 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
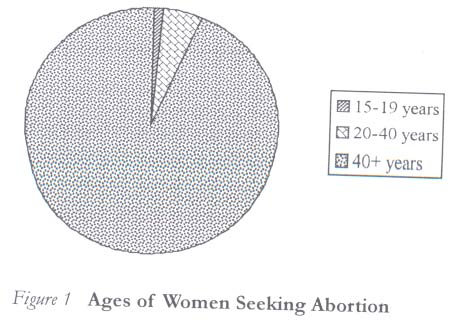
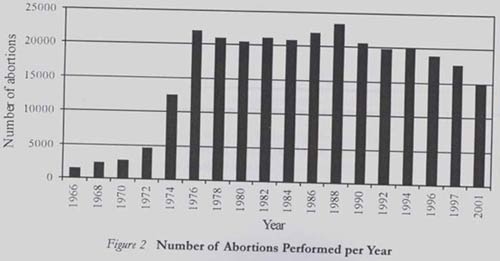
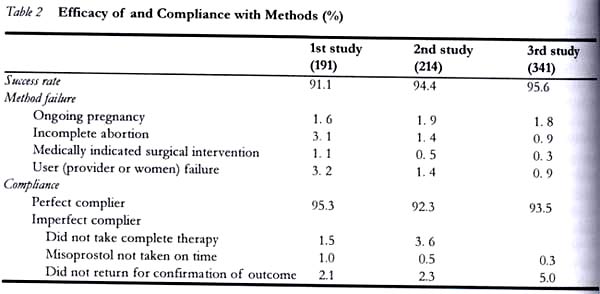
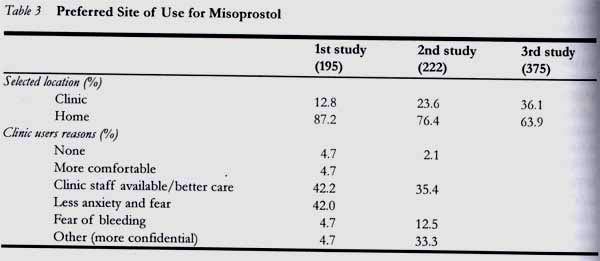
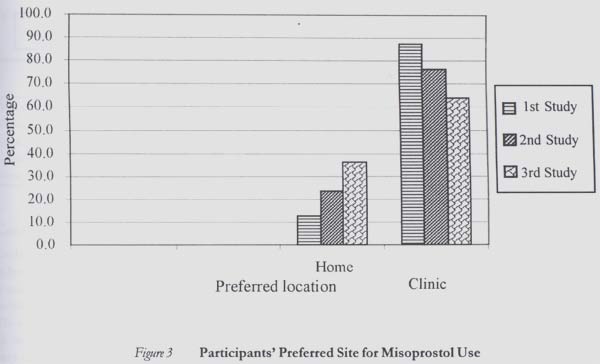
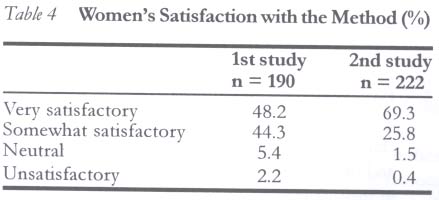
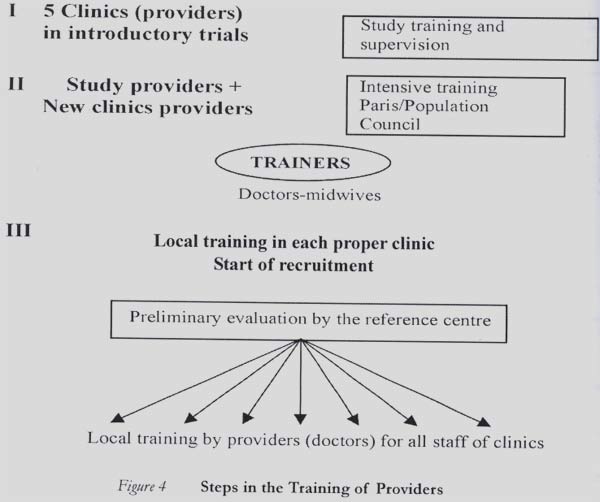
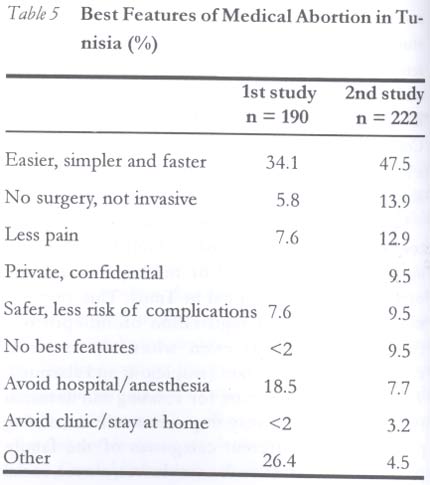
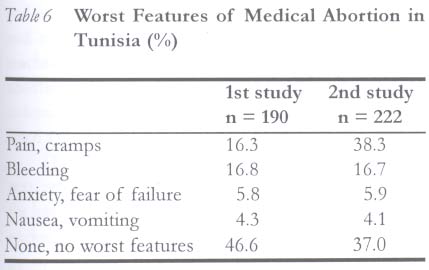
Medical Abortion: The Tunisian Experience Selma Hajri Correspondence: Dr Selma Hajri, Endocrinologist - Reproductive Health, Office National de la Famille et Population - Tunisia, 1 rue de la mosquée Marsa Plage 2070, Tunis, Tunisia. Tel: 216-71-748 371 (Office), 216-71-232-053 (Residence), 216-98-303-111; Fax: 216-71-728530; E-mail: selmahajri30@hotmail.com selmahajri@graffiti.com Code Number: rh04011 Abstract This paper reports the Tunisian experience of medical abortion. The project started in 1998 with a small introductory study at the obstetric and gynaecology department of a university hospital and was later extended step by step to other family planning and public health centres that provided abortion services. The study was first conducted on 264 women using the modified regimen of 200mg mifepristone, followed 48 hours later by 400µg misoprostol in women seeking pregnancy of maximum 56 days of amenorrhoea. This gave a success rate of 91.1%. Results from further studies in other locations showed increasing success rates of 94.4% and 95.6%, with high acceptability and satisfaction among users and providers. The registration and effective introduction of medical abortion was quite rapid. Following successful conduct of the pilot study, intervention programmes were designed and implemented to improve the capacity of providers in providing safe medical abortion. (Afr J Reprod Health 2004; 8[1]:63-69) Key Words: Medical abortion, Tunisia, mifepristone, misoprostol, simplified regimen Résumé L'avortement médical: l`expérience tunisienne. Cet article rapporte l`expérience tunisienne de l`avortement médical. Le projet a commencé en 1998 avec une petite étude d`initiation dans le Département de l`obstrétique et gynécologie d`un centre hospitalier universitaire. Plus tard, l`étude a été élargie pour couvrir d`autres centres de planification familiale et centres de santé qui rendent des services d`avortement. L`étude a été menée la première fois au sein de 264 femmes en utilisant le régime modifié de mifepristone 200mg, suivi 48 heures plus tard du misoprotol 400pg chez les femmes qui recherchaient la grossesse du 56 jours maximum d`aménorrhée. Ce qui a donné un taux de succès de 91,1%. Les résultats d'études supplémentaires dans d`autres endroits ont montré des taux croissants de succès de 94,4% et 95,6%, des résultants qui ont eu une acceptabilité et une satisfaction élevées parmi les usagers et les fournisseurs. L`enregistrement et l`introduction de l`avortement médical étaient bien rapides. Suite au succès de cette étude pilote, des programmes d`intervention ont été élaborés et réalisés afin d`améliorer la capacité de fournisseurs en assurant l`avortement médical sans risque. (Rev Afr Santé Reprod 2004; 8[1]:63-69) Introduction Tunisia is a small country located in North Africa. By location, it is an African country, but also part of the Arabo-Islamic world. It has a history of the influence of several cultures and civilisations that invaded and occupied the country until its independence. The coast of Tunisia is less than 14km from Italy, a European country. Its history and geographical location are partly responsible for the modern approach to family planning and abortion that is experienced in the country. This is in contrast to the practice in most other Islamic countries. Abortion was integrated into the national family planning programme of Tunisia in 1967 with restricted