 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 8, No. 1, April, 2004 pp. 85-91 Promoting Sexual and Reproductive Health and Rights in Nigeria through Change in Medical School Curriculum Boniface A Oye-Adeniran1,2, Isaac F Adewole2,3, Ngozi Iwere3 and Pat Mahmoud3 1Department of Obstetrics & Gynaecology,
College of Medicine, University of Lagos, Lagos, Nigeria. 2Department
of Obstetrics & Gynaecology, College of Medicine, University of Ibadan,
Ibadan, Nigeria. 3Campaign Against Unwanted Pregnancy, Lagos,
Nigeria.
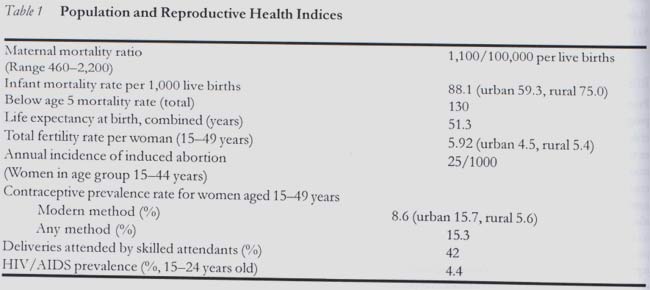
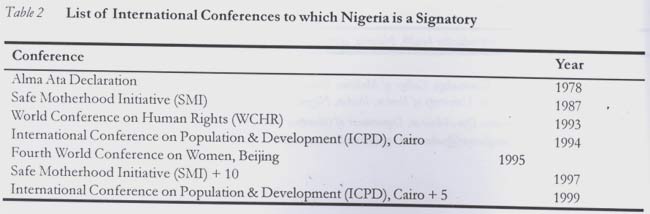
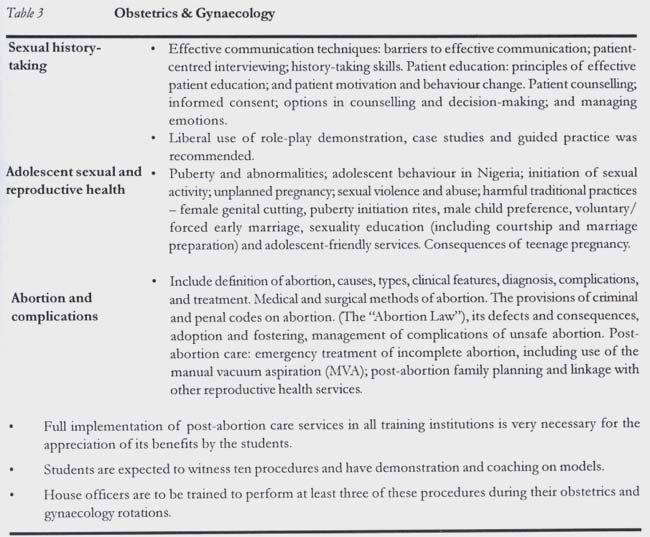
Code Number: rh04015 Abstract Significant developments have occurred in the field of sexual and reproductive health and rights (SRHR) globally in the last decade. However, this is yet to translate into improved status of SRHR in developing countries. One of the strategies recognised worldwide for addressing the poor status of SRHR is human capacity building at all levels. A pilot work conducted in two federal university medical schools identified a major gap in knowledge among medical students on issues related to SRHR. This called for a review of the curriculum to enable the incorporation of relevant and topical issues. This article describes the processes leading to the adoption of the Nigerian medical schools' sexual and reproductive health and rights curriculum. The exercise culminated in the identification of internal and external stakeholders and needs of the Nigerian medical schools in teaching reproductive health. The participation of lecturers (bottom-up approach) brought about a sense of ownership of the document and promoted the broad consultation and participation of all participants. It also identified capacity building and the need for evaluation as a basis for further review. (Afr J Reprod Health 2004; 8[1]:85-91) Key Words: Sexual and reproductive health, Nigeria, curriculum, Campaign Against Unwanted Pregnancy. Résumé Promotion des droits de la santé et sexuelle de reproduction au Nigéria à travers la modification du programme scolaire medical. Il y a eu des développements importants dans le domaine de la santé et les droits sexuels et de reproduction (SDSR) dans le monde entier au cours de la dernière décennie. Pourtant ceci n`a pas encore été tradiut en une meilleure condition de la SDSR dans les pays en voie de développement. Une des stratégies reconnues dans le monde entier pour aborder le statut faible de la SDSR est le renforcement de capacité humaine à tous les niveaux. Une etude pilote menée au sein de deux écoles médicales des universités fédérales a identifié un écart important dans la connaissance chez les étudiants en médicine sur des questions liées à la SDSR. Ceci nous a obligé de revoir le programme afin d`inclure des sujets pertinents et d`actualité. Cet article décrit le processus menant à l`adoption du programme de l` école médicale nigériane sur la santé sexuelle et les droits de reproduction. Le projet a abouti à l`identification des partenaires sociaux internes et externes et les besoins des écoles médicales nigérianes dans l`enseignement de la santé de reproduction. La participation des enseignants (l`approche de bas en haut) a provoqué un sens de la propriété du document et elle a encouragé de grandes consultation et participation de tous les participants. Elle a également identifié le renforcement de capacité et la nécessité d`une évaluation comme base pour d'autres examens. (Rev Afr Santé Reprod 2004; 8[1]:85-91) Introduction Nigeria is the most populous country in Africa with a population estimate of about 134 million in 2003.1 It has the largest concentration of black persons globally. One out of every five black persons is a Nigerian. Data from the Population Reference Bureau1,2 indicate that Nigeria has some of the worst reproductive health indices in the world (Table 1). Nigeria consequently has enormous unmet reproductive health needs.3-5 It is believed that local implementation of internationally acclaimed strategies would improve various reproductive health indicators.3 Presently, the country has enunciated bold plans for the rectification of some of these problems in the national health and population policy,6 which was launched in 2001. A review