked over time from their enrolment to follow-up. Use of contraception at the time of follow-up was the dependent variable and all the independent variables, including quality of care that respondent received and her background characteristics were measured at the time of first interview. Having visited a reference centre and the quality of care received were the critical independent variables under study. In these analyses, we used a comprehensive measure of quality, which encompassed all five aspects, namely, choice, needs assessed, information, interpersonal relations and continuity of services. This combined measure is the sum of the weighted average of each indicator. The effect of having visited a reference centre and of quality on contraceptive use was tested in multivariate logistic regression models where other socioeconomic background variables were controlled. RESULTS Table 2 presents information on the choice that clients reported receiving. Clients who went to reference centres were more significantly likely to report that they were informed about at least one other method than the one they chose (93% versus 54% who visited health centres), that they received the method of choice (86% versus 81%), felt that there were enough methods (92% versus 51%) and had sufficient information (80% versus 65%) to make an informed choice. It is also interesting to note that they were significantly less likely to be asked about their preference for a method than those who visited health centres (72% versus 94%). One explanation for this seemingly anomalous finding is the differences in the processes of service delivery in the two types of facilities. At reference centres, clients receive services from two providers, a counsellor and a midwife. Service provision begins with a session with the counsellor who informs the client about the various contraceptive options available at the facility and pertinent information on each method. Thus, the client is prepared with sufficient information and is able to make a tentative selection of a method before she meets the midwife. The client informs the midwife about her selection and the latter repeats the relevant information specific to the chosen method, answers any questions that the client may have, and dispenses the contraceptive. Thus, in this process, as midwives do not specifically ask clients about their method of choice, it is not likely to be reported in the exit interviews. In contrast to this process of service delivery, at health centres, clients meet with only one provider who enquires about their preference and then provides them with it without much information on other contraceptive options available at the clinic. The physical layout of reference centres in terms of a waiting room, counselling room and a service delivery room aids the flow of clients through these various stations. Also, reference centres, in contrast to health centres, were more likely to have explicit diagrams and posters on the walls depicting the client flow. Field visits to these facilities and conversations with service providers indicate that the reference centre strategy emphasised this specific method of service delivery, which allows greater contact of clients with providers. It is also interesting to note that the differences between the two groups on all these items persist after controlling for a range of variables reflecting the respondent's background as shown in the right hand side panel of Table 2. This indicates that reference centres are indeed more successful in increasing the choice that clients receive. Significant differences were also observed in two other aspects of quality - assessing clients' needs and the information provided to them. Respondents from the reference centre group were more likely to report that the provider had asked them of their reproductive intention (56% versus 33% in health centre group) and about their previous family planning experience (94% versus 80%) (Table 3). These findings were borne out by the multivariate model as well where the odds of being asked of reproductive intentions were two and a half times higher among reference centre attendees than among health centre attendees. Similarly, respondents from reference centres were over four times as likely to be asked about their previous family planning experience. It is interesting to note that providers in both types of facilities are more likely to ask about family planning experience than reproductive intentions. At one level, it is intuitively understandable that clients visit family planning clinics only when they wish to avert pregnancies and hence any query about their desires to space or limit childbearing are superfluous. However, such enquiries are important inputs, as they inform the provider about the relevant contraceptive options she can offer the client (options available to those who wish to limit childbearing are qualitatively different from the ones available to those who wish to space). It is also evident that while clients at reference centres receive relatively better services than those at health centres, there is considerable room for improvement, as over two fifths of the women were not asked their reproductive intentions. Overall, respondents who visited reference centres were significantly more likely than those who visited health centres to have their needs fully assessed. In terms of odds, they were thrice as likely to have their needs assessed. Another important finding is that attendees of reference centres got more information. It has often been cited in literature that family planning service delivery is characterised by low levels of information that providers give their clients. Often, providers do not inform clients of