 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 8, No. 2, Aug, 2004 pp. 71-76 Self-Disclosure of HIV Serostatus in Recently Diagnosed Patients with HIV in South Africa BO Olley1,2, S Seedat1, and DJ Stein1 1MRC Unit on Anxiety Disorders, Department of
Psychiatry, University of Stellenbosch, Cape-Town, South Africa. 2Department
of Psychology, Faculty of the Social Sciences, University of Ibadan, Ibadan,
Nigeria.
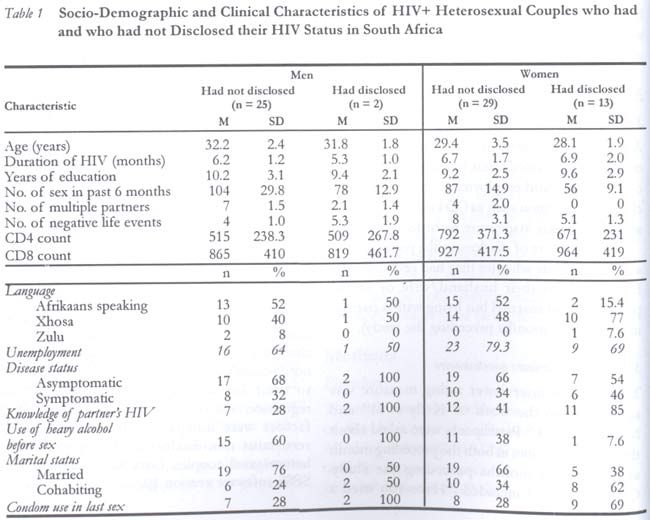
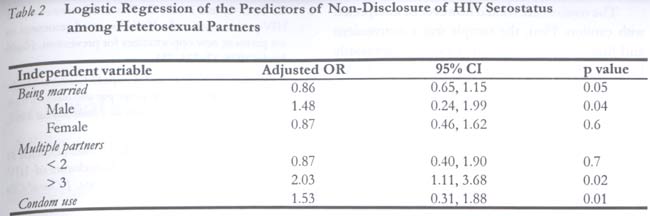
Code Number: rh04028 Abstract Failure of people living with HIV/AIDS to disclose their HIV serostatus can place their sexual partners at risk. The current study examined HIV serostatus disclosure and its relationship to risky sexual behaviours in 69 sexually active, heterosexual, married (62%) or cohabiting (38%) patients recently diagnosed as HIV positive. Results show that 78% had not disclosed their HIV serostatus to their sexual partners and 46% had no knowledge of their sexual partner's serostatus. Compared to those who disclosed their serostatus, those who did not disclose were more likely to be male (x2 = 7.02, p = 0.00), to have not used a condom during their last sexual encounter (x2 = 29.64, p = 0.000), to have used alcohol heavily before sex (x2 = 6.79, p = 0.00), to have multiple sexual partners (t = 3.01, p = 0.05), and to have engaged more frequently in sexual intercourse in the six months preceding the study (t = 8.21, p = 0.00). Logistic regression analysis show that being in a married relationship (OR = 0.86, 95% CI = 0.65, 1.15), being male (OR = 1.48, 95% CI = 0.24, 1.99), having more than two multiple partners (OR = 2.03, 95% CI = 1.11, 3.68) and non-use of condom at last sex (OR = 1.53, 95% CI = 0.83, 1.88) were significantly associated with non-disclosure of HIV serostatus. Preventive strategies among HIV- positive patients should place emphasis on the management of self-disclosure and its importance in safe sexual behaviour. (Afr J Reprod Health 2004; 8[2]: 71-76) Key Words: Self disclosure, hetrosexual couple, HIV/AIDS patients Résumé Auto-révélation de la situation sérologique du VIH chez les patients récemment diagnostiqués comme ayant le VIH en Afrique du Sud. L'nicapacité des gens vivant avec la VIH/SIDA de révéler leur situation sérologique du VIH peut mettre leurs partenaires sexuels en péril. Cette présente étude a examiné la révélation de la situation sérologique et son rapport avec le comportement sexuel à risque chez 69 patients sexuellement actifs, hétérosexuels, mariés (62%) ou qui co-habitent (38%) récemment diagnostiqués comme étant VIH positifs. Les résultats ont montré que 78% n'ont pas révélé leur situation sérologique du VIH à leurs partenaires. Par rapport à ceux qui ont révélé leur situation sérologique, ceux qui ne l'ont pas avaient plus la possibilité d'étre des mâles (x2 = 7,02, p = 0,00), de ne pas avoir utilisé un préservatif au cours de leur dernier rapport sexuel (x2 = 29,64, p = 0,00), d'avoir bu trop d'alcool avant d'avoir un rapport sexuel (x2 = 6,79, p = 0,00), d'avoir des partenaires sexuels multiples (t = 3,01, p = 0,05) et d'être engagés plus fréquemment dans des rapports sexuels dans les six mois qui ont piécédé l'étude (t = 8,21, p = 0,00). L'analyse de la regression logistique a montré qu'étant dans un rapport conjugal (OR = 0,86, 95% CI = 0,24, 0, 99), ayant plus de deux partenaires multiples (OR = 1,53, 95% CI = 0,31, 0,88) ont été liés de manière significative à l'incapacité de révéler la situation rérologique du VIH. Les stratégies préventives chez les patients séropositifs devraient mettre l'accent sur la conduite à tenir devant l'auto-révélation et son importance dans le comportement sexuel sans risque. (Rev Afr Santé Reprod 2004; 8[2]: 71-76) Introduction It would seem ethical for individuals infected with HIV to notify their sexual partners of their serostatus.1,7 Furthermore, disclosure of HIV serotstatus can help in promoting safe sex, reducing the transmission of/or re-infection with HIV.5,6,8,9 Nevertheless, there are many reasons that such self-disclosure may not occur; these include stigmatisation, isolation or abandonment, lack of social support, separation or divorce, and even prosecution.10 