 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
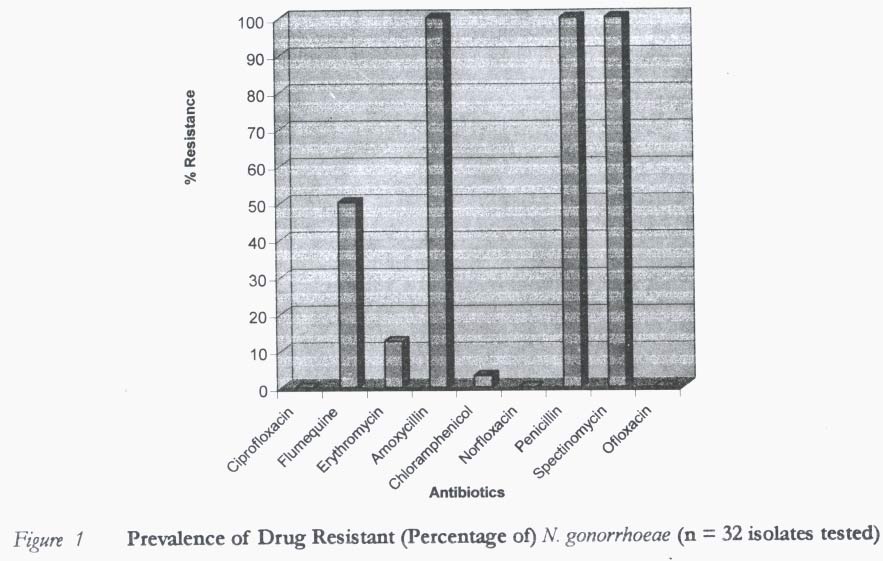
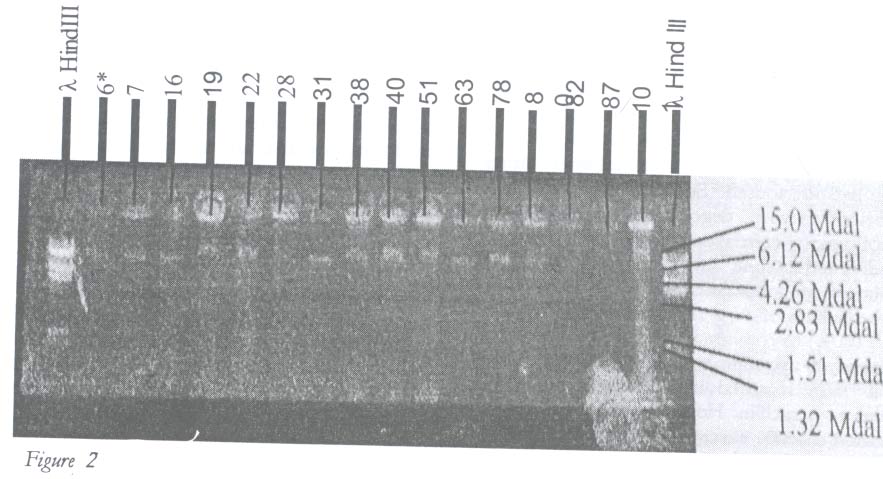
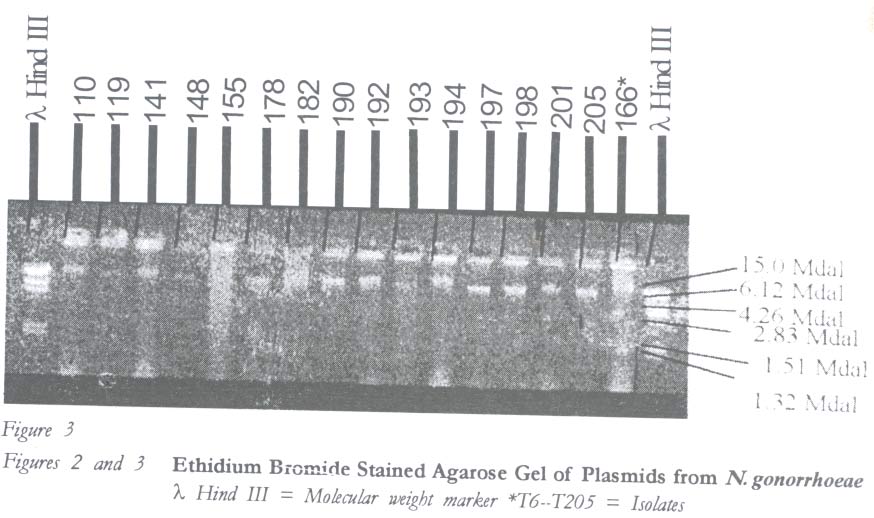
African Journal of Reproductive Health, Vol. 7, No. 2, Aug, 2003 pp. 100-105 Laboratory Report Antibiogram and Plasmid Profiles of Neisseria gonorrhoeae Isolates from Cameroon: Useful Tools for Epidemiological Survey RN Ndip1, G Aroke1, W Mbacham2, LM Ndip1 and VPK Titanji1 Correspondence: Dr Roland Ndip, Biotechnology Centre, Department of Life Sciences, Faculty of Science, University of Buea, P.O. Box 63, Buea, Cameroon Tel: 237 752 68 84 Fax: 237 332 22 72 . E-mail: ndip3@yahoo.com Code Number: rh03027 ABSTRACT A prospective laboratory-based investigative study was carried out on clinical isolates of N. gonorrhoea to determine their antibiotic susceptibility patterns and plasmid profile using standard microbiological and molecular techniques. All the 32 isolates studied showed total resistance to penicillin, spectinomycin and amoxycilin. On the other hand, susceptibilities of 100%, 98.6% and 98.6% were noted for ciprofloxacin, ofloxacin and norfloxacin respectively. Thirty (93.8%) of the 32 isolates were found to harbour plasmids of molecular weights ranging from 9.2 to 25.2Mdal. Three distinct groups of N. gonorrhoea isolates were identified based on the molecular weights of the plasmids, namely, group one (9.2Mdal), group two (12.6Mdal) and group three (25.2Mdal). These results suggest that different strains of N. gonorrhoea may be circulating in Fako Division of Cameroon, a finding that is of clinical and epidemiological significance. (Afr J Reprod Health 2003; 7[2]: 100-105) RÉSUMÉ Profils plasmidiques et antibiotiques des isolats de Neisseria gonorrhoeae du Cameroon: outils nécessaires pour l'enquête épidemiologique. Une étude prospective basée dans le laboratoire a été menée sur des isolats cliniques de N. gonorrhoeae pour déterminer leur modèles de susceptibilité antibiotique et leurs profil plasmidique à l'aide des techniques moléculaires et microbiologiques standards. Tous les 32 isolats que nous avons étudiés ont révélé une résistance totale à la pénicilline, à la spectinomycine et à l'amoxicilline. Par contre, on a noté des susceptibilitiés de 100%, 98,6% et 98,6% pour la ciprofloxacine, l'ofloxacine et la norfloxacine respectivement. On a découvert que 30, soit 93,8% des 32 isolalats, contenaient des plasmides de poids moléculaires allant de 9,2 à 25,2 Mdal. Nous avons identifié trois groupes distincts d'isolat de N. gonorrhoeae à partir des poids moléculaires des plasmides, c'est-à-dire le groupe un (9,2 Mdal), le groupe deux (12,6 Mdal) et le groupe trois (25,2 Mdal). Ces résultats affirment que des souches de la N. gonorrhoeae sont peut-être en circulation dans la région de Fako au Cameroun, une trouvaille qui a une signification à la fois épidémiologique et clinique. (Rev Afr Santé Reprod 2003; 7[2]: 100-105) KEY WORDS: Neisseria gonorrhea, antibiogram, plasmid profile, Cameroons INTRODUCTION Neisseria gonorrhoeae is the etiologic agent of gonorrhoea, one of the major causes of infertility and sterility in males and females.1 There has been an increasing number of reports in recent years on the emergence of resistant strains of N. gonorrhoea to newer antibiotics previously used for treatment.2 It has also been documented that bacteria that show resistance to certain antibiotics contain the R-plasmid, which code for -lactamase production.3 A single plasmid may carry separate genes for resistance to several antibiotics. The plasmid may be dissociated into the resistance transfer factor, carrying the genes governing the intracellular transfer, and the R determinant, carrying the resistance genes. Therefore, these plasmids have different patterns, and changes in old patterns are occurring.4 Consequently, the antibiograms