 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 7, No. 2, Aug, 2003 pp. 89-99 Gender Issues in the Prevention and Control of STIs and HIV/AIDS: Lessons from Awka and Agulu, Anambra State, Nigeria Nkoli N Ezumah1 1Department of Sociology/Anthropology, University of Nigeria, Nsukka,
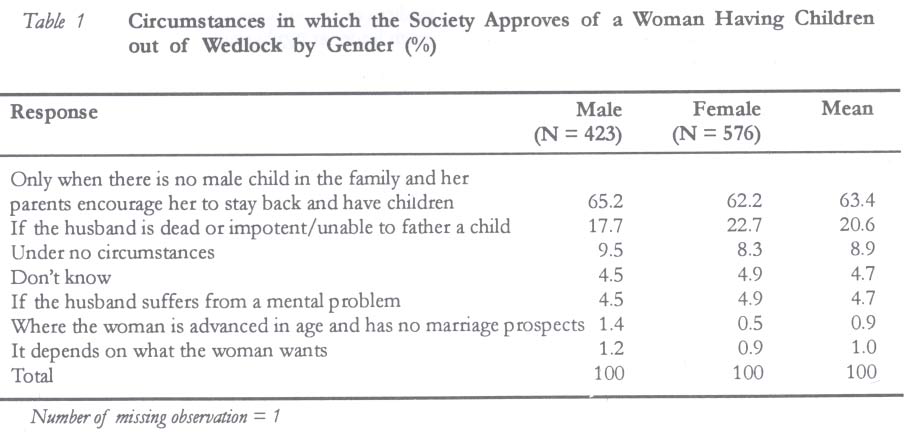
Nigeria Code Number: rh03026 ABSTRACT The study examined perceptions, practices and norms underlying sexuality and gender relations that constrain the prevention and control of STIs and HIV/AIDS. It was carried out among the Igbo of Awka and Agulu in Anambra State of Nigeria. Both quantitative and qualitative methods were used for data collection. Findings indicate that cultural practices that encourage the establishment of sexual networks by men persist in the study communities. Some married women who are not able to achieve pregnancy with their husbands get involved in such networks to have children. Some parents who do not have male children encourage their unmarried daughters to have children out of wedlock so as to perpetuate the lineage. Inequality in gender relations and fear of repercussions constrain women from negotiating safe sex. Sexuality education is, therefore, necessary to improve the knowledge base, perceptions and sexual behaviours of the study communities. Women should be empowered to make informed decisions about sexuality and childbearing. Male responsibility in reproductive health should also be encouraged. (Afr J Reprod Health 2003; 7[2]: 89-99) RÉSUMÉ Questions de genre dans la prévention et la lutte contre les IST et le VIH/SIDA: lessons tirées d'Awka et d'Agulu, Etat d'Anambra, Nigeria. L'étude a examiné les perceptions, les pratiques et les normes qui sous-tendent la sexualité et les relations de genre qui limitent la prévention et la lutte contre les IST et le VIH/SIDA. L'étude a été menée auprès des Ibos d'Awka et d'Agulu dans l'Etat d'Anambra au Nigéria. Pour collecter les données, nous avons employé les méthodes quantitative et qualitative. Les résultats montrent que les pratiques culturelles qui encouragement l'établissement des réseaux sexuels par les hommes, demeurent toujours dans les communautés qui ont fait 'objet de l'étude. Certaines femmes mariées qui n'arrivent pas à devenir enceintes de leurs maris, deviennent impliquées dans de tels réseaux pour avoir des enfants. Certains parents qui n'ont pas d'enfants de sexe masculin encouragent leurs filles célibataires d'avoir des enfants hors mariage afin de prolonger la lignée. L'inégalité dans les relations de genre et la peur des repercussions obligent les femmes à ne pas négocier la sexualité sans danger. L'éducation sexuelle est donc nécessaire pour améliorer la base de la connaissance, les perspectives et les comportements sexuels des communautés qui ont fait l'objet de l'étude. Il faut donner le pouvoir aux femmes qui leur permeltra de prendre des décisions en connaissance de cause sur la sexualité et l'accouchement. Il faut également encourager la responsabilisation de la part des hommes en matière de la santé reproductive. (Rev Afr Santé Reprod 2003; 7[2]: 89-99) KEY WORDS: Gender, sexuality, STIs, HIV/AIDS, prevention, safe sex INTRODUCTION STIs constitute a reproductive health problem for men and women with many complications including infertility. It has been reported that 85% of primary infertility in women and 20% in men in sub-Saharan Africa is due to previous genital tract infections.1 In the case of HIV/AIDS, about 60% of the 33 million infected people worldwide live in Africa.2 In Nigeria, there has been a dramatic increase in the rate of HIV/AIDS infection from 1.8% in 1990 to 5.4% in 1999.3 In some states that constitute the hot spots of Nigeria the rate is 6-10%. 