of the curriculum is one of the strategies being promoted to solve some of these problems.7,8 International Challenges The reality of un-attainability of "health for all by the year 2000", as was earlier envisaged, prompted a revision of strategies that had been in existence for addressing various health issues. Prominent among these review processes were the series of international conferences that were held during the last decades of the twentieth century. These conferences are listed in Table 2. These meetings noted, among other things, that although the bulk of health-related problems in the world, especially in the developing countries, were often attributed to poverty, illiteracy and lack of resources, there were other contributory factors that had hitherto been overlooked. These factors include gender inequalities, "neglect" of adolescents and poor efforts at ensuring fertility regulation.9 The conferences crystallised women's sexual and reproductive health and rights as important issues requiring global attention and action. Other issues brought to public domain include adolescent health, fertility regulation, ethics, gender and power, abortion and post-abortion care, quality of care, sexually transmitted infections and HIV/AIDS, resource allocation, and project management. These international efforts also called for the improvement of quality of care by ensuring that medical school curricula and health care training include gender-sensitive, client-centred comprehensive and mandatory courses in women's sexual and reproductive health and rights. In this regard, there was acceptance of the call for the recognition of sexual and reproductive rights as human rights, thereby affirming them as an inalienable, integral and indivisible part of universal human rights. It was also agreed that all health services and providers should conform to human rights, ethical, professional and gender-sensitive standards in the delivery of health services including family planning and related reproductive health services.10 The implications of this resolve include such affirmations as reproductive health care should be accessible to every individual by right; health care providers must upgrade their ethical standards to guarantee these rights, as well as ensure that their services are gender-sensitive. These international efforts also called for the development of integrated service, information and educational programmes for adolescents that address adolescent sexual and reproductive health issues including unwanted pregnancy, unsafe abortion, sexually transmitted infections and HIV/AIDS.10 This necessitates restructuring of existing health systems and development of collaborations to provide adolescents and other relevant individuals with information, education, counselling and services that could prevent or control sexuality issues, unsafe abortion, sexually transmitted infections and HIV/AIDS, among others. Rationale for the Curriculum The experience gained by the Campaign Against Unwanted Pregnancy (CAUP) through working with young persons indicated a radical need to review the existing medical curriculum in our universities. There exist 16 accredited medical schools in Nigeria, each of which currently graduates an average of 100 doctors annually. Endowment of these new and future doctors with improved capability to provide reproductive health care will give a tremendous boost to the country's effort to revamp the reproductive health of its citizens.8,11,12 Teachers in the medical schools have complained about gross defects in the curricula of these schools and their review will, therefore, be needed as a first step towards enhancing their relevance and impact, as was done in the United States of America and advocated by the Commonwealth Medical Association Trust.7 A pilot work conducted in two federal university medical schools identified a major gap in knowledge among medical students on issues related to reproductive health. The curriculum in use lacked depth and focused more on theoretical and hard core obstetrics and gynaecology to the detriment of practical and relevant issues affecting reproductive health. The traditional components of core obstetrics and gynaecology, though relevant for individual case management, lacked public health