the side effects of the methods in the fear that it will dissuade them. Sometimes they withhold relevant information. For example, the condom is the only method to protect against STIs and HIV.21 Confirming similar results is a recent study from Jamaica where a lack of complete information about side-effects, correct use of methods, and a tendency to believe rumours were important reasons for discontinuation.22 Information empowers clients to make appropriate choices and is as valuable a commodity as the contraceptive method. Thus, services that provide information in addition to the contraceptive are indeed of good quality. Greater proportions of women attending reference centres (30%) reported being told all seven pieces of information, while less than 10% of those attending health centres did so (Table 4). Further, they were at least 15 percentage points more likely to be told more information than their health centre counterparts on specific items. For example, they were told of side effects of their method (84% versus 63% in health centre group), its warning signs (77% versus 59%), what to do if they have problems (84% versus 60%), and that the condom is the only available method that protects against STDs (47% versus 15%). As seen in the multivariate analyses of previous indicators, the effect of being in the reference centre group net of other background influences remains significant. Given the high levels of information that these respondents received it is puzzling to note that they were less likely to report being told of how their contraceptive method works (96% versus 98%) or how to use it than those in the health centre group (80% versus 97%). We surmise that these results could be artefacts of the service delivery process noted earlier. In summary, respondents who visited reference centres did in fact receive more information than those who visited health centres, they were six times more likely to receive all seven pieces of information than the others. However, there is scope for further improvements especially on those relating to the possibility of switching and methods offering STIs protection, as about half the respondents were not informed on these items. Tables 5 and 6 present two other aspects of care, the interpersonal relationship between the provider and the client and ensuring that there is a mechanism for continued services respectively. On all items of the two aspects, respondents in both groups reported near universal levels of care. For example, nearly all respondents reported that the provider had been cordial (99% in reference centre group and 100% in health centre group), that they had been told about the date of their next visit (96% and 97%), and were given a reminder card (99% and 98%). From these data, it appears that these aspects of service delivery are uniformly good and are at a high level. In summary, the evidence presented in Tables 1 to 6 suggests that the effects of the reference centre strategy can be observed in higher standards of some elements of care provided to clients who visit them. The greatest improvement seems to have occurred in the content of information exchanged between provider and client. On other items, clients who visited either facility received similarly high levels of care, while on some items respondents who visited health centres fared better. Thus, combining all the items into a single index will show the net gain or loss, as the gains made on specific items would be adjusted by the losses made on others. On a scale ranging from unity to five, respondents who visited reference centres reported receiving a mean quality of 4.3, compared to 3.8 among those who visited health centres, a difference that is statistically significant (Table 7).m Multivariate analyses confirm that having visited a reference centre significantly increases the care received by half a unit (0.45) (analysis not shown). These findings are consistent with those reported on each individual index of quality. Client Level Impact In this set of analyses, we examined the extent to which panel respondents were using contraception after having come into the study as new contraceptive acceptors. The following multivariate analyses tested whether having used a reference centre or having received good quality care had an effect on contraceptive use after controlling for a host of other influential factors. At the time of the follow-up interview, 57% of the respondents reported that they were using a contraceptive method (59% of those who were enrolled from reference centres during their visit and 54% of those who were enrolled from health centres). Table 8 presents results of six multivariate logistic regression models. The purpose of the models was to examine the effect of the critical independent variables (visit to a reference centre and quality of care) singly and along with other pertinent controls. Thus, models 1 and 2 indicate the effect of visiting a reference centre for contraceptive service, models 3 and 4 that of quality, and models 5 and 6 of the effect of both variables on subsequent contraceptive use. From models 1 and 2 it is clear that having contraceptive services at a reference centre did increase the likelihood that a respondent was using contraceptives, with the effect showing a minor increase in magnitude and significance, albeit at the 10% level when controls were added. The effect of quality on the other hand was more significant as seen in models 3 and 4. It is in the direction postulated with those who receive better care being more likely to continue using contraceptives. On average, women who received better care were 1.3 times more likely to be using contraception than others. Furthermore, the magnitude and direction of the