4 Research has established a link between risky sexual behaviour, especially sexual networking, and the transmission of HIV/AIDS. About 80% of infections in Africa are as a result of heterosexual transmission.5 There is a higher rate of infection in women than men, and several factors contribute to this. Gender issues are of prime importance among such factors. Due to gender inequality and women's low socio-economic status, they are less likely than men to exercise control over the timing, frequency and conditions of sex.6-8 The vulnerability of women to STIs and HIV/AIDS is also aggravated by sexual exploitation, coercion, rape and commercial sex work. Cubis9 argues that without considering the impact of gender relations and strategies for dealing with women's low socio-economic status, the distribution of condoms and education will not be effective in dealing with the spread of HIV/AIDS. In addition, ideologies about sexuality tend to predispose men and women to indulge in risky sexual behaviours and unprotected sex. Women are often expected to be passive in sexual relations. Their sexual expression is assumed to be reactive or in response to male advances, whereas men's sexuality is assumed to be active. People's adherence to these notions about sexuality explains why a double standard of sexual morality persists in some societies.10 This has been identified as one of the predisposing factors to STIs in Nigeria.11 The belief that women should be passive in sexual relationships also makes them to be ignorant and misinformed about the sexual behaviour of their husband and the consequences of such actions.12 Gender roles and cultural values related to marriage and childbearing also predispose men and women to STIs and HIV/AIDS. Marriage and childbearing provide social status and respectability for women in Nigeria as in other African countries.13,14 In fact, procreation is perceived as the major role of Igbo women in Nigeria.15 Consequently, the society tends to treat childless women with disdain. Although the increasing phenomenon of "outside wives" who serve as mistresses to married men who are still living with their "inside wives" was attributed to women's quest for materialism,13 such a development could also be related to women's desire to bear children. This paper examines how perceptions, practices and norms underlying sexuality and gender relations among the Igbo constrain men and women from taking appropriate measures to protect themselves as well as their partners from STIs including the HIV/AIDS. THEORETICAL FRAMEWORK The sexuality-gender framework propounded by Dixon-Mueller 7 provides a useful theoretical orientation for the analysis of the effect of gender issues and sexuality in the prevention and control of STIs and HIV/AIDS. She identified four dimensions of sexuality-gender framework, namely, sexual behaviour, nature of sexual acts, social construction of sexuality, and nature of sexual drives and enjoyment. The first dimension, which focuses on sexual behaviour, deals with the issue of timing, duration, number, choice and identity of sexual partners. The conditions that influence the initiation of sexual activities have important influence on peoples' subsequent attitudes and behaviour. In some societies, a double standard of morality exists with respect to gender differences in sexual behaviour. It has been pointed out that sexual relationships between older men and younger women are acceptable in many societies.17 Extramarital relationships by married men are also tolerated in Nigerian communities.16,17 Similarly, the practice of patronising commercial sex workers by married men is often pervasive.10,11 The second aspect focuses on sexual acts. These include the nature, frequency and conditions of choice of sexual partners as well as the types of sexual practices individuals engage in. Dixon-Mueller7 argues that because heterosexual practices tend to be more dominant in societies, the existence of homosexual practices might appear invisible in apparently heterosexual populations. Moreover she raises the issue of certain sexual practices such as oral and anal sex, masturbation, use of devices to enhance sexual pleasure that may have implications for disease transmission and prevention. That dimension also addresses the implications of gender-based