value. There is therefore a need to develop a revised curriculum to meet the new challenges in the field of sexual and reproductive health and rights. These issues include: • Enhanced and more in-depth focus on family planning information and services, which would also emphasise quality of life and reproductive health goals rather than demographic goals. • Expanding the frontiers of teaching of abortion to the full extent of the law as a medical subject to an all-embracing issue with social, cultural, economic, religious, ethical, political and health dimensions. • Training in safe abortion care services and post-abortion contraception when these are not against the law. • Socio-cultural and political dimensions of sexual and reproductive health. A gender perspective of reproductive health, which must emphasise male involvement in the prevention of unplanned pregnancy and contraceptive acceptance and usage. • Expanding the notion of rights in sexual and reproductive health. • Emphasising the burden of reproductive tract infection (RTI) in developing countries and linkage with infertility and cancer among women. • Teaching HIV/AIDS as an important subject with introductory sessions on counselling in health care. • Expanding the preventable nature of reproductive tract cancer. • Emphasising the acquisition of clinical skills as an integral component of the training curriculum. • Emphasising the linkage between resource mobilisation, appropriate utilisation of resources for effective intervention and quality of health care. Methodology A multi-phase systematic approach was adopted to facilitate maximum attainment of set objectives. Pre-Review CAUP identified and recruited two consultants who were seasoned teachers in the medical schools in May 2000 to prepare a draft revised medical curriculum for use at the planning meeting. The consultants visited all the accredited medical schools in the country for needs assessment, to study their curricula and hold consultations with the teachers. They sensitised them on the need for a revised curriculum and discussed areas that required amendments with them. The consultants submitted two reports, which were considered at the planning meeting held at the Gateway Hotel, Ota, near Lagos, on 23-27 August 2000. Participants at the planning meeting included representatives of international agencies such as the WHO, CEDPA, Pathfinder and UNFPA, heads of departments of obstetrics and gynaecology, the Nigerian Medical Association, medical students, consultants and CAUP coordinators and staff. The interim report prepared at the planning meeting was circulated far and wide across the medical and reproductive health circle in Nigeria for comments. The reports indicate that many medical schools did not have well thought-out curricula, while those that had curricula did not have mechanisms for periodic review. Review Meeting A meeting was convened to review the curriculum of Nigerian medical schools from February 22 to 25, 2001, at the Gateway Hotel, Ota, near Lagos. The forum brought together university lecturers, admini-strators, related associations/bodies, policymakers and medical students to produce a set of guidelines for the content of sexual and reproductive health and rights in the medical school curriculum. In all, there were 78 participants drawn from 16 accredited Nigerian medical schools, health profes-sional associations, medical students, policymakers including the Federal Ministry of Health, Federal Ministry of Education, the National Universities Commission, Nigerian Educational Research and Development Council, and the Federal Ministry of Women's Affairs and Youth Development), as well as international organisations. Subjects covered by the review included medical sociology, physiology, pathology, microbiology, haematology/immunology, pharmacology, paediatrics, obstetrics and gynaecology, general community health, psychiatry, surgery/urology and medical ethics. During the three-day meeting, presentations were made by academicians, representatives of medical schools and educational organisations, followed by group discussions. The deliberation culminated in the adoption of a proposed set of guidelines for the Nigerian medical school curriculum on sexual and reproductive health and rights.13 A key feature of the adopted guidelines is an expanded curriculum in obstetrics and gynaecology (Table 3). The guidelines are intended to be incorporated into existing curricula in an effort to update the sexual and reproductive health and rights content and ensure that medical school graduates are adequately equipped to perform their roles in addressing respective reproductive health issues when they commence practice in the community. The adopted curriculum incorporated a wide spectrum of new concepts such as:
