 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 8, No. 2, Aug, 2004 pp. 59-63 Donor Blood Procurement and Utilisation at the University of Benin Teaching Hospital, Benin City ME Enosolease1, CO Imarengiaye2 and OA Awodu1 Departments of Haematology1 and 2Anaesthesiology,
University of Benin Teaching Hospital, P. M. B. 1111, Benin City, Nigeria.
Code Number: rh04026 Abstract Banked blood is a limited resource in Nigeria. We sought to
evaluate factors that may further limit the effective utilisation of donor
blood in a tertiary hospital in Benin City. The records of the blood transfusion
unit of the hospital were studied to identify the methods of blood procurement
and utilisation from January 1, 2000 to December 31, 2002. A total of 11,021
units of blood were received in the blood transfusion unit within this period
out of which 1491 (13.5%) donor blood samples were found unfit for transfusion
and, hence, discarded. Commercial blood donation accounted for 95.3%, compared
to 4.7% from replacement and volunteer donors. Commercial blood donation was
a major risk factor for likely disposal of donor blood (x2 =
74.3, p < 0.0001, OR = 21.1, 95% CI = 7.8-56.7). Expired units of blood
with low PCV were discarded for lack of infrastructure to fractionate and store
them.
Over Key Words: Donor blood, precurement, transfusion-related viral infection Résumé L'obtention du sang de donneur et l'utilisation au Centre
Hospitalier Universitaire de Benin City. Le sang gardé dans la
banque de sang est une ressource limitée au Nigéria. Nous avons
essayé d'évaluer les facteurs qui peuvent limiter davantage
l'utilisation efficace du sang de donneur dans un hôpital tertiaire à Benin
City. Les dossiers du service de la transfusion sanguine de l'hôpital
ont été étudiés pour identifier les méthodes
d'obtention et d'utilisation du sang à partir du 1er janvier
2000 jusqu'au 31 décembre 2002. Au total, 11,021 unités de
sang ont été obtenu dans le service de transfusion sanguine
au cours de la période. Dans l'ensemble, 1491 (13,5%) échantillons
du sang de donneurs ont été jugés impropres à la
transfusion et donc ont été rejectés. Le don commercial
de sang représente 95,3% volontaires. Le don commercial du sang était
un risque majeur pour la disposition du sang de donneur (x2=74,3,
p<0.0001, OR = 21,1, 95% CI = 7,8-56,7). Des unités de sang à faible
VCP ont été rejetés faute d'infrastructure pour les
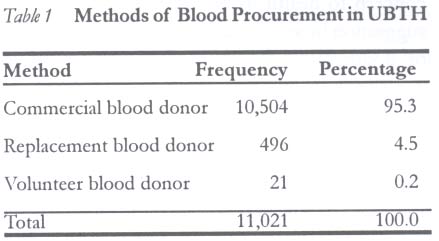
fractionner et les conserver. Plus de Introduction Blood and blood products are resources in the hands of clinicians. The demand for blood transfusion services in Nigeria is high due to road traffic accidents, surgical and obstetrical blood loss, and anaemia from other causes. In spite of its usefulness, donor blood is still a limited resource in developing countries.1,2 There are several reasons for this limited availability of donor blood.2 The main sources of blood procurement are voluntary donor programme or commercial blood donors. The hospital's policy on blood screening is that all donations are checked anonymously for viral pathogens. Those in the voluntary donor's programme may be screened prior to phlebotomy. A commercial blood donor offers a unit of blood for a fee paid by the contracted hospital vendor. A replacement blood donor is a family member or relation of a patient, donating a unit of blood to be used for a specific patient. Volunteer blood donors are well-meaning members of the society who offer themselves for free, non-remunerated, non-directed blood donations. Improving the availability and efficient utilisation of donor blood may include limitation of wastages of donor blood. Anecdotal reports indicate that some units of donor blood are discarded after procurement possibly because they were not tested for viral pathogens before phlebotomy by the designated blood vendor. The units of blood supplied commercially by blood vendors are usually collected from outside the hospital's blood bank. This development is inimical to the efficient utilisation of this scarce product. It would be helpful to identify factors leading to disposal of donor blood as a way of encouraging rational utilisation of blood and blood products. The objective of this investigation is to evaluate the procurement and utilisation of donor