violence and coercive sex for disease transmission and unwanted pregnancies. The third dimension, which focuses on the social construction of sexuality, deals with the cultural interpretations and meanings that are ascribed to sexual thoughts and behaviours. These reflect the beliefs and ideas people have about "the nature of the body". Cultural taboos and sanctions are established to control undesirable sexual behaviours of males and females. However, it has been observed that due to cultural inhibitions, the "culture of silence" in sexuality has persisted in some societies among couples and between parents and children.18 In particular, women's compliance with their expected norms in sexual relationships (i.e., passivity in sexual relationships) is often responsible for their inability to participate in meaningful communication about sexuality. Consequently, some women dwell on misinformation and ignorance about the sexual behaviour of their partners and the likely consequences of such actions. Concomitantly, they are not able to protect themselves from infection especially if their partners indulge in multiple sexual networking.12,16The lack of communication about sexuality is aggravated in some societies like Nigeria by the use of poignant lan guage that stigmatises women as disease vectors.1 The fourth dimension refers to sexual drives and pleasures. It deals with how individuals perceive their sex drives and the meanings they attribute to sexual pleasure. The perception that sexual pleasure is desirable for males predisposes them to early involvement in sexual experience. This often starts during adolescence. In the case of women, the expression of sexual pleasure is hardly thought of. However, for many Nigerian women the consideration of sexuality as a source of pleasure still remains beyond imagination.14 Due to the interrelationship between gender, sexual behaviours and practices that enhance the transmission of STIs and HIV/AIDS as demonstrated in this theoretical orientation, one joins in the call for a better understanding of sexual behaviour as well as its determinants in different cultural settings.9,19 Such information would be indispensable in ensuring that culturally specific and appropriate programmes are instituted to bring about desired positive changes in sexual behaviour as a measure towards prevention and control of STIs and HIV/AIDS. MATERIALS AND METHODS The study was conducted in two Igbo communities in Anambra State of Nigeria, namely, Awka and Agulu. Awka is the capital city of the state. The 1991 National Census puts the population of Awka at 58,225 persons, comprising 28,335 males and 29,890 females. On the other hand, Agulu is a rural community situated about 30km from Awka. The 1991 National Census puts the population at 49,310 persons, comprising 23,573 males and 25,737 females. Data were collected from five randomly selected communities - three in Awka (Ifite, Amenyi and Ezioka) and two in Agulu (Obeagu and Nkita-aku). Eight and six enumeration areas (EAs) (based on the 1991 census figures) were randomly selected from Awka and Agulu respectively. Both quantitative and qualitative methods were used for data collection. Survey instruments were administered to a total of 1000 randomly selected respondents, 600 from Awka and 400 from Agulu. The distribution pattern was based on the proportion of the two communities in relation to the total population. The sample distribution ratio (3:2 in favour of women) was a reflection of the male:female ratio in the general population of the two communities. Eighteen focus group discussions (FGDs), made up of 12 in Awka (comprising six female and six male groups) and six in Agulu (comprising three male and three female groups) were administered. The participants were purposively selected to fall within three age groups -15-24 years, 25-44 years and 45 years and above. Other criteria used for the selection of FGD participants included education and occupation. Due to greater migration of young men from