 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 8, No. 2, Aug, 2004 pp. 64-70 Are Public Antenatal Clinics in Blantyre, Malawi, Ready to Offer Services for the Prevention of Vertical Transmission of HIV? Humphreys E Misiri1, Eyob Tadesse2 and Adamson S Muula1 1Department of Community Health, University
of Malawi College of Medicine and 2Department of Obstetrics and
Gynaecology, College of Medicine and Queen Elizabeth Central Hospital, Blantyre,
Malawi.
Code Number: rh04027 Abstract At least 10% of the adult population in Malawi is infected with HIV and vertical transmission is a major mode of transmission. Currently, there are plans to provide widespread antiretroviral therapy to prevent mother to child transmission of HIV. This study was conducted to describe the perceptions of midwives towards selected issues regarding prevention of mother to child transmission of HIV in eleven public health centres in Blantyre, Malawi. A cross-sectional study using a self-administered questionnaire incorporating both open-ended and closed-ended questions was used. Twenty seven midwives participated in the study. Less than half (40.7%), of them reported working at a baby friendly hospital initiative health facility, while 96.3% reported that they would advise an HIV infected woman to breastfeed her infant. HIV prevention messages were reportedly offered routinely by 77.8% of the respondents, but only 22.2% reported that their clinics offered condoms to pregnant women. Also, only 37.0% reported offering routine STI screening, while 37.0% of the midwives would support antenatal women being accompanied by their male partners. Majority (81.2%) said that women who know they are HIV infected should not become pregnant, while 37.0% reported that they would be uncomfortable to assist in the delivery of an HIV infected woman. There was lack of appropriate clinic space and sterile gloves for the proper delivery of maternity services. Midwives in Malawi need training, supervision and other support to provide adequate health care services to antenatal women. (Afr J Reprod Health 2004; 8[2]: 64-70 ) Key Words: Malawi, vertical transmission, mother-to-child transmission, HIV Résumé Les cliniques prénatales publiques à Blantyre, Malawi, sont-elles prêtes à assurer des services pour la prévention de la transmission verticale du VIH? Dix pourcent de la population adulte au Malawi sont infectés par le VIH. La transmission verticale est un moyen important de transmission. A l'heure actuelle, il y a des tentatives pour assurer la thérapie anti-retrovirale bien répandue pour prévenir la transmission du VIH de la mère à l'enfant. Cette étude a été menée pour décrire les perceptions des sages-femmes envers des problèmes sélectionnés concernant la prévention de la transmission du VIH de la mère à l'enfant dans onze centres de santé publique à Blantyre, Malawi. Nous avons effectué une étude transversale à l'aide d'un questionnaire auto-administré qui incorporait à la fois les questions sans limite et celles qui sont limitées. Vingt-sept sages-femmes ont participé à l'étude. Moins d'une moitié (40,7%) ont déclaré qu'elles travaillaient dans les hôpitaux adoptés aux besoins des enfants alors que 96,3% ont déclaré qu'elles conseilleront à une femme infectée par le VIH d'allaiter son enfant. Des messages pour la prévention du VIH, selon 77,8% des interviewées, ont été diffusés régulièrement, mais, seuls 22,2% ont déclaré que leurs cliniques donnaient des préservatifs aux femmes enceintes. De plus, il n'y avait seules que 37,0% ont déclaré qu'elles assuraient le dépistage de routine des MSTs, alors que 37,0% des sages-femmes soutiendraient que les femmes prénatales soient accompagnées par leurs partenaires hommes. La majorité (81,2%) ont dit que les femmes qui savent qu'elles sont infectées par le VIH ne doivent pas devenir enceintes, alors que 37,0% ont déclaré qu'elles ne seriont pas à l'aise à assister à l'accouchement d'une femme infectée par le VIH. Il manquait d'espace approprié dans la clinique ainsi que de gants stériles pour la présentation des services de maternité. Les sages-femmes malawiennes ont besoin de formation de surveillance et tout autre appui afin qu'elles puissent rendre des services de soins de santé adéquate aux femmes prénatales. (Rev Afr Santé Reprod 2004; 8[2]: 64-70 ) Introduction Africa, and especially southern Africa, has been significantly affected by HIV/AIDS. Malawi's HIV infection rate is estimated to be at least 10% among the adult population.1 High infection rates have been reported in Blantyre, the major commercial city of Malawi, among women attending antenatal care, where up to 30% are reported to be infected.2 There has been increasing global interest towards the prevention of vertical or mother to child transmission of HIV (MTCT). Initially, at least in the developed world, caesarian section deliveries were instituted to