blood at the University if Benin Teaching Hospital, Benin City, Nigeria. Methods Records of the blood transfusion unit of the University of Benin Teaching Hospital were reviewed from January 1, 2000 to December 31, 2002, in order to identify the methods of donor blood procurement and utilisation. For every unit of blood, we studied the method of procurement (commercial or volunteer blood donation) and utilisation (transfusion or disposal). Blood from commercial donors is usually obtained from outside of the hospital through a vendor. Collection by the vendor is usually not supervised by hospital personnel but adheres to routine guidelines for phlebotomy. The vendor brings the units of blood to the hospital in fulfillment of a contractual agreement. Blood from volunteers (replacement donor or panel donor) is collected at the blood transfusion unit of the hospital. Blood (450ml) is usually collected into a bag containing 65ml citrate phosphate dextrose with adenine (CPDA) and stored at 2-8oC. Prior to phlebotomy, the donor's blood group is determined and the packed cell volume (PCV) ascertained. Units of blood from commercial donors are inspected to determine good anticoagulation and exclude haemolysis. Thereafter, they are screened for HIV and HbsAg. HIV screening is conducted using the Hexagon® HIV strips. The strip has three horizontal lines labelled control, HIV-1 and HIV-2. At room temperature, and using automatic micropipette, 20µl of whole blood is added to the indicated window on the test strip with three drops of a diluent (tris buffer mmol/L and sodium azide 0.02%w/v). The test strip is read within 10 minutes while still holding the strip horizontally. A single red line at position C (control) on the strip indicates a valid control. A similar line is found in either position 1 or 2 if positive for either HIV-1 or HIV-2. The sample is negative for HIV if there is no colour change in positions 1 and 2. Hepatitis B surface antigen screening is carried out using ACON's one-step hepatitis B antigen test strip. An already anticoagulated blood sample is collected into a clean tube and centrifuged at 3000rpm for 10 minutes to obtain clear plasma at room temperature. A test strip is then inserted into the test plasma to a maximum indicated by the manufacturers for 15 seconds and laid face up on a flat non-absorbent surface. A test is positive if two transverse bands (T = test and C = control) are seen and negative when only the one band at control (C) is seen. Only units of donor blood found to have adequate PCV (> 36%), good collection and storage, and free from these viral infections are offered for transfusion to patients. Others that fail any of the above screening tests are discarded. The units of blood discarded are further scrutinised to determine the reasons for disposal and the unit cost of procurement calculated. The results are presented as counts and frequencies where necessary. Statistical analysis was conducted using the GraphPad Instat® (1990-1994). Chi square test was used to test the association between commercial and replacement donor as risk factor for wastage of donor blood. A p value of less than 0.05 was considered significant. Results A total of 11,021 units of donor blood were procured within
the study period. Blood procurement was mainly from commercial blood donors
(95.3%) while replacement and volunteer donors accounted for 4.7%, as shown
in Table 1. Table
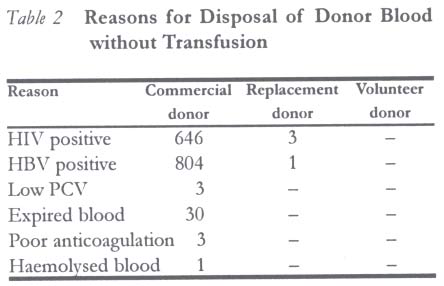
2 shows that 13.5% (n = 1491) of the total units of blood
procured were discarded. A high proportion of disposed donor blood was from
commercial donors. Contamination with human immunodeficiency virus (HIV) and
hepatitis B virus were the leading reasons for discarding donor blood. The
prevalence of viral infection among blood donors was 5.9% (649/11021) for HIV
and 7.3% (805/11021) for HBV. No unit of blood tested positive for both viruses.
Thirty
units of blood were discarded
following expiration. Serotypes AB and A rhesus
negative were the blood groups commonly discarded
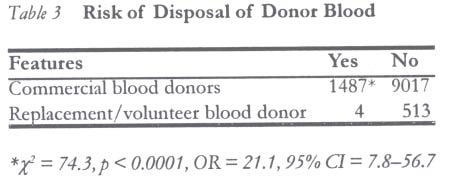
(data not shown). The risk of disposal of donor
blood (Table 3) was higher among
commercial blood donors than volunteer and replacement donors combined (x2 =
74.3, p < 0.0001, OR = 21.1, 95% CI = 7.8-56.7).