Agulu to Awka and other urban areas, it was difficult to get up to six male focus groups of the required age, education and occupational categories at the time of investigation. We therefore had to scale down the number of FGDs in Agulu to three male and three female groups to enhance effective gender comparison of responses. Each focus group comprised 8-10 participants. Sixteen respondents were selected for the in-depth interviews, eight in Akwa (four men and four women) and eight in Agulu (four men and four women). The participants included leaders of organisations, community leaders, youth leaders, teachers, public servants, farmers and housewives. RESULTS AND DISCUSSION Cultural Practices Associated with Childbearing that Predispose Women to STIs and HIV/AIDS Although the Igbo frown at premarital sex,16 the study identified circumstances that the community approves of women having children out of wedlock. About 63.4% of the survey respondents indicated that where a couple does not have a male child, there could be a tendency to coerce one of their daughters to remain unmarried and have male children for the family in order to perpetuate the lineage. Also, 20.6% indicated that if a man dies without having children from his wife, or if he is impotent or unable to father a child, his wife would be encouraged to have a lover with whom she can have children. Both male and female respondents expressed similar views on these issues (Table 1). The establishment of sexual networks by widows and childless women to have children was corroborated by findings from the FGDs and IDIs. A male community leader at Awka referred to the practice as "taking shelter". He explained that through this practice the woman is trying to save herself from the embarrassment and scorn that childless women usually experience in the Igbo society. One of the problems associated with the practice of "taking shelter" was, however, indicated by a respondent as follows:
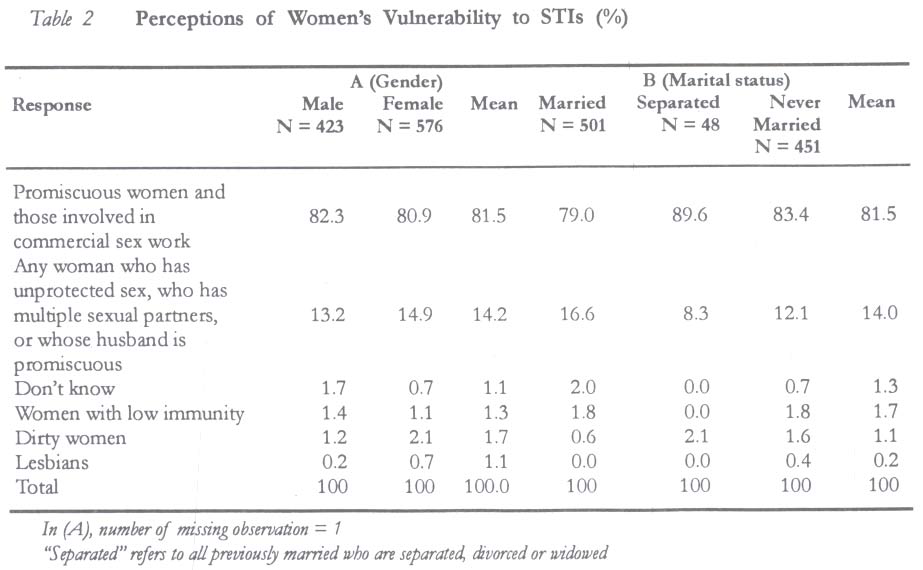
The practice of having multiple sexual partners in order to have children and of couples coercing their unmarried daughters to bear children for their natal families expose women and girls to the risk of contracting STIs including HIV/AIDS. This therefore supports the finding that HIV/AIDS seroprevalence is higher among women of childbearing age in Nigeria.7 Perceptions of People's Vulnerability to STIs Results show that 81.5% of the survey respondents held the view that only promiscuous women and commercial sex workers are vulnerable to STIs. Only 14.2% indicated that any woman who has unprotected sex is at risk of contracting STIs. Male and female respondents held similar views irrespective of their marital status (Table 2). It is important to note that most of the responses from the IDIs and FGDs reflected the ideas expressed by survey respondents. For example, male respondents in the FGDs (25-44 years) at Awka pointed out that only commercial sex workers and unmarried promiscuous women are at risk of contracting STIs. These findings demonstrate that ignorance and misinformation about sexual relationships are still serious issues to be addressed in any effort to prevent STIs and HIV/AIDS in these communities. This is because married women who might not be promiscuous but whose husbands might be having unprotected sex with multiple partners are also at risk of contracting STIs. In fact, it has been pointed out that the single most important risk factor for women in the transmission of HIV/AIDS in sub-Saharan Africa is being married.20 However, 81.6% of male respondents rightly indicated that any man who patronises commercial sex workers or has many sexual partners is at risk of contracting STIs. To buttress that point, a male respondent in an FGD (45 years and above) at Agulu said:
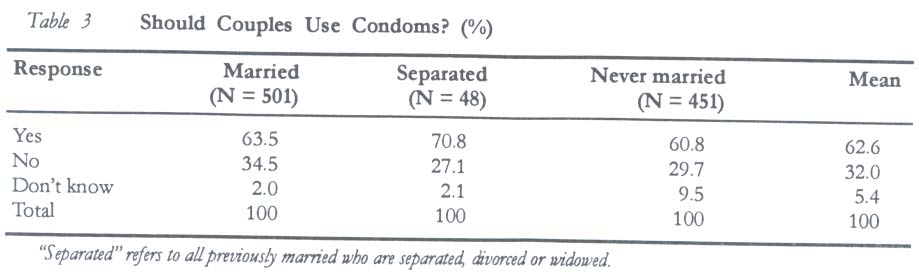