Indeed, data indicate that HIV-positive patients do not always disclose their serostatus and, in fact, may be ignorant of their sex partners' serostatus. Perry et al2, for example, found that almost one third of HIV-seropositive men and women had not disclosed their HIV serostatus to past or present sexual partners. Stein et al3 found that 40% of sexually active men and women living with HIV in a community sample had not disclosed their serostatus to all their sexual partners. Similarly, in a community sample, Kalichman and Nachimson4 found that 41% of HIV-positive persons had not disclosed their HIV serostatus to their sexual partners. In a study involving 206 HIV+ men of mixed sexual orientation5, 48% had not disclosed their serostatus to their sexual partners. Consistent with these findings, a recent report6 of 105 HIV+ men showed that 47% did not disclose their seropositive status to their at-risk partners. A number of these studies have also documented that many people with HIV have sex with partners who are HIV-negative or of unknown serostatus.5,6 Kalichman12 found that 42% of HIV+ men and 42% of HIV+ women reported at least one instance of unprotected sex during a six-month period, frequently with partners with unknown or seronegative HIV status. Similarly, among 48 respondents, Ciesla et al13 reported that 31.1% of HIV+ patients reported unprotected vaginal or anal intercourse with a partner of negative or unknown HIV status. Being married or having a long-term relationship has been reported to be protective of infection as well as transmitting the HIV virus; available data are however contradictory. For example, while one study reported increased risky sexual behaviour in HIV-positive patients who were married and in long-term relationships9, another study found that unprotected sexual intercourse was more frequent in unmarried individuals, those in casual relationships, and where partners were ignorant of each other's serological status.12 In one study11, 14% of male and 7% of female HIV-positive couples did not use a condom in their last sexual encounter. There are relatively few studies on disclosure of HIV serostatus and unsafe sexual behaviours among HIV+ individuals in sub-Saharan Africa. Most studies to date have originated in the United States and have been conducted among homosexual or bisexual white men.5,6,9,12,14 In sub-Saharan African countries, where the primary mode of transmission is heterosexual contact and where rates of infection and transmission of HIV are increasing daily among married persons, it is useful to document levels of disclosure among heterosexual HIV-positive individuals. For example, of all persons in South Africa infected with HIV/AIDS, the proportion of married heterosexual couples who are infected has cumulatively increased from 5% of the infected population in 1999 to 12% at the end of 2002.15 In the present report, we examined retrospectively: (i) the level of self-disclosure of HIV serostatus, and (ii) the prevalence of unprotected sex among heterosexual patients who were married or cohabiting. In addition, we examined the socio-demographic correlates of self-disclosure in these patients. Methods Procedure The study was approved by the ethics committee of the University of Stellenbosch, Cape Town. All consecutive HIV/AIDS patients who were on follow-up management were approached and included in the study. Patients were first seen by their treating physician and thereafter interviewed by a trained researcher. Included in the interview were assessments of sexual behaviour in the six months preceding the interviews and a questionnaire on socio-demographic characteristics. Participants/Setting The study sample consisted of 69 patients (27 males and 42 females) recently diagnosed with HIV (mean duration of diagnosis = 7.12 months, SD = 2.8). Patients were recruited from the outpatient infectious diseases clinic of the Department of Internal Medicine and Infectious Disease, Tygerberg Hospital, Cape Town, South Africa. Inclusion criteria were: age 18 years and above, recently diagnosed (< 1 year) HIV infection, no neurological or cognitive disorder, and willingness to give written informed consent. The hospital is one of two major