 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
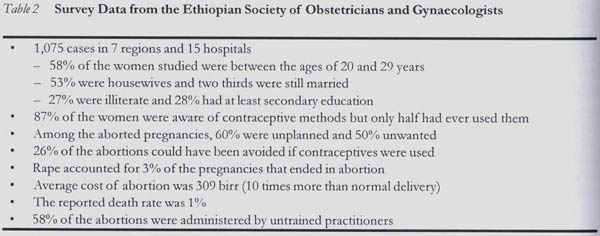
African Journal of Reproductive Health, Vol. 8, No. 1, April, 2004 pp. 79-84 Advocacy for Legal Reform for Safe Abortion Meaza Ashenafi Correspondence: Ms. Meaza Ashenafi, Executive Director, Ethiopian Women Lawyers Association (EWLA), P.O. Box 13760, Addis Ababa, Ethiopia. Tel: 251-1-523946; Fax: 251-1-531818; E-mail: ewla@telecom.net.et Code Number: rh04014 Abstract In Ethiopia, violation of women's reproductive rights is both a cause and a manifestation of women's disempowerment. Obstacles to full realisation of Ethiopian women's reproductive health and rights include the persistence of harmful traditional practices such as female genital mutilation, early marriage and abduction, as well as the disturbing prevalence of rape and HIV/AIDS. Unsafe abortion represents a particularly serious threat to women's health and lives. Ethiopia's status as a signatory to the Convention to Eliminate all Forms of Discrimination Against Women (CEDAW) and its constitutional guarantee of women's equality demand more aggressive action to eradicate such practices and inequities. After years of lobbying by women's organisations, parliamentarians are now reviewing a draft of the 1957 penal code, which includes numerous provisions addressing some of these practices and other conditions that underlie women's poor social and health status. (Afr J Reprod Health 2004; 8[1]:79-84) Key Words: Abortion, Ethiopia, CEDAW, legal reform, reproductive health Résumé Plaidoyer pour une réforme de la loi en faveur de l`avortement sans risqué. En Ethiopie, la violation des droits de reproduction de la femme est une cause et une manifestation du manque du pouvoir de s´assumer. Parmi les obstacles à la pleine réalisation des droits de la santé de reproduction de la femme éthiopienne sont la persistence des pratiques traditionnelles nuisibles telles la mutilation génitale féminine, le mariage précose et l`abduction ainsi que la prédominance inquiétante du viol et du VIH/SIDA. L`avortement à risque représente une menace à la sante´de la femme et à sa vie. Le statut de l`Ethiopie comme signataire à la Convention pour l`Elimination de toutes formes de Discrimination Contre la Femme (CEDCF) et sa garantie constitutionnelle de l`égalité féminine exige une action plus agressive pour éliminer de telles pratiques et injustices. Après des années de sollicitation par des organismes féminins, les parlementaires rédigent le brouillon du code pénal de 1957 qui contient de nombreuses dispositions pour aborder certaines de ces pratiques et d`autres conditions qui sous-tendent l` état social et de santé faible de la femme. (Rev Afr Santé Reprod 2004 ; 8[1]:79-84) Introduction Paragraph 7(2) of the Programme of Action from the 1994 International Conference on Population and Development (ICPD) defines reproductive health as a state of complete physical, mental and social well-being…in all matters relating to (a woman's) reproductive system and to its functions and processes…1 This broad definition demands that all practices, behaviours, structures and policies that directly or indirectly affect women's reproductive health facilitate exercise of the right to complete physical and mental health as distinguished from the mere absence of infirmity or disease. The well being of women and girls in Africa at large and particularly in Ethiopia is hampered by a number of policy, legislative, attitudinal and cultural factors. Ethiopia's endorsement of the above language as part of the ICPD Programme of Action implies a commitment to address these factors. This paper reviews the context of reproductive health and rights in Ethiopia with a focus on the impact of and need to address unsafe abortion. It highlights challenges and opportunities for liberalising Ethiopia's existing criminal law regulating abortion. My use of the term "advocacy for legal reform for safe abortion" means that women's right to abortion - despite my conviction that women's reproductive health should be approached squarely from a rights perspective - reflects recognition that more subtle language and strategies are useful in certain contexts. Especially in traditional countries like Ethiopia where no aspects of women's rights can be taken for granted, approaching the right to abortion from the public health perspective of preventing deaths and injuries from unsafe abortion, rather than from a rights-based perspective, may appeal to a broader constituency. Reproductive Health and Rights in Ethiopia Obstacles currently prohibiting full realisation of Ethiopian women's reproductive health and rights include a social context characterised by discrimination against women. As defined by the Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW), this means any distinction, exclusion or restriction made on the basis of sex, which has the effect or purpose of impairing or