PERCEPTIONS OF THE USE OF CONDOM BY MARRIED COUPLES Some 62.6% of the respondents agreed that married couples could use condoms (Table 3) to avoid unwanted pregnancies and for child spacing. Among those who disagreed that couples should use condoms, 52.6% said married couples should accept the number of children God has given them because condoms are meant for unmarried people who desire to avoid pregnancy. About 31% expressed their fears that the use of condoms could create such problems as infection, bleeding, barrenness and cancer of the womb for women. The remaining 16.4% indicated that if women know their safe periods they and their partners would be in a position to practice periodical abstinence as a natural method of family planning. When women were asked if they would discuss the use of condoms with their husband if they suspect that he indulges in extramarital affairs, only 54% of the married women said they would do so. Several reasons were given by those who said they would not discuss the use of condoms with their husband even when they suspect that he has multiple sexual partners. About half (49.6%) said such a discussion would encourage them to have outside lovers, 24.8% said they did not know about the use of condoms, and 12.4% said their husbands would not listen to them and that it might even worsen the situation. Seven per cent said it is not their business to make such suggestion while 6.2% said it is immoral to use condoms. These responses also highlight the fact that fear of repercussions constrains women from negotiating safe sex practices. The views expressed by participants at the FGDs and IDIs on the use of condoms reflected both inter-generational gap and gender differences. A female vice principal (above 50 years) in Awka said it is all right for a woman to advise her husband to use condoms if she finds out that he is unfaithful. At the same time, she quickly pointed out thus:
Similarly, a retired female headmistress (above 60 years) in Agulu said although a woman could suggest the use of condoms to her husband, in practice men are those who would be expected to bring up such issues for discussion because of their constant urges for sex. Some of the males in the IDIs, both at Agulu and Awka, were opposed to the idea of a woman suggesting the use of condoms to her husband regardless of the circumstances. For example, a male youth leader at Agulu said:
It was only in the male FGDs (15-24 years) in both communities that there was a consensus that women could suggest the use of condoms to their husbands. In fact, one of them indicated:
On the other hand, a male in one of the FGDs (25-44years) at Awka insisted:
Similarly, a male respondent in an FGD (25-44 years) at Agulu said:
These responses show that male control is a fundamental problem confronting women in exercising their rights to protect themselves from infection. The fact that the opposing views were expressed by some men and women clearly reflect the prevailing notion that males should have control of heterosexual relationships. For many of them the issue was who has the prerogative to control decision-making in sexuality. This finding corroborated reports from other studies, which identified lack of power as a serous impediment to women's ability to negotiate safe sex.21, 22 People's Perception of Whose Responsibility it is to ensure that one does not contract STIs A majority of the respondents (86.4%) indicated that both men and women are responsible for ensuring that one does not contract STIs. Only 10.7% indicated that it is the responsibility of men, 2.7% said it is the responsibility of women, while 2% had no clear views on the issue. These views were supported by responses from the IDIs and FGDs. A male community leader at Awka argued:
A male teacher in the IDI at Awka pointed out:
