 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 8, No. 2, Aug, 2004 pp. 91-100 Voluntary Counselling and Testing (VCT) for Human Immunodeficiency Virus: A Study on Acceptability by Nigerian Women Attending Antenatal Clinics EE Ekanem1 and A Gbadegesin2 1Department of Community Health, College of
Medicine, University of Lagos, PMB 12003, Lagos, Nigeria. 2Department
of Obstetrics and Gynaecology, Ayinke House Maternity Hospital, Ikeja, Lagos,
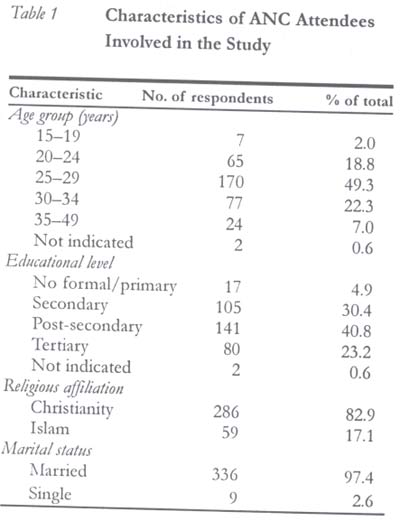
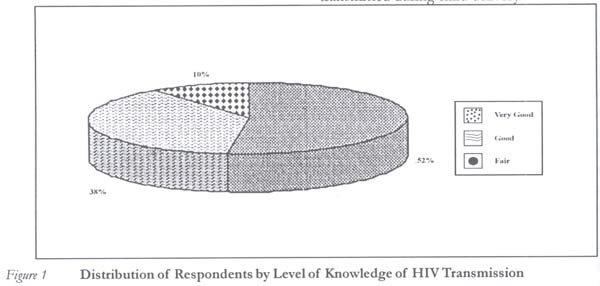
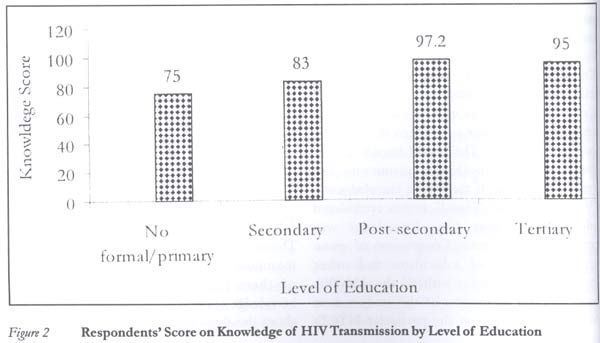
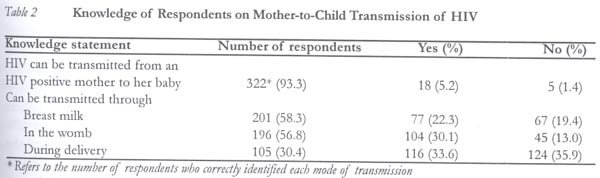
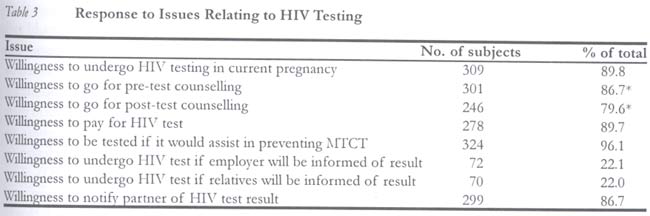
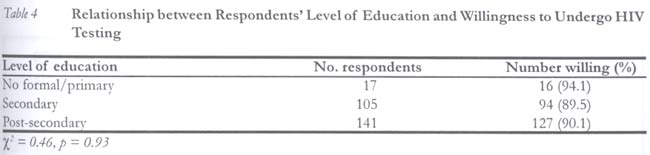
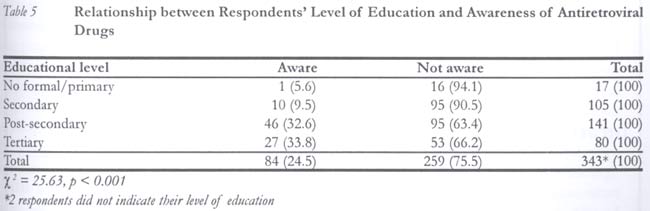
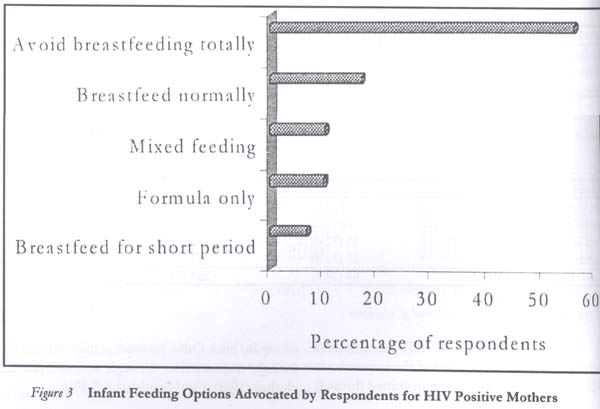
Nigeria. Code Number: rh04031 Abstract This study was carried out among 345 pregnant women attending antenatal clinics at two health facilities in Lagos, Nigeria. It was undertaken to determine their knowledge and acceptability of HIV voluntary counselling and testing in pregnancy as a strategy for the prevention of mother-to-child transmission (PMTCT) of HIV. Data were collected on issues relating to mother-to-child transmission of HIV, willingness to go for voluntary counselling and testing, actions to be taken if a pregnant woman was found to be HIV positive including infant feeding options. Majority of the women (89.9%) had good knowledge of the modes of HIV transmission, however, knowledge of specific aspects of PMTCT was poor. Close to half of the women (41.7%) were not aware of the association between breast milk and HIV transmission. Almost all the women (96.1%) were willing to undergo HIV testing in pregnancy particularly if it would assist preventing transmission of HIV to their babies; but only few would undergo the test if the result would be shared with relatives. Many of the women would still prefer breastfeeding even if they were found to be HIV positive. Awareness of anti-retroviral drugs among the study group was very poor. As the country is about to embark on its PMTCT programme, there is need to increase the level of knowledge, acceptability and adoption of VCT and other PMTCT strategies among potential beneficiaries. Innovative information and education techniques need to be developed to provide HIV positive mothers with knowledge and skills that can enable them to make informed choices about infant feeding options and other forms of care. (Afr J Reprod Health 2004; 8[2]: 91-100 ) Key Words: HIV/AIDS, voluntary counselling and testing, antenatal women, PMTCT Résumé Dépistage et conseil volontaires (DCV) pour le virus immunodéficience humaine: une étude sur l'acceptabilité par les femmes nigérianes qui fréquentent les services de consultation prénatale. Cette étude a été menée auprès de 345 femmes enceintes qui fréquentent les services de consultation