indications. It was legally provided and performed in the first trimester for women who already had five or more children; the mean number of children per woman in Tunisia then was more than seven. Family Planning Association was also created in the same year. In 1973, abortion was legally provided for almost all indications in the first trimester since the creation of the first office of the National Family Planning. From this date, surgical abortion was practiced all over the country and was provided free in all health care centres that had the facilities to perform the surgical procedures.2 Access to abortion was considered as part of women's rights. They were free to manage their pregnancies and make their own decisions. Access to abortion was realised progressively and two conditions were unavoidable: (1) abortion must be procured before the end of the first trimester of pregnancy (12 weeks), and (2) it must be done by qualified practitioners in appropriate medical units. Family planning clinics were also allowed to provide surgical abortion with certain restrictions. All these conditions made access to abortion easy and free but also safe. It produced an impressive increase in the number of abortions procured from 1974, with a great majority of married women aged betwen 20 and 40 years (Figure 1). However, 15 years after the number of abortion cases per year became stable. From 1999, the need for abortion decreased significantly to 15,000 cases per year.3 With the expansion of family planning and contraceptive methods (prevalence increased to 50% in 1984 and reached 70.5% in 1999), Tunisian fecundity fell to 2.08, and the need for abortion decreased progressively (Figure 2). Even if surgical abortion was done under appropriate conditions with few side effects, intro-ducing medical abortion was a logical and expected step in improving reproductive health services. As soon as RU486 was introduced in France, Tunisian family planning centres showed interest in testing its efficacy. The first trial began in 1994 as part of a multi-centre study of the WHO. In 1998, when we began the introductory trials, 20,000 abortions were performed per year in public health structures.3 History of Medical Abortion in Tunisia After four years multi-centre introductory trials in over 8,000 women, the Tunisian Ministry of Health authorised the use of mifepristone for medical abortion including all other medical indications authorised in Europe. Medical abortion began in Tunisia in 1994 with a pilot study, which was part of the WHO multi-centre study. The first Population Council study began in 1998. It has continued till now with more than 800 cases and was conducted in five centres throughout the country. At the beginning of the study, Roussel Laboratory was not interested in introducing medical abortion in non-European countries, and we had to wait until 1997 when the Population Council showed interest in collaborating and conducting introductory trials on medical abortion in Tunisia with the aim of introducing the methods in the country. The trials were first carried out in Tunis, the capital of Tunisia, in two sites (the Department of Obstetrics and Gynaecology of a university teaching hospital and a family planning clinic). Both sites had experienced more than 3,000 abortions per year. The trials were then extended to other urban sites. On these studies we had new objectives and tried to explore the easiest protocol giving high efficacy rates and some particular aspects like the social profile of young Islamic Tunisian women (pregnant and unmarried). We also tested our ability as providers and teachers to extend the method to new clinics and to train new providers. At the same time we focused on registering the drug. This was done in collaboration with, and encouragement of, the head of the ONFP