of different isolates may differ according to the different plasmids they harbour. Plasmid profile analysis is known to aid in the identification of a source of infection, differentiating strains or evaluating efficiency of control measures.5 Different types of plasmids have been extracted from N. gonorrhoea. They include the TEM-1 -lactamase, the cryptic plasmid and the conjugal plasmid.4-6 The 4.4Mdal plasmid first isolated from South East Asia and the 3.2Mdal plasmid originating from Africa code for the TEM-1 -lactamase plasmid. Other plasmids of molecular weights 2.9Mdal, 4.1Mdal, 6.2Mdal have also been reported to code for the same TEM-1 -lactamase. The cryptic plasmid, which remains to be fully characterised,7 has a molecular weight of 2.6Mdal, and a conjugal plasmid of molecular weight 24.5Mdal had been isolated from many localities including Cameroon.8 As a result of the widespread resistance to various antibiotics used for treatment, it is necessary to constantly determine the susceptibility pattern of various antibiotics to the isolates for proper management of infections caused by the organism. It becomes pertinent, therefore, to undertake a study on plasmid profiles and antibiotic susceptibility of N. gonorrhoeae isolated from a cohort of workers of the Cameroon Development Corporation (CDC), a milieu that is associated with high prevalence of sexually transmitted diseases (STDs). MATERIAL AND METHODS Study Setting and Design Study samples for this prospective laboratory investigative study were obtained from both symptomatic and asymptomatic patients attending the CDC central clinic in Tiko, Cameroon. The CDC is the second largest employer of labour after the government of Cameroon and it spans most of the Fako Division in the South West Province with several estates. Workers from these estates consult regularly at the CDC central clinic as outpatients three times a week. This population is characterised by high rate sexual promiscuity and unhygienic living conditions, which may be attributed to low level socio-economic status, education and poverty. As a result of these, gonorrhoea and other STDs are very common amongst the population. Bacteriological Culture and Identification Vaginal and urethral exudates collected from symptomatic and asymptomatic patients of both sexes were inoculated on Thayer Martin agar, incubated at 37oC overnight under increased CO2 concentration (Genbag CO2, biomerieux, France). The isolates were identified based on colonial morphology, gram staining, oxidase test and sugar fermentation, as previously reported.9 Antibiotic Susceptibility Testing Antibiotic susceptibility test was carried out on all isolates using the Kirby Bauer disk diffusion method.10 Briefly, small inoculum of each pure bacterial isolate was emulsified in 3ml sterile physiological saline solution in bijou bottles and the density compared to a barium chloride standard (0.5McFarland). A sterile cotton swab was dipped into the standard solution of bacterial cultures and used to inoculate the Mueller-Hinton agar (Biotec, England). The inoculated plates were allowed to dry, and the antimicrobial disks with the following drug contents were used: ciprofloxacin (5mcg), flumequine (4mcg), norfloxacin (10mcg), spectinomycin (30mcg), ofloxacin (10mcg) and penicillin (1iu). The plates were incubated for 24 hours at 37oC under increased CO2, and zones of inhibition were compared with standard. Determination of Plasmid Profiles Cell Harvesting Bacterial cells were harvested as earlier described,11 with slight modifications. Briefly, 5ml of Luria-Bertani (LB) broth was poured into a testtube. Fifty μg/ml of penicillin was added to the LB broth and inoculated with a colony of the pure bacteria culture. The tube was then incubated overnight in an incubator shaker (Innova TM 4000, New Brunswick Scientific