prevent vertical HIV transmission.3 Such an intervention was deemed inappropriate for the majority of women in Africa. Various antiretroviral therapy regimes have been tried and have brought new hope in the prevention of vertical HIV transmission even in Africa. This has been possible because of simplified drug regimens and reduction in prices of antiretrovirals (ARVs). HIV is mainly spread heterosexually in Africa.4 The other major mode of transmission is vertical transmission, when a baby or child acquires HIV from the mother in-utero, intrapartum and through breastfeeding. The following maternal and infant factors facilitate vertical HIV transmission: advanced maternal disease, reduced CD4 counts, mastitis, high viral load, genital tract infection and oral sores in the infant.5,6 Prevalence of genital infections among antenatal women has been described as high in several locations in Africa, with over 60% infection rates in some settings.7,8 Mastitis is potentially preventable through improvement of the micronutrient status of nursing women.9 HIV transmission is also efficient with colostrum and early milk, as they have higher viral load than mature milk.10 Studies to determine whether vitamin A supplementation could reduce vertical transmission have shown no positive effect.11 Prenatal HIV testing was reported to be acceptable to the majority of women studied,12 where 92.5% suggested that it is a good idea in Ireland. In Rwanda, HIV testing was acceptable to the majority of women with high maternal age and high socio-economic status of spouse.13 A multi-centre study14 reported HIV acceptance rates averaging 69% among pregnant women. It is therefore expected that with such high level of HIV testing acceptance, prevention of mother to child transmission (PMTCT) programmes would be implemented in many sites in Africa. While acceptability of HIV testing reported is high, some women decide not to inform their spouses when tested in the absence of the male spouse. In Malawi, midwives receive training in HIV during both pre-service and in-service trainings. Most of the trainings concentrate on counselling and education on the prevention of HIV infection and not on ARV therapy. In early 2004, Malawi provided ART for the prevention of vertical HIV transmission in a few mission hospitals, two central hospitals and three private hospitals using nevirapine as pilot initiatives. Expansion of the programmes has been planned using resources from the Global Fund for the prevention of tuberculosis, malaria and HIV/AIDS.15 Midwives are at the forefront in the provision of care to pregnant women and nursing mothers. However, the perceptions and experience of this cadre of healthcare workers has not been studied. We therefore undertook this study to describe the perceptions and experiences of nurse-midwives towards efforts to prevent mother to child transmission of HIV in Blantyre, Malawi. Materials and Methods This cross-sectional descriptive study carried out in 2003 utilised a self-administered questionnaire. The survey instrument contained questions on demographic characteristics of respondents, perceptions and advice towards breastfeeding support, availability of infrastructure for HIV testing, knowledge about use of ARVs to reduce PMTCT of HIV and perceptions towards HIV infected women and babies. Both open-ended and closed-ended questions were used. All midwives currently in public practice within the Blantyre District health office were eligible for recruitment. Eleven public health centres, five rural and six urban in Blantyre participated, two of which offered HIV testing on site while the rest offered counselling and advised clients to obtain testing elsewhere. Syndromic STI management is practiced in all the clinics. Respondents were interviewed during antenatal clinic (ANC) visits. Midwives who were on leave or had travelled were excluded from the study. Data was analysed using Microsoft Excel 6.0 to obtain proportions. Explanations obtained from open-ended questions were analysed based on themes and, in some cases, particularly interesting answers presented as written by the respondent. Results Twenty seven midwives participated in the study. The number of years they had practiced mid-wifery ranged from 2 to 32 years (mean 15.5 years). Attitudes Towards Breastfeeding Of the 27 respondents, 21 (77.78%) reported training women on how to properly position baby during breastfeeding, while 3 (11.11%) did not and 2 (7.40%) were not sure. Eleven (40.74%) of them worked at baby-friendly health facilities, 9 (33.33%) did not work there, while 6 (22.22%) did not know about the baby-friendly hospital initiative.16-18 The advice given by midwives to ANC attendees on exclusive
breastfeeding was determined. Almost all (96.30%) the midwives reported encouraging
all women to practice exclusive breastfeeding, while only one reported otherwise.