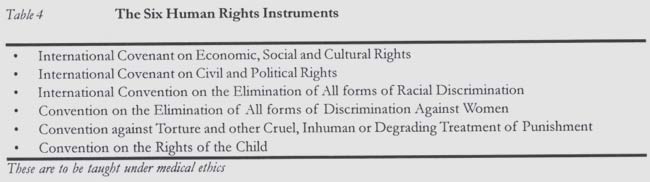
• Adolescent sexual and reproductive health • Abortion and its complications • HIV/AIDS • The six human rights instruments related to "the right to health" to be taught under medical ethics (Table 4). Post-Review CAUP has carefully monitored the implementation of the adopted curriculum on sexual and reproductive health and rights meant for use in accredited medical schools in the country since it was circulated. The Federal Ministry of Health, on its own volition, has adopted all the contents of the reviewed curriculum and has re-circulated it to the medical schools for further comments. CAUP is getting feedback from the medical schools on the use of the adopted curriculum. The ten accredited medical schools visited so far by CAUP coordinators have reviewed the contents of their reproductive health curricula. The remaining accredited schools will be visited in 2004. CAUP planned to organise workshops to build the capacity of lecturers/professors in the medical schools to teach sexual and reproductive health and rights. Teaching aids such as overhead and multimedia projectors, computers including laptops, and photocopiers have been provided to the ten medical schools visited to support their teaching of SRHR. The other six medical schools will be given teaching aids this year. An exchange programme for students and teachers is also envisaged to enable continuous exchange of knowledge and information. CAUP, in collaboration with other interested partners, plans to further develop the contents of the adopted curriculum into training manuals. Conclusion This paper outlines the processes undertaken by the Campaign Against Unwanted Pregnancy, in collaboration with all the 16 accredited medical schools, in reviewing the Nigerian medical schools' curriculum on SRHR. The exercise involved five key areas and identified some challenges. These areas are:
1. Identification of internal and external stake-holders and needs of the Nigerian medical schools 2. The bottom-up approach, bringing about a sense of ownership by all participants 3. Broad consultation and participation 4. Capacity building, as part of a continuing medical education of students and lecturers 5. Evaluation as a basis for further review - as curriculum review is a continuous process The challenges were lack of resources, inadequate knowledge about SRHR, lack of political will, opposition from religious leaders, and less liberal interpretation of reproductive health legislation by health care providers. These challenges can be overcome through advocacy, education of policy-makers, religious and community leaders, and partnership with other reproductive health-focused non-governmental organisations. The authors believe that the poor state of SRHR in Nigeria can be addressed by facilitating capacity building through faithful implementation of the adopted curriculum. Acknowledgement We wish to acknowledge the invaluable contributions of our consultants, the 16 accredited medical schools, the National Universities Commission, the Department of Hospital Services of the Federal Ministry of Health and non-governmental organisations in the planning and conduct of this review and adoption of the curriculum on SRHR for Nigerian medical schools. The John D. and Catherine T. MacArthur Foundation's grant No. 99-58346-GSS supported the review, while grant No. 02-71972-000-GSS supported the provision of teaching aids to the accredited medical schools. The views expressed in this article do not necessarily represent the opinion of the John D. and Catherine T. MacArthur Foundation. References
© Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04015t2.jpg] [rh04015t1.jpg] [rh04015t4.jpg] [rh04015t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}