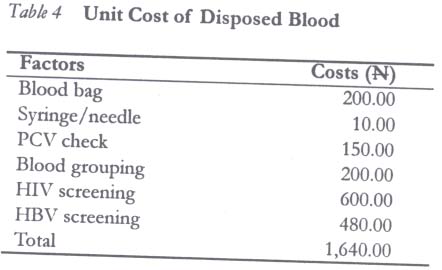
The computed costs of the disposed units of blood are shown in Table
3. A unit
of donor blood is procured at a cost of Discussion Procurement of donor blood is mainly through commercial donors as seen in this study. Viral contamination was the leading cause for disposal of donor blood meant for transfusion. The safety of donor blood for transfusion has been a major concern to health workers. This has led to the suggestion by several authors for rigorous testing of donor blood for viral infections3-5 and even parasites.6 In spite of these tests, the risk of residual viral infections may exist. In one study, Moore et al7 estimated that 2% of transfusion blood in Kenya was contaminated with HIV. In another study,8 the residual post-transfusion risk of HIV and HCV infection of blood collected from replacement donors ranged from 1:260 to 1:16,393 after screening for anti-HIV, p24 antigen and anti-HCV. These results7,8 have a number of implications. First, the prevalence of viral infections (HIV = 5.9%, HBV = 7.3%) among the blood donors in our study is similar to findings in these studies. This may imply a similar risk of transfusion transmissible viral infections. Second, the method of blood procurement in the hospital may require an overhaul, as it is dependent on commercial donors. The prevalence of HIV and HBV in this population of blood donors may indicate the risk of transfusion transmissible viral infection. The current methods of blood screening may not identify all infected blood. For example, the Hexagon® rapid kit used in our blood bank has a high sensitivity but does not preclude the risk of transfusion transmitted HIV infection. This lapse could be explained by the period of seroconversion, during which there is no antibody to the virus. This may mean the transfusion of some units of blood that are negative to testing but actually have the human immunodeficiency virus. The use of surrogate markers for HIV infection among blood donors has been suggested.9 The authors showed anti-HBc and anti-HCV as useful surrogate markers for HIV infection in blood donors. In addition, they speculated that screening for these surrogate markers may prevent the small number of cases in which HIV is still transmitted by transfusion. Nevertheless, screening for HCV in donor blood is not routine in our hospital. Thus, other methods of improving utilisation and safety of donor blood may be necessary. Improving the utilisation of donor blood, a scarce resource, in developing countries will include screening for risk factors for viral infection in potential donors. Sentjens et al10 showed risky sexual behaviour to be significantly associated with HIV infections in Ethiopia. The results of the study indicate that 25% of STD clinic attendees tested positive for HIV. Identifications of similar risk factors in would-be blood donors in our centre may minimise wastage of donor blood and improve its safety. Simple measures such as sub-group selection of donor, stricter indication for blood transfusion and correct use of non-expired tests have been speculated to decrease the risk of iatrogenic HIV transmission.11 Extending these simple measures to our centre may be difficult for some reasons. Commercial blood donors, the major source of donor blood in our environment, may refuse pre-donation screening. Sub-group selection of donors is unlikely until structures and policy to encourage voluntary non-remunerated blood donation are put in place. Comparison of methods of procurement in different countries may not be valid due to the differences in policy on donor blood. In our centre, donor blood is mainly from commercial donors. This is unlike other countries where blood transfusion service is centralised. The patient finances procurement and screening of each unit of donor blood in our hospital. Public funding of transfusion services in sub-Saharan Africa has been suggested.12 Public participation and funding of safe transfusion may eliminate the difficulties with donor blood procurement. Such level of community involvement is also likely to enable a safer method of procurement and decrease the huge wastage associated with current methods. Specifically, the availability of appropriate technology could have obviated the units of blood discarded on account of low PCV. Other blood components like fresh frozen plasma, cryoprecipitates and coagulation factors can be derived from units of blood with low red blood cells. Similarly, the expired units of donor blood in this study are the rare phenotypes (like O rhesus D negative and ABO groups), often reserved for specific indications. Their disposal could have been avoided if infrastructure for fractionation and storage of the blood products were available. Thus, improved funding of blood banking facilities may prevent the disposal of non-infected donor blood. We reviewed factors that affect procurement and utilisation of donor blood. Commercial blood donation was the main source of banked blood for transfusion. HIV and HBV were the main viral infections resulting in disposal of blood products. The public health implications of current methods of sourcing donor blood are enormous. An overhaul of methods of blood procurement to include sub-group selection of donors, improved funding of blood banking services may minimise wastages of donor blood and enhance effective utilisation of this scarce resource. References
© Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04026t4.jpg] [rh04026t1.jpg] [rh04026t3.jpg] [rh04026t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}