nullifyingthe recognition, enjoyment or exercise by women...on a basis of equality of men and women of human rights…2 Agreement to eliminate discrimination against women, so defined, requires removing all barriers to the full exercise of basic human rights through any and all measures necessary. Ethiopia is party to the CEDAW and has also incorporated the principle of women's equality as a constitutional principle. However, both de jure and de facto discrimination against women persists, and women's poor reproductive health status both reflects and perpetuates such discri-mination. Clearly, women's reproductive autonomy is central to the issue of women's equality and full participation in society. Ethiopia is a traditional society. Naturally, some of its customs have been invaluable for the cohesion and continued survival of the nation in the face of multiple economic and political challenges over several decades. But some harmful traditional practices have contributed immensely to the subordination and exploitation of women, directly impinging on their reproductive rights. After four years of intensive lobbying by women's organisations, parliamentarians are now making a draft revision of the 1957 penal code, which includes numerous provisions addressing some of these practices and other conditions that underlie women's poor social and health status. These organisations continue to play an important watchdog role in ensuring adoption of the draft law, which still faces resistance. One issue that is high on advocates' agenda is female genital mutilation (FGM), which is a common practice in Ethiopia; according to the latest baseline survey, close to 73% of women are mutilated.3 While it is beyond the scope of this paper to examine in depth the health complications that result from this practice, it is revealing to note that every year the fistula hospital in the capital city of Addis Ababa admits about 2,000 girl-children and women suffering serious reproductive system complications from FGM or early marriage. Some cause irreversible disability. Moreover, studies indicate that the annual number of patients as earlier indicated is only a tip of the iceberg, since many patients are not in a position to access health services and, therefore, remain unrecorded. Consistent with the Ethiopian constitution's prohibition of all harmful traditional practices causing physical or mental harm to women (Article 35/3), the draft penal law under consideration by the parliament criminalises FGM. After adoption and pending the challenge of implementation, Ethiopia will be one of 14 African countries that legally and officially condemn FGM. Early marriage, especially common in Ethiopia's northern highlands, is another harmful traditional practice that has a serious detrimental impact on women's reproductive rights and health. Research suggests that 35% of Ethiopian girls are married by the age of 15 years and 70% by 17 years. The mean age at first marriage among Addis Ababa women between the ages of 20 and 30 is 17 years.4 Reasons behind early marriage are complex and include cultural beliefs and socio-economic realities. The clearest effect of early marriage is to deny girl-children the key tool to their empowerment — education. Despite recent progress in improving the rate of girls' school enrolment, the gender gap - defined as the difference between boys' and girls' attendance in primary school - still remains at 20%. The school dropout level is also disproportionately higher for girls. Consistent with the constitutional guarantee noted above, the 1995 constitution proclaimed an equal age of marriage for boys and girls, and in 2000 the family law was amended to raise the marriage age for girls from 15 to 18 years (legal marriage age was previously 15 years for girls and 18 years for boys). Nevertheless, despite these and other initiatives to curb early marriage in Ethiopia, the practice remains a serious challenge to social and economic liberation of women. A third closely related harmful traditional practice in Ethiopia (which is not so common in other African countries) is that of forced marriage, also known as abduction. In this practice a young man, usually in consort with his friends, abducts the woman he desires to take as a wife. The practice has been defined as a criminal act since 1957, but the law provides immunity in cases where the abductor willingly marries the abducted girl (similarly a rapist who marries his victim is absolved of all criminal charges). The draft penal law suspends this provision since such immunity violates the constitution's basic definition of marriage as requiring the free and full consent of both members of a couple. Although it may not be identified as a harmful traditional practice, rape is another common form of violence against women in Ethiopia, which similarly violates their liberty and integrity. Child rape is an especially serious problem