and a few key persons, especially the obstetrics and gynaecology department of the university hospital, who were convinced of the efficacy and innocuousness of the method and its usefulness for Tunisian women. The French protocol (600mg mifepristone + 400µg misoprostol) was the registered regimen but the ONFP adopted the revised simplified protocol (reduced doses of 200mg mifepristone + 400µg misoprostol) based on literature4 and our local results in the introductory trials.5,6 In 2002 the use of medical abortion with mifepristone was already widely practiced in Europe and Asia, but in Africa only Tunisia and South Africa had the drug approval, and only Tunisia had started introducing the method. After approval, we started a third study exploring our ability to extend the method to other clinics, and to train providers. So we extended to the other urban sites. A fourth trial then followed with greater zeal and ambition to introduce the method in the sub-urban and rural areas. While trying to integrate medical abortion into family planning activities, we decided to use the progressive step-by-step approach. We started with 10 clinics in six cities within the country with the help of the family planning centres of training. Looking at the results of these successive studies, we noticed that the age of pregnant women reduced significantly from the first to the third study. Another interesting point was that in the last study the majority of women had never previously experienced abortion. (Table 1) The efficacy rate also changed significantly in the studies. From the beginning we obtained an acceptable efficacy rate of 91.1%, and this increased through the studies. We attained the European efficacy rate of about 97% during the third study, with very good compliance to the protocol of medical abortion. The women felt that the method was very simple and easy, and about 40% of them did not complain of any negative side effects (Table 2). Almost all the women in the three studies preferred home use of misoprostol for various reasons (Table 3 and Figure 3). Satisfaction of women with this method was as high as 92.5% in the first study and 94.1% in the second one. Unsatisfied women were significantly lower, even less than the failure rate (Table 4). (Figure 4) It took about two years after registration to start the use of medical abortion in Tunisia because there was not enough motivation and conviction by decision-makers to make the method available and to generalise it. The best aspects for women are the fact that this method is very simple, of easy use (Table 5), and avoids surgery and anaesthesia. Pain was frequently reported but did not decrease satisfaction (Table 6). Careful training of providers from the beginning of the study enhanced good results and helped to convince detractors of the efficacy of the method. Even though it made method use proceed more slowly, it was with more accuracy. We concluded this first step in 2003 with the need for another national meeting that included (1) a scientific presentation; (2) reports of the Tunisian studies and evaluation of the new experience of the ten clinics; and (3) elaboration of recommendations and guidelines in order to prepare a consensus involving all the protagonists, including the university College of Obstetrics and Gynaecology, which plays a key role in acceptability by the medical corporation and all policymakers. During the studies, there was high level of commitment of the heads of the ONFP and a strong involvement of the head of the largest maternity of the university hospital in Tunis. This commit-ment enabled rapid registration of mifepristone (with misoprostol) even when the medical community was resistant (suspicious and alarmist). The International Centre for Training and Research (CIF) now plays a very important role in training providers and different categories of the family planning clinic staff such as midwives, nurses, social workers, etc. All the introductory processes were related to training, with certain aspects dominated by a careful selection of potential providers to be trained and progressive step by step progression. Three steps were involved in the training of providers. 