Co., Edison, USA) at 200rpm and a temperature of 37oC. Then 1.5ml portions of the broth culture was put into eppendorf tubes and centrifuged at 14,000rpm for 20 seconds to pellet the cells. Cell Lysis and Plasmid Isolation The cells were lysed using alkali as previously described.11 Briefly, the pelleted cells were re-suspended in 100μl TE buffer and allowed to sit for five minutes at room temperature. Two hundred microlitre of NaOH/SDS (cell lysis solution) were added to it and mixed. The mixture was placed on ice for five minutes and spun. The nucleic acid was precipitated with 95% ethanol and the mixture spun for one minute to pellet the plasmids. The pellet was suspended in 20ml TE buffer and stored on ice until use. Plasmid Analysis One per cent agarose gel (SIGMA-Aldrich, GmBH, Germany), prepared following a previously reported scheme,11 was used for the analysis. To each tube containing 10μl plasmid sample, 4μl of loading buffer consisting of bromophenol blue (0.25%), xylene cyanol (0.25%), Ficoll (15%) and EDTA (0.02M) was added. They were mixed and loaded into the wells. The first and last wells of the gel were loaded with a known β Hind III molecular weight marker, and the other wells with the various isolates. Electrophoresis in a horizontal system was carried out at 100V and 90A. After 1 1/2 hours of run, plasmid bands stained with ethidium bromide were visualised on a UV (300nm) transilluminator (BIOMETRA T13, Germany) and the gel photographed. RESULTS Figure 1 shows the antibiotic susceptibility results. All the 32 isolates tested were found to exhibit total resistance (100%) to penicillin, amoxycillin and spectinomycin respectively. However, it was also interesting to note that all the isolates (100%) were sensitive to ciprofloxacin, and most (98.6%) were sensitive to ofloxacin and norfloxacin. Out of the 32 isolates, 30 (93.8%) were found to harbour plasmids of molecular weight ranging from 9.2 to 25.2Mdal. Figures 2 and 3 show that the isolates could be classified into three groups based on the weight of the plasmids they contain. Two of the isolates, T101 and T166, had plasmids with molecular weight of 25.2Mdal, while nine (T19, T22, T28, T38, T40, T51, T192, T194, and T201) had plasmids with a molecular weight of 12.6Mdal. Lastly, 19 isolates (T6, T7, T16, T31, T63, T78, T80, T82, T110, T119, T141, T148, T178, T182, T190, T193, T197, T198 and T205) had plasmids with a molecular weight of 9.2 Mdal. Further analysis revealed that those with molecular weight 25.2Mdal were sensitive to only two drugs (ofloxacin and ciprofloxacin) while those with molecular weight 12.6Mdal were sensitive to at least three of the following drugs: ciprofloxacin, ofloxacin, norfloxacin and chloramphenicol. About 49% of the isolates that were sensitive to flumequine had molecular weight 9.2Mdal. DISCUSSION N. gonorrhoeae remains a major cause of infertility and sterility in both males and females. The emergence of strains that are resistant to commonly used drugs remains a significant problem especially in developing countries where drugs are constantly abused.2 Several authors3,12-15 have reported varying degrees of success with ciprofloxacin, ceftriaxone, penicillin, aminoglycosides, tetracycline and spectinomycin in the treatment of gonorrhoea. In the present study, all the isolates of N. gonorrhoea were totally resistant (100%) to commonly used drugs like spectinomycin, amoxycillin and penicillin. Kyungwon et al16 also reported total resistance of their strains to penicillin. However, Van Dyck et al13 reported a 100% susceptibility of their isolates to spectinomycin. Similarly, Kyungwon et al16 reported a 100% success rate with their isolates in Korea. This drug was first used on a wide scale in Korea and in the Philippines in 1981 as the primary drug for the treatment of gonorrhoea. In a study in Lagos, Nigeria, Obi