effect remained unaltered as controls were added to the model. Models 5 and 6 reflect the effect of each of these independent variables controlling for the other. It is noteworthy that the direction and magnitude of both obtaining services at a reference centre or quality remained unchanged when they were used as covariates in the same equation. In sum, this set of models indicates that visits to reference centre and quality of care are important determinants of contraceptive use, with the quality variable being more significant. The quality of care a woman receives is an important determinant of whether she will use contraception over a year and a half later. CONCLUSION This paper described the effects of a policy and programme change in the provision of family planning services undertaken by the government of Senegal. It focused on the effect it had on clients using the services, specifically in terms of their contraceptive behaviour. The objective of the paper was to provide documentation of the programme efforts and the impact they have on contraceptive use. Documentation such as this is necessary to provide information and evidence to other public sector initiatives. The government of Senegal envisaged the strategy of creating reference centres for family planning to increase access while maintaining quality. This ambitious strategy has been implemented with substantial inputs provided to improve infrastructure, equipment, supplies and personnel skills. Public sector provision of family planning in Senegal is barely a decade old and current contraceptive prevalence is low at less than 10%. Government is keen to move the family planning programme ahead and, hence, there is an urgent need to learn from the experience thus far. This paper reports that the reference centres do indeed offer significantly better care to clients than other health facilities, especially health centres that have similar functions and caseloads as reference centres. The differences in quality of care between the two types of facilities are reflected in the nature of transactions between providers and clients during consultations. Providers in the reference centres were able to provide better client-oriented care as reported by clients themselves. Exit interviews with clients indicate that those who attended reference centres had their needs assessed better, were offered more contraceptive choices, and received relevant information. All clients, regardless of the type of facility they visited, reported being treated well and being linked to services. It thus seems that information exchange between providers and clients is the critical component in their interaction that distinguished the type of care received by respondents in the two types of facilities. In summary, these data provide persuasive proof that such improvements in the process of care giving can be made. The impact of high quality care is also encouraging. There is clear empirical evidence that clients who received good care at the initiation of contraception indeed continued to use contraceptives. The analyses indicated that clients who received good care were 1.3 times more likely than those who did not to continue using contraceptives over a year later. These findings are consistent with those reported by other researchers from a variety of different settings. As noted in earlier sections, some elements of quality such as information have been reported to have an effect on contraceptive continuation.15-18 Research has repeatedly documented the importance of information for contraceptive continuation. Discontinuation due to side effects is an oft reported finding. Women discontinue contraceptive use due to their experience of side effects, lack of accurate information including management, coupled with erroneous information from the rumour network nudging women to discontinue.22 Other aspects of quality reported to have an effect include being provided the method of choice and humane treatment.14 Yet another study that used a composite indicator of quality similar to the one used in this paper also found that contraceptive use increased significantly with good care. At low levels of care the predicted probability of contraceptive use was 55%, increasing to 67% at the highest level of care.19 Based on this background of research and evidence, the paper makes a case for including more dimensions of quality that capture more of the essence of the client-provider interaction rather than concentrating on any single aspect. For illustration, accurate and complete information provided without proper assessment of the client's needs may be irrelevant. Or the availability of a choice of methods without adequate information or humane treatment may be a harsh choice indeed. For these reasons, we believe that it will be useful to include the five dimensions of quality as discussed in this paper. Second, we would also like to sound a note of caution. Every aspect may be equally important and, hence, efforts to rank them must be stopped at this stage. Finally, in addition to the indicators used in this paper, a plethora of additional ones have been suggested. For example, information collected from users and non-users have identified service cost, waiting time for consultation and perceptions of cleanliness of facilities as some important factors. It is important to have a conceptual framework in mind for identifying variables so that the indicators will have both theoretical and programmatic value. A mere identification and listing of variables unaccompanied by a theoretical framework may lead to misleading programme and service delivery emphases. The paper also reported the association between an intervention to improve quality and subsequent