1. The first training involved only a few persons, mostly doctors in the family planning clinics and a few professors of obstetrics and gynaecology, who were already involved in family planning activities. It was greatly supported by the Population Council and the Centre for Training in Reproductive Health Technologies. 2. The second training was dedicated first to those selected for intensive training in France, but also to some selected midwives and nurses from the same clinics rather than the doctors who had already been trained. This was because we were strongly concerned about the need to obtain a good collaboration between doctors and paramedical staff in the clinics. 3. Both categories of trainees involved in the two groups (doctors and midwives in family planning clinics) became trainers after a refresher training, and they were able to organise local site trainings in their clinics. After these training procedures, we started recruitment with the supervision of staff from the centre of training (CIFR), who were responsible for managing all the introductory processes and evaluation steps. From the first steps of recruitment and throughout the period of initiation, staff of the training centre worked closely with each other and made regular in-site visits for supervision. The first evaluation was carried out in the reference centre after three months. This evaluation was carried out to discuss the progress of the study and to consider difficulties encountered while carrying out the study. It was also aimed at correcting the wrong attitudes of providers and counsellors. Conclusion Evidence of efficacy and safety of the method appears to have contributed strongly to the success of the study. It made providers enthusiastic for medical abortion, as they spontaneously advocated for it in their units. The reaction of participants was the same at each step of the trials and in each new clinic. We were however very careful first to train providers on all the steps involved in medical abortion before and during the first stages of the introduction, until we obtained an acceptable success rate. The progression of training and concern of people made them very flexible in their function, and depending on their level of knowledge and competence they could be involved in all the important stages of training and administration of the medical abortion process. Providing medical abortion, besides the registered conditions that need the practitioner's prescription, does not necessarily require an obstetrician/gynaecologist or even doctors. It could be easily managed by paramedical staff as long as they are well trained and sufficiently convinced and motivated. Women who experienced this method of medical abortion were highly satisfied, even higher than the success rate, thus making it a good alternative choice for women who need abortion. Acknowledgements We are grateful to the Population Council and Genuity Health Projects, which organisd and financed the three introductory studies. Special thanks to Mrs. Emanuelle H'sairi for her dedication to this method and valuable contribution to provider training in Tunisia, and to the providers and women who participated in this study. References
© Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04011t5.jpg] [rh04011f4.jpg] [rh04011t4.jpg] [rh04011t6.jpg] [rh04011t1.jpg] [rh04011f2.jpg] [rh04011f3.jpg] [rh04011t3.jpg] [rh04011t2.jpg] [rh04011f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}