Similarly, women at the FGD for those 45 years and above at Agulu pointed out that if a husband and wife are able to avoid outside lovers, they would have no problems of contracting STIs. Some respondents said it is the responsibility of the man to ensure that he and his wife do not contract STIs. Sixty eight per cent of the women and 55.6% of the men who gave this response attributed their view to the prevalence of male promiscuity. A female respondent in one of the FGDs (15-24 years) at Awka added that males tend to be promiscuous because "there is no punishment for them for flirting". These responses underscore the need to emphasise male responsibility in ensuring the sexual health of their partners. Responses by those who said it is the responsibility of women to ensure that couples do not contract STIs demonstrate how the prevailing language of sexuality stigmatises women. About 28.6% of the men and 16.7% of women perceived women as disease vectors. Also, more men (35.7%), compared to women (16.7%), felt that it is the responsibility of women to monitor their husbands' activities in order to know whether they are indulging in extramarital affairs. Similarly, a male youth leader in the IDI at Agulu argued that it is the responsibility of women (to ensure that couples do not contract STIs) because they tend to be promiscuous. He emphasised:
Perceptions on whether it is Appropriate for Women to Refuse to have Sex with their Husbands when they do not desire it, or when they feel that it is not Safe Findings reveal that 81.6% of respondents agreed that it is appropriate for women to refuse to have sex with their husband if they do not desire it. They said the woman might be indisposed due to ill health, she may be weak, pregnant, menstruating or still weaning an infant (78.3%). Others said she could refuse if she knows that her husband is having an extramarital affair (10.4%), she might be unhappy with the husband especially if he is not taking good care of her (7.0%), if the woman does not want to be pregnant (3.3), or if she is fasting or meditating. The fact that only 10.4% raised the issue of fear for disease transmission shows that many of the respondents are still ignorant of the adverse consequences of the sexual behaviours of their partners. This highlights the gravity of the danger of disease transmission that risky sexual behaviours of husbands could pose on their wives. Similar responses were obtained from IDIs and FGDs as with the questionnaire survey. Some of the respondents said a woman cannot refuse to have sex with her husband because they believe the males should have control over female sexuality and that women should remain passive in sexual relationships. A male youth leader in the IDI at Agulu said:
Similarly a female Christian woman leader in Agulu said if a woman refuses to have sex with her husband and the later starts flirting she is to be blamed for his action. A male participant in one FGD (45 years and above) at Awka also said:
Even a female in the FGD for the 45 years and above group at Agulu said:
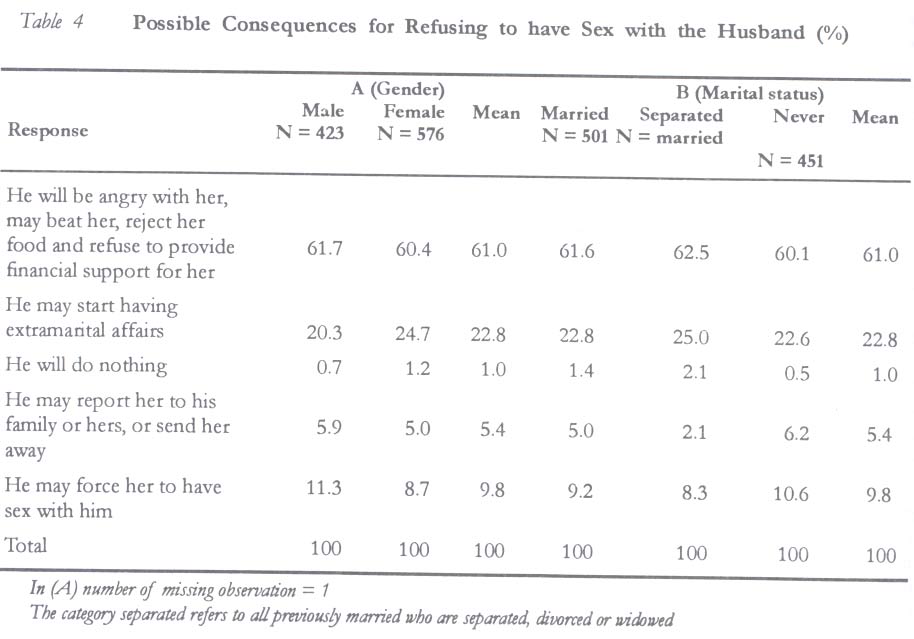
Possible Consequences of Refusing to have Sex with the Husband Majority of the respondents said the man would be angry with his wife if she refuses to have sex with him, he may also beat her, reject her food, refuse to provide financial support for her, and he may start having extramarital affair. These responses were consistent among both men and women and among the married and unmarried (Table 4). The responses were also corroborated by participants in the FGDs and IDIs. Participants at the female and male FGDs (45 years and above) in Awka and Agulu specifically emphasised that a husband who has been denied sex by his wife would become suspicious. This could lead to fighting and quarrelling, making the man to deny her of housekeeping allowance. One of the females pointed out that Arefusal is giving the husband a license to seek an outside lover. A female vice principal in the IDIs at Awka responded:
A female leader of a Christian women organisation in the IDIs at Agulu also emphasised that refusal of sex by a wife could lead to trouble in the home. A male teacher at Awka pointed out:
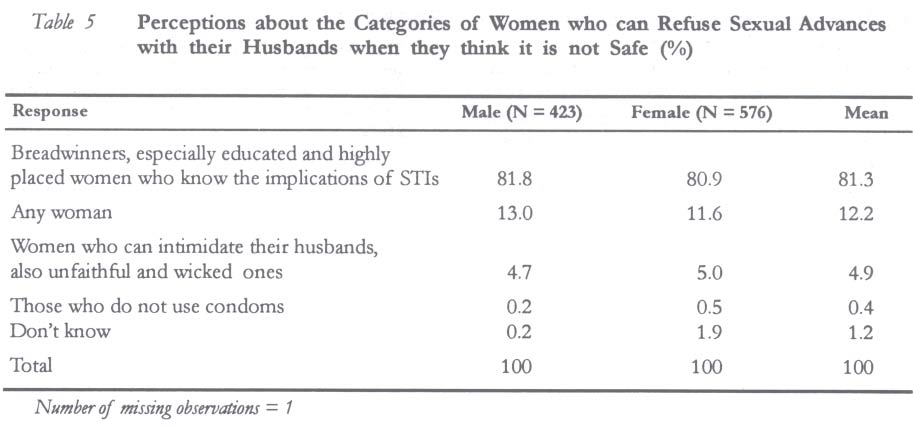