Interestingly also 96.30% reported that they would advise HIV-infected women
to exclusively breastfeed, while only one respondent reported that she would
not do so. Regarding whether to provide exclusive breastfeeding or not, one
respondent said:
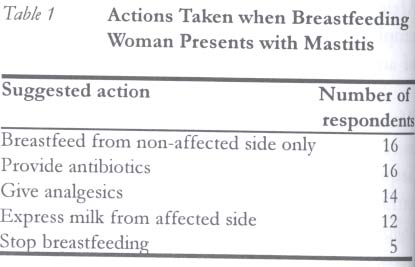
Another respondent who said she would encourage breastfeeding reported advice on cessation during teething. The reason given was: Because during teething the baby tends to have sores around the erupting tooth, which can allow HIV into the baby. One respondent reported that there is no conclusive evidence that breastfeeding could be a vehicle of vertical HIV transmission. As mastitis is identified to facilitate HIV transmission during breastfeeding, respondents were asked what advice they would give to a nursing mother with the condition. The responses are presented in Table 1. Sexuality Advice In order to determine whether antenatal attendees were advised to abstain from sex at any time by midwives, respondents were asked whether they would advise abstinence from sexual intercourse at anytime. Two respondents each said they would advise a woman to abstain from sex if she has antepartum haemorrhage, or if she has reached term. Two respondents said they would advise sexual abstinence during the whole puerperium. Perceptions and Practices towards HIV Testing HIV/AIDS prevention messages were reported to be routinely provided by 21 (80.76%) of the midwives. However, only 6 (22.22%) reported that their clinics would offer condoms to pregnant women, 16 (59.26%) would not, and 5 (18.51%) were not sure. It was reported that condoms are not usually offered as pregnant women would not feel the need for them. In order to determine the capacity for HIV counselling and testing, respondents were asked whether their health facilities had at least one trained HIV counsellor. About half (51.85%) reported having such a counsellor, 10 (37.03%) had no counsellor and 3 (11.11%) were not sure of the existence of a counsellor within their facility. Only 9 (33.33%) midwives reported conducting routine screening of sexually transmitted infections (STIs). At one health centre, antenatal clinics were being conducted in the corridors and respondents expressed unsuitability of such a site for either HIV/AIDS counselling or STI screening. However, 21 (77.78%) reported teaching ANC attendees about HIV/AIDS. We also aimed to determine midwives' perceptions about the reasons antenatal women sometimes either do not accept HIV testing or accept testing without wanting to know the results. The responses were that women were afraid of a positive result, feared losing hope and dying prematurely if they are confirmed to be HIV infected. The lack of adequate HIV counselling services was mentioned as one of the reasons women would not fully accept testing or would not wish to know their test result. In practice sometimes, women who accept HIV testing decide not to inform their spouses. Midwives' perceptions of this practice were sought. Midwives thought that women are reluctant to inform their spouses about HIV testing and seropositive results for the following reason: fear of blame that it was the woman who acquired the infection from extramarital sexual relations, fear of divorce, and fear of accusation of being unfaithful in marriage. It was reported that there is a common perception that those who go for test do so after realising their high risk sexual behaviours. A woman who decides to have an HIV test: is therefore telling others that she has been unfaithful. Spousal Support in Antenatal Clinics It has been suggested that successful PMTCT programme should endeavour to involve men. Midwives were therefore asked whether they would allow men to attend antenatal clinics with their spouses. Only 10 (37.03%) reported that they would allow men to accompany spouses, 8 (29.62%) would not and 9 (33.33%) were not sure if they would accept. The reasons provided for not involving male spouses in antenatal care services were that ANC services have traditionally been tailored for pregnant women and not men, midwives have never thought or discussed about involving men, and that men are usually busy at work at the period ANCs are conducted. For those respondents who wished that men would come to ANC, the reasons provided for such intentions were that: if men were to come to ANC they would help in ensuring that their spouses understood health information better and that midwives would cease being accused in the event of adverse neonatal and maternal outcomes. Midwives' Attitudes towards HIV-Infected Women and Babies Respondents were asked whether they thought women who know they are HIV-infected should become pregnant if they so wished. Only 3 (11.11%) thought they should, 22 (81.48%) said HIV-infected women should never become pregnant, while 2 (7.41%) were not sure. Sixteen (59.26%) indicated that they would not mind assisting in the delivery of a woman known to be HIV-infected, 10 (37.04%) reported that they would be uncomfortable assisting and 1 (3.70%) was not sure. Relating this to the availability of sterile gloves to use in assisting deliveries, only 11 (40.74%) midwives reported working in health centres with adequate stocks of gloves. However, only 9 (33.33%) always have gloves appropriate to their hand sizes. Only 2 (7.41%) reported that women should have access to ARVs even when not tested for HIV, two were not sure, while 23 (85.19%) reported that access to ARVs should only be to those who have had a positive HIV testing result. With regard to the baby, 40.74% reported that they would go ahead to give BCG to a day-old infant whose mother is known to be HIV-infected, 48.15% would not give the vaccine, while 11.1% were not sure. Discussion Midwives in Blantyre, Malawi, generally have a positive attitude towards the use of ARVs to prevent vertical