prénatales dans deux établissements de santé à Lagos, Nigeria. Elle avait pour objectif de déterminer leur connaissance et leur acceptabilité des dépistages et des conseils volontaires pendant la grossesse comme stratégie de la prévention de la transmission du VIH de la mère à son enfant (PTME). Des données ont été recueillies sur les questions portant sur la transmission du VIH d'une mère à son enfant, la volonté d'aller volontairement subir des tests et de bénéficier des conseils, ce qu'il faut faire si une femme enceinte découvre qu'elle est séropositive y compris les options concerant l'alimentation de l'enfant. La majorité des femmes (89,9%) avaient une bonne connaissance des modes de transmission du VIH, pourtant elles avaient une faible connnaissance des aspects spécifiques de PTME. Presque la moitié des femmes (41,7%) n'étaient pas au courant du lien entre le lait maternel et la transmission du VIH. Presque toutes les femmes (96,1%) étaient prêtes à subir le test pour le VIH pendant la grossesse si cela aidera à éviter la transmission du VIH à leurs bébés; mais peu de femmes voudraient subir le test si le résultat serait divulgé aux parents. Bon nombre des femmes préféreraient encore l'allaitement même si elles sont séropositives. La conscience des médicaments antérétroviraux au sein du groupe étudié est très faible. Alors que le pays est en train de commencer le programme de PTME, il est nécessaire d'augmenter le niveau de la DCV et toutes les autres stratégies de la PTME chez les bénéficiaries potentiels. Il faut développer l'information innovatrices et les techniques d'éducation afin d'assurer aux mères séropositives la connaissance et la compétence qui leur permettront de faire des choix en connaissance de cause à l'égard des options concernant l'alimentation de l'enfant et d'autres formes de soin.(Rev Afr Santé Reprod 2004; 8[2]: 91-100) Introduction HIV/AIDS is a global problem whose emergence has introduced new dimensions to health care delivery wordwide. One of this is voluntary counseling and testing (VCT). It has been estimated that most of the 37 million people worldwide now living with HIV do not know that they are carrying the virus. The proportion is highest in countries worst affected by the epidemic.1 HIV is heavily stigmatised in many countries and people with HIV may experience social rejection and discrimination.2 Voluntary HIV counselling and testing (VCT) is the process by which an individual undergoes counselling enabling him/her to make an informed choice about being tested. This decision must be entirely the choice of the individual and s/he must be assured that the process will be confidential.3 Recognising the vital role that VCT has to play within a comprehensive range of measures for HIV/AIDS prevention and support, the joint United Nations Programme on AIDS encourages countries to establish national policies