These responses demonstrate that fear of repercussions still poses a serious constraint to women's ability to exercise their rights in negotiating sexual relationships with their spouses. There was a consensus among both males and females, indicating group norms that emanated from their socialisation, a situation in which female passivity as well as male control in sexuality is still predominant. The persistence of such views is a serious impediment to social change. This consequently continues to pose a threat to the prevention of STIs and HIV/AIDS among married women in the study communities. Respondents' Perceptions about Categories of Women who would be able to Refuse Sex with their Husbands when they Suspect that it is not Safe Majority (81.3%) of the survey respondents felt that mostly breadwinners, especially educated and highly placed women who know the implication of STIs, would be able to refuse sex with their husbands when they suspect that it is not safe (Table 5). The importance of economic independence in enhancing women's ability to be assertive and to refuse sex when it is not safe was also highlighted in the FGDs and IDIs. A female teacher in the IDI at Awka indicated that women who cannot refuse sex are immature wives who do not know their rights. She identified other categories such as illiterates, the jobless who are dependent on their husbands, and those who could be easily intimidated by their husbands among those who cannot refuse their husbands' sexual advances. Female participants in the FGDs (15-24 and 25-44 years) at Agulu and Awka emphasised the issue of fear and intimidation. One of them said: The inability of women to refuse sex is due to fear of violence on their husbands' part because some men beat fear into their wives. So, because of fear the women may not voice out even when they suspect that their men may be infected. CONCLUSION AND RECOMMENDATIONS This paper makes some important contributions to knowledge and research in reproductive health issues. It identified the cultural practices, perceptions and norms about gender relations and sexuality that influence the sexual behaviours of men and women, thus increasing their chances of contracting STIs including HIV/AIDS in the communities studied. Findings from the study can be summarised as follows:
These findings raise important policy issues that must be addressed in any effort to prevent the spread of STIs and HIV/AIDS. The intervention strategies suggested are two-fold. The first entails the provision of culturally specific and appropriate sexuality educational programmes in these communities to improve their knowledge and perceptions of sexual behaviours. Such programmes should highlight the reproductive health hazards involved in the harmful cultural practices that encourage the involvement of men and women in risky sexual behaviours. Specifically, women should be empowered to make informed decisions about their sexuality and childbearing. Male responsibility in reproductive health should also be encouraged in order to promote the sexual health of men and the wellbeing of their partners. The second is the need to embark on empowerment strategies that would deal with issues of male dominance in sexual relationship, women's passivity and the fear of reprisals, which arise as a result of women's low socio-economic status. Women should be educated on the need to improve their self-image, they should be given opportunities for skills training and assisted to engage in income generating activities that would reduce their dependence on men. If women are empowered economically they will be better able to overcome the fear of reprisals when they need to take decisions on issues that affect their sexuality. ACKNOWLEDGEMENT The author acknowledges the support of the John D. and Catherine T. MacArthur Foundation, which provided fund for the project under the Fund for Leadership Development (FLD) in Nigeria. The support of field staff in data gathering is also acknowledged. REFERENCES
Copyright 2003 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh03026t2.jpg] [rh03026t5.jpg] [rh03026t4.jpg] [rh03026t3.jpg] [rh03026t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}