in Ethiopia. Although few data documenting the problem are available, numerous cases - many resulting in pregnancy and sexually transmitted diseases including HIV/AIDS - have been reported to legal aid centres such as the Ethiopian Women Lawyers Association (EWLA). Despite public outcry particularly against child abuse and rape, scant legal protection exists for women and girl-children. Rape outside wedlock is a criminal act under the 1957 penal code, but the law leaves the penalty to the discretion of judges, with a maximum penalty of 15 years imprisonment. The amendment currently under review establishes a minimum five-year jail sentence for rape offenders and increases the maximum penalty to 20 years in prison. A final dimension of the reproductive health context in which unsafe abortion must be examined in Ethiopia is the serious challenge posed by the HIV/AIDS pandemic. Of the 2.1 million people living with HIV/AIDS in Ethiopia, women aged 15-49 years constitute 1.1 million, or 52%.5 In addition to physiological factors (women's physiology makes them more susceptible to becoming infected), several socio-economic conditions, some of which are discussed above, account for the gender imbalance in HIV prevalence in Ethiopia. For instance, studies show that prostitution, whose driving force is poverty, increases young women's risk of exposure to the disease; and data from 1998 showed that 73.7% of female sex workers in Ethiopia were HIV positive.5 Less conspicuous factors include women's lack of social and economic capacity to negotiate safe sex. According to clients of the Ethiopian Women Lawyers Association, in marital relationships women are forced to submit to sexual advances even when they are sure of their partners' infidelity. Given these scenarios, women's minimal role in decision and policy-making at all levels, their lack of technical capacity, and the static/regressive roles played by predominant religions, Ethiopian women's health in general and their reproductive health in particular are severely constrained even in comparison to other countries in sub-Saharan Africa. Table 1, based on data from the 2000 demographic and health survey, summarises the reproductive risks that Ethiopian women confront. Unsafe Abortion: The Second Leading Cause One very serious threat to Ethiopian women's reproductive health that until recently has not been included in most statistics is that posed by unsafe abortion. In Ethiopia, abortion is legally permitted only in cases where the woman's life or health is in grave danger. These restrictions take their toll. According to Ministry of Health (MOH) reports, abortion complications are the fifth leading causes of hospital admissions and the second leading causes of deaths among hospitalised women. Ethiopia ranks very high on several risk factors related to sexual and reproductive health. It is estimated that one of seven women in Ethiopia dies from pregnancy-related complications. Skilled attendants are present at only 8% of births, and emergency obstetric complications including those related to unsafe abortion are a leading cause of maternal deaths. According to a recent report published by the Ethiopian Ministry of Health, abortion is the second leading cause of death of women, next to tuberculosis. Another study conducted in a hospital in Addis Ababa indicated that 54% of maternal deaths resulted from unsafe abortion. A thirdstudy conducted in five hospitals also estimated that 52% of maternal deaths were related to abortion. The largest study on unsafe abortion in Ethiopia was conducted by the Ethiopian Society of Gynaeco-logists and Obstetricians (ESOG) in 2002 (Table 2).6 Data were collected at 15 hospitals in seven out of nine federal regions, reporting on a total of 1,075 cases. Findings from the study challenge the prevalent assumption that abortion is restricted to a small section of the society, usually unmarried and irresponsible urban young women. To the contrary, researchers found that two thirds of women seeking treatment for abortion complications were married, and that nearly 60% were between the ages of 20 and 29 years. The study results also question the common belief that if legally permitted abortion would create a disproportionate burden on governmental health budgets. Moreover, the findings offer ample evidence of the negative impact of unmet family planning needs and justify liberalisation of abortion laws in countries where family planning is not a top priority. Although progressive for its time in some respects, Ethiopia's 1957 penal code was extremely conservative in its approach to women's reproductive autonomy. Not only did it prohibit abortion, it also penalised advertising and sale of contraceptives. In 1999, that provision was repealed because of its inconsistency with the constitutional guarantee of the "information and means" to regulate fertility. Revision of this aspect of the code was