relating to VCT.4 The most effective intervention to reduce transmission from mother to child depends on a woman knowing her HIV status, which in turn depends upon the availability of information, counselling and voluntary service.5 VCT would therefore enable mothers to determine their serostatus before PMTCT intervention can be carried out. With the advent of zidovudine (ZDV) and other antiretroviral drugs (ARVs), mothers with HIV can prevent transmission to their infants in at least 50% of cases.6 HIV VCT has been found to be effective in changing behaviour. More than 40% reduction in unprotected intercourse among individuals who received VCT, compared to those who received health information only, has been reported.7 HIV VCT services combined with STD diagnosis and treatment and economic development services have been found to motivate at-risk individuals and couples to receivecounselling and testing.8 The family also stands to benefit when an infection is discovered early enough to permit advance planning for the financial security of the survivors. Benefits to the community flows especially when people with HIV feel safe enough to be open about their infection and become involved in the fight against the epidemic. They can then bring first-hand experience to AIDS actions and help neighbours, institutions and policymakers to face up to the reality of the epidemic.1 The knowledge of availability of treatment options has been demonstrated to affect the attitudes of people to VCT. Several studies have shown that those who knew about ZDV therapy for pregnant women were more likely to have had an HIV test than those without such knowledge.9,10 Despite the proven benefits of VCT, acceptability is variable. While some countries have recorded high acceptance rates, others have recorded very low rates.11 This study was undertaken to determine the acceptability or otherwise of HIV voluntary counselling and testing in pregnancy as a strategy for the prevention of mother-to-child transmission (PMTCT) of HIV in Nigeria. The findings should help programme managers in understanding the limiting as well as positive factors influencing VCT uptake and its potential success in the country. Materials and Methods The study was carried out in two health facilities in Lagos (General Hospital, Ikeja and Regina Mundi, Mushin). Respondents consisted of pregnant women attending antenatal clinics at these sites. Pregnant women from many areas within Lagos and beyond utilise the services of the General Hospital. Regina Mundi is a comprehensive primary health care centre patronised largely by women in the Mushin catchment area. Thus, the two settings attempted to capture women with diverse educational and social characteristics. The sample size expression n = 1/d2 * Z2pq was used to determine the minimum number of subjects to be included in the study; where Z is