tertiary health facilities in the Western Cape and receives referrals from surrounding community health centres as well as medical and obstetric/gynaecology clinics at Tygerberg Hospital. Measures Socio-demographic variables A brief questionnaire was used to collect information on age, gender, marital status, home language, years of education, and employment status. Similarly, clinical information such as CD4 and CD8 counts and HIV disease stage were recorded. As a measure of disclosure, the patients were asked to indicate whether they had revealed their HIV status to their husband/wife or sexual partner (if not married but living with a partner in the past six months preceding the study). Sexual risk behaviours questionnaire This 20-item interviewer rating measure was adapted from the work of Kelly et al16 and McKinnon et al.17 Participants were asked about their sexual activities in both the preceding month and in the six months preceding the study. Questions asked included: "Have you used a condom at last sex?" "Have you had sex with a partner who used intravenous drugs?" "Have you had sex after heavy use of alcohol or other drugs?" "Have you had sex with a partner known to you for less than one day?" Negative life events scale This was adapted18 from a scale developed by Swartz, Elk, Teggin, et al.19 It is a 42-item clinician-administered checklist that inquires about the number of life events (positive and negative) occurring during the past six months as well as the degree of stress (impact, 0-2 score). Two measures were derived: the number of events and degree of impact, with higher scores on impact signifying greater stress. Coping behaviours Coping behaviours, that is, specific styles used by HIV positive patients to deal with the stress associated with living with HIV, was assessed with the abridged version of Cope called the Brief COPE.20 Brief COPE is a 14-scale questionnaire spanning active coping, planning, positive reframing, acceptance, humour, turning to religion, venting of emotions, mental disengagement, denial, substance use, behavioural disengagement, and emotional support. Each item is rated on a four-point Likert scale: `1' = I did not do this at all to `4' = I did this a lot to the activities in the past three months. Statistical Analyses Chi-square tests for categorical variables or Student's t-tests for continuous variables were used to compare differences in socio-demographic characteristics, risky sexual behaviours and clinical characteristics of heterosexual couples who had not disclosed or who had disclosed their serostatus to their sexual partners. Multiple logistic regression analysis was then used to assess which factors were independently related to HIV serostatus non-disclosure/disclosure among heterosexual couples. Data were analysed with SPSS software version 10. Results Table 1 presents data on the 69 sexually active heterosexual patients living with HIV/AIDS. Forty three (62%) of them were married, while twenty six (38%) were cohabiting. Seventy eight per cent had not disclosed their HIV serostatus to their sex partners and 46% had no knowledge of their sex partner's HIV serostatus. The other 54% knew about their sex partner's serostatus; all of these were positive for HIV. Relatively few (64%) of these patients remembered having received counselling for HIV/AIDS. Compared to those who did disclose their serostatus to their sex partners, those who did not disclose were significantly more likely to be male (x2 = 7.02, p = 0.00), to have used alcohol heavily before sex (x2 = 6.79, p = 0.00), to have had multiple sex partners (t = 3.01, p = 0.05), to have engaged in more frequent sexual intercourse in the six months preceding the study (t = 8.21, p = 0.00), and not to have used a condom during their last sexual encounter (x2 = 29.64, p = 0.000). Further result showed that 38 (88%) of the married patients had not disclosed their serostatus to a spouse, while 16 (62%) of the cohabiting patients had not disclosed their serostatus to their sex partners. Logistic Regression Table 2 presents the predictors of self-disclosure. While adjusting for the other variables, results from logistic regression showed that being in a married relationship (OR = 0.86, 95% CI = 0.65, 1.15), being male (OR = 1.48, 95% CI = 0.24, 1.99), having multiple partners (i.e., more than two) (OR = 2.03, 95% CI = 1.11, 3.68), and non-usage of condom at last sex (OR = 1.53, 95% CI = 0.83, 1.88) were significantly associated withnon-disclosure of HIV serostatus. Discussion The results of this study provide significant findings worth considering in the implementation of preventive measures aimed at individuals infected with HIV/AIDS. Primarily, it was found that a substantial majority of heterosexual married and cohabiting men and women recently diagnosed with HIV/AIDS did not disclose their HIV serostatus and did not have knowledge of their sex partner's serostatus. These findings are consistent with previous reports,2-6 and underscore the need for more effective interventions to prevent worsening of the AIDS epidemic. In particular, it would seem important to focus interventions on helping patients and communities to increase the extent to which self-disclosure is made. Such interventions may include helping patients to alleviate the fear of negative consequences if they self-disclose their serostatus, and working with communities to destigmatise HIV/AIDS. Contrary to earlier findings,4,14 where no gender differences in disclosure of serostatus to sexual partners were observed, the present study shows that compared to women, men are significantly more likely not to disclose their serostatus to their partners. These results are consistent with the imbalance in sexual power that is often present in the developing world, and suggest that a particular focus is needed to help men with the process of self-disclosure. Consistent with previous reports,4-6 we found that among individual patients who did not disclose their serostatus to sex partners, there tended to be a higher likelihood of unsafe sexual practices including non-use of condom in their last sex, heavy alcohol use before sex, multiple sex partners, and increase in the number of sexual intercourse. One worrying finding from this study is that only 44 (64%) of the subjects remembered having received counselling for HIV/AIDS. This figure is low given that all HIV-positive patients are required to receive counselling about safe sexual practices on notification of their HIV status. Presumably, subjects did not regard the communication of information about their serological status as "counselling". There is therefore a need to enhance this aspect of clinical practice. Perhaps the need for self-disclosure was discussed but at a time or in a way that meant that it was not remembered or acted upon. In the absence of previous work examining coping styles and self-disclosure, this study investigated differences in the coping styles of patients who disclosed versus those who did not disclose. The results reveal no differences between the two groups. The number and impact of negative life events on HIV-infected individuals six months prior to study were also not associated with self-disclosure. It is possible that self-disclosure reflects a range of social factors and is not simply a product of individual psychological differences. The results here should however be interpreted with caution. First, the sample was a convenient and highly selective one that cannot necessarily be generalised to other groups living with HIV/AIDS. The study was also limited in that it relied on self-report and obtained only limited detail about what was self-disclosed and when. Most patients in this study were not on antiretroviral therapies, and the introduction of these medica-tions to South Africa may well lead to a change in disclosure patterns. Finally, the data in this study were cross-sectional, with resulting limitations in inferring causation from the associations found. Nevertheless, these data emphasise the extent to which lack of self-disclosure of HIV serostatus remains an important issue, and on the need for focusing additional attention on this issue. Acknowledgment This work was supported by the Medical Research Council of South Africa and by a SAAVI Fellowship. References
© Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04028t1.jpg] [rh04028t2.jpg] |
| |||||||||

{kind=link}
{kind=link}