also required by the 1993 population policy, which aspires to increase family planning from 4% in 1993 to 44% in 2015; the current contraceptive prevalence rate among married women is only 8% for any method and 6% for modern methods.7 The Ethiopian penal code is very strict concerning abortion, allowing it only to save the pregnant woman from grave and permanent danger to life or health where it is impossible to avert in any other way. The law requires two doctors qualified to make a deter-mination on the alleged health defect to certify the need for abortion. Despite this prohibition, however, women determined to terminate unwanted pregnancies often risk their lives to do so by resorting to unsafe abortion. A number of organisations, including the Ethiopian Women Lawyers Association (EWLA), the Ethiopian Society of Obstetricians and Gynecologists (ESOG), Ipas and several grassroots associations have been working to call attention to women's right to safe abortion. To date, however, the draft revision of the penal code has failed to register progress on the issue. The only relevant proposal to date is to decriminalise abortion in case of rape and incest — conditions that can be used to mitigate the penalty for abortion under the 1957 penal code. This proposed change does not mean much in light of the anticipated procedural complications of proving rape, and given the small number of unsafe abortions it would affect (estimated at only about 3%). Nevertheless, women's groups are drawing lessons from the success of their advocacy related to the Ethiopian family law, which took four years of intensive collaborative work (1997-2000). Success obtained in achieving amendments to the penal code in other areas such as FGM, rape and abduction, as indicated above, is also a source of encouragement. While fully aware of the sensitivity of the abortion issue, women's groups have come a long way in challenging the defences against liberalisation of laws governing abortion in Ethiopia. Their objective remains, at a minimum, to win a law that permits abortion in cases of fetal deformity, HIV infection, or when a mental or physical disability makes it difficult or impossible to carry a pregnancy to term or to raise a child. As in other countries, the strongest opposition to liberalising the abortion law in Ethiopia comes from religious groups, which also oppose all forms of family planning and do not seem to offer women any options for ensuring their reproductive well being. We hope that in the future, religious institutions will play a more realistic and productive social role, given their immense power of outreach. In the meantime, advocates for women's health and rights rely on the existence of a constitution that proclaims a secular republican state to counteract the regressive influence of the religious opposition in matters related to reproductive health. Conclusion Women's reproductive health and rights are predicated on other aspects of women's rights such as education, civic participation, economic opportunity, etc. However, in Ethiopia, as in other countries, violation of women's reproductive rights is both a cause and a manifestation of women's disempowerment. As personal and private as it is, reproductive autonomy is also a key to women's ability to exercise all other fundamental rights. Preserving women from the dangers of unsafe abortion and ensuring women's ability to safely exercise their reproductive rights requires significantly greater attention from policymakers, the health system and society. In conclusion, I would like to reiterate an inspiring question posed by a speaker at the "Action to Address Maternal Mortality in Africa" regional consultation on unsafe abortion in Addis Ababa. The speaker, a senior medical doctor, challenged the forum by asking why we need a law on abortion in the first place. He argued that medical codes and guidelines should be sufficient to guide the provision of abortion procedures as they are for all other medical practices. Indeed, this approach would spare us all the acrimonious debates over whether to liberalise the law, how far to go in this regard, etc. The proposal is also supported by the interpretation of the CEDAW committee, which asserts that limitations placed on services or practices needed only by women constitute discrimination. Moreover, the African protocol on women, adopted by the Conference of Heads of State and Government of the African Union in Maputo in July 2003, sets the tone for the legal framework of abortion laws in Africa. The protocol, beyond affirming women's reproductive autonomy, permits abortion in cases of sexual assault, rape, incest, and where the continued pregnancy endangers the mental and physical health of the mother or the life of the mother or the unborn child.8
References
© Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04014t1.jpg] [rh04014t2.jpg] |
| |||||||||

{kind=link}
{kind=link}