contraceptive use. Despite improvements in quality of care in the facilities that have received additional inputs, contraceptive use is not significantly higher among attendees of these facilities than others. Contraceptive use was 59% among those who had visited reference centres, compared to 54% among those who visited health facilities. A result that is not statistically significant. This finding does not imply that the reference centre strategy did not work. On the contrary, clients who were served at reference centres did indeed receive better care than those who went to health centres (Tables 2,3,4,5,6). However, some clients who visited health centres also received good care, albeit in lower proportions. Therefore, to elicit a statistical significant increase in contraceptive use, it may be necessary that the quality of care offered at reference centres be even higher than that currently offered. Put differently, though the reference centre was able to shift quality upwards it was not sufficiently far enough to significantly influence subsequent contraceptive use. We saw earlier that the average quality of care received by clients increased from 3.8 units in the health centres to 4.3 units in the reference centres. Our findings indicate that the difference between the two levels of quality needs to be larger to attain statistical significance. In conclusion, since the collection of data presented in this paper, the government of Senegal has embarked on a phased programme of improving health centres nationally. Inputs vary across sites and facilities. Some have undergone whole site training in client oriented provider friendly (COPE), which aims to identify problems and solutions at the facility level, while others have had new buildings, or specific staff underwent various types of training. With all these efforts to improve quality, individuals might be better able to achieve their contraceptive and reproductive goals. Just as rumours and misconceptions have played a part in dissuading users from contraception, there is hope that the converse will be true as well. In other words, diffusion of news of high quality care and services through satisfied users and informal community networks can help. ACKNOWLEDGEMENTS We wish to acknowledge the collaboration and support of Colonel Adama N'doye, Director, Service Nationale de la Sante Reproductive (SNSR). The paper benefited from the insightful comments of John Casterline. Thanks to Gina Duclayan for providing crucial editorial assistance. We also thank Mady Cisse, Heather Clark, Karen Schoepflin, and the data collectors for their assistance. This study was carried out under the Impact Studies Program of the Population Council. The project is one of four field studies designed to document the feasibility of improving quality of care and the effect of improved quality on women's reproductive behaviour. This programme is directed by Anrudh Jain and is being funded by the Rockefeller Foundation, USAID, and the Population Council. An earlier version of this paper was presented at the annual meetings of the Population Association of America meetings, Los Angeles on 23-25 March 2000. NOTES a Some private sector clinics and gynaecologists provided pills, condoms and IUDs, but these were available largely in the urban areas. b In this paper, comparisons will be made between the reference centres and health centres c The available contraceptives are oral pills, depo-provera, IUD, Norplant, condoms, and spermicide, which are supported by USAID. Reference centres are envisaged to provide tubal ligation as well. The drug list comprises of metronidazole, cotrimaxazole, benzathine penicillan and quinine, available under the Bamako Initiative d Agencies include AVSC International (now renamed Engender Health), MSH, JHPIEGO, and the Family Planning Logistics Management Project (FPLM) e Identification of clients who have not returned to the facilities through the MIS and follow-up at home has not yet been fully implemented f The most current policy direction is the creation of an agency, the Service National de la Santé de la Reproduction (SNSR) to further strengthen the delivery of reproductive health services. SNSR is composed of the Office of Maternal and Child Health, and the Office of Family Planning and Adolescents Health and operates under the Ministry of Health. g Other researchers have utilised data from DHS surveys and examined the effects of service availability, readiness of the service environment and access on clients' contraceptive behaviour19 h Dakar region was excluded because it is an outlier in many respects, and Diourbel, Louga, Kolda and Ziguinchor regions because they did not satisfy one or more of the criteria. i The reference centre and health centre closest in size and caseload to it from each of the five study regions were chosen j Only respondents who had given permission for a follow-up interview were followed up. Some respondents were reluctant to be interviewed at home for reasons of privacy, and so were interviewed at the clinics. Those who had no such constraint were interviewed at home. k Some respondents gave wrong addresses and others could not be located. l The mean difference in age between the two groups was about a year and a half at both time points m 15% of the respondents who visited reference centres compared to 4% who visited health centres reported receiving the best possible quality of service, i.e., receiving a quality of care score of 5 out of a possible 5. REFERENCES
Copyright 2003 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh03024t7.jpg] [rh03024t6.jpg] [rh03024t3.jpg] [rh03024t8.jpg] [rh03024t1.jpg] [rh03024t5.jpg] [rh03024t4.jpg] [rh03024t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}