HIV transmission. However, there still exist important potential impediments to preventing HIV infections among pregnant women and infants. This study reports that only 22.22% of midwives provide condoms within their facilities. As consistent and correct use of condoms during sexual intercourse is an important HIV preventative tool, lack of promotion of such intervention is a matter of concern. Bauni and Jarabi reported lack of acceptance of condom use within stable relationship. Use of condoms was associated with perceived lack of trust in the relationship.19 Perceptions that pregnant women may not need condoms should be challenged and corrected. There are general beliefs in some parts of Malawi about sexual intercourse among pregnant women; some cultures promote it, others advice abstinence, while yet others advice abstinence under particular circumstances. Only 37% of the midwives reported conducting routine STI screening, yet genital infections facilitate HIV transmission. Lack of STIs screening should be perceived as lost opportunity at ANC where some vertical HIV transmission and maternal HIV acquisition20 could be prevented if treatment for STIs were routine. Of course, it ought to be recognised that many women with STIs are asymptomatic and, therefore, will not present with symptoms.21,22 However, Wilkinson et al,23 in their study among 189 rural South African women showed that 74 (39%) of them who had not presented with symptoms to a family planning clinic admitted having genital symptoms on direct questioning. It is interesting to note, however, that just about 59% reported that they would be comfortable to assist in the delivery of a known HIV-infected woman. This certainly has implications on widespread access and use of ARV to prevent vertical HIV transmission in labour. It is possible that HIV-infected women would be stigmatised and discriminated by their professional carers. Programmes that provide ARVs for prevention of vertical HIV transmission should seriously consider this finding. In general, midwives reported high acceptance and promotion of exclusive breastfeeding even for HIV-infected women. As breast milk can spread HIV from mother to infant, any advice given whether to encourage or discourage must be as much as possible evidence-based. Nduati et al24 reported both high maternal and infant mortality in a randomised study associated with breastfeeding among HIV-infected women. The attributable risk of maternal mortality as a result of breastfeeding was 69% as compared to formula feeding. The opinions of the woman and her family must always be respected. This study reveals that sometimes advice on this subject has been confusing and conflicting. This disempowers midwives as to what advice to give to ANC attendees. Also, although exclusive breastfeeding is known to have a lower risk of vertical HIV transmission, the practice is a rarity in many developing countries.25 It is also of particular interest that about half (48.15%) of the midwives reported that they would not provide BCG vaccine to a day-old infant whose mother is HIV-infected. This is obviously in contrast to the recommendation that BCG should be given to all infants regardless of their HIV status. Only when the child has clinical AIDS can BCG be withheld. Midwives had negative attitudes towards involvement of men in ANC services. This can be explained by the belief that ANC services are for women. However, the observation that men are busy at work during ANC clinic periods is quite important. The majority of women in Malawi are housewives.26 Changing attitudes towards men attending ANC with their spouses should be viewed as just the first step. In order to ensure sustained participation of men, there is need to introduce flexible clinic schedules, make allowance for their presence and probably include male health professionals.27 The continued and significant braindrain of nurses and midwives from the country to other countries is also a significant challenge towards wide implementation of PMTCT programmes.28 In the study health centres, each of the facilities had just between two and five midwives. The reasons for the braindrain and lack of interest in midwifery in Malawi have been described by Ostergaard. 29 Unwillingness to disclose one's HIV status to the spouse remains a formidable challenge towards effective implementation of a comprehensive PMTCT programme. Twahir et al30 reported that women attending STI services in Mombasa, Kenya, were unwilling to disclose their diagnosis to their spouses for fear of being accused of bringing the infection into the home. Even though ARVs could be administered intrapartum without the knowledge of the male spouse, the subsequent decision to either breastfeed or not, have further children, and the need for behavioural change, will most likely require a spouse who is knowledgeable of the HIV status. Although most Malawian women attend antenatal services at least once during their pregnancy, delivery is usually outside a modern health facility.31 Therefore, programmes aimed at preventing vertical HIV transmission must consider this important fact. Despite its attendant formidable challenges, some programme planners have suggested the use of traditional birth attendants. 32 Acknowledgements We are greatly indebted to the nurses who accepted to participate in the study. Permission to conduct the study was obtained from the District Health Officer for Blantyre, Dr Atupele Kapito. We also thank the following research assistants: Malangizo Mbewe, Francis Kachali, Sandress Msuku, Lumbani Munthali, Staphael Kalengo and Amos Nyaka. This study was funded through a research grant from the National Research Council of Malawi (NRCM) of the Government of the Republic of Malawi. References
© Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04027t1.jpg] |
| |||||||||

{kind=link}