et al3 reported 44.4% susceptibility of their isolates to penicillin and amoxycillin respectively. When compared to those of other authors, the discernible disparity of susceptibility rates noted in the present study could be attributed to the fact that these drugs are relatively cheap in our environment. They are readily available to the population who tend to abuse them and, thus, spiralling the emergence of resistant strains against the drugs. Although we did not determine if our strains were β-lactamase positive, we also speculate that this could have been responsible for the high levels of resistance noted. The resistance noted for penicillin could also be related to an alteration of penicillin-binding proteins. Interestingly, susceptibilities of 100%, 98.6% and 98.6% were reported for ciprofloxacin, ofloxacin, and norfloxacin respectively. The quinolones are very active against the gonococci and are recommended for the treatment of gonorrhoea in the United States of America.17 However, in their study in Dhaka, Bangladesh, Bhuiyan et al18 reported 61.7% sensitivity of their isolates to ciprofloxacin. Similarly, Knapp et al19 noted that the proportion of strains exhibiting decreased susceptibility to ciprofloxacin were approximately 36%, 54% and 22% in Hong Kong, the Philippines and Thailand respectively in 1994-1995. The difference in these results could be attributed to the fact that our isolates might have lost the genes for resistance to this drug, or probably have never acquired the genes which those in Dhaka had. Several studies have related drug resistance in N. gonorrhoeae to plasmids7,18-20, with plasmids of sizes ranging from 2.6Mdal to 27.2Mdal commonly incriminated. A previous report18 documented that a 4.4Mdal plasmid was common to Asian strains, and a 3.2Mdal to Africa. Further analysis by these investigators revealed that the 3.2Mdal plasmid was also prevalent in the Philippines. This may suggest that the 3.2Mdal plasmid is spread as a result of frequent travelling, revealing the need for frequent monitoring of plasmid profiles as a guide for epidemiological surveillance. In the present study, plasmids of sizes ranging from 9.2Mdal to 25.2Mdal were noted. Most of our isolates had plasmids of weight 9.2Mdal and were resistant to amoxycillin, penicillin, spectinomycin and flumequine. Two of our isolates had the conjugal plasmid with molecular weight 25.2Mdal. This plasmid has been reported7 in other regions of the world including Cameroon, and is thought to confer resistance to a range of antibiotics including the penicillins, sulphonamides and cephalosporins. A significant and interesting finding in this study is the fact that plasmid profiles revealed three groups of N. gonorrhoeae isolates in terms of the plasmids. This indicates a possibility of the existence of different strains of the organism in Fako Division in particular and the South West Province of Cameroon in general, and as such may serve to explain why there are difficulties in the treatment of diagnosed cases so far. In conclusion, our study has revealed that ciprofloxacin, ofloxacin and norfloxacin could be useful in the treatment of cases of gonorrhoea in our environment. Furthermore, plasmid profile analysis could serve as a useful tool for epidemiological investigations, as three different groups of N. gonorrhoeae were identified based on molecular weights of the plasmids. ACKNOWLEDGEMENT We wish to thank the Universities of Buea and Yaounde I for equipment and some reagents put at our disposal. We are also grateful to the CDC for letting us use their clinic and to Mr. A.A. Ewang, laboratory technologist at the clinic, for his technical assistance. REFERENCES
Copyright 2003 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh03027f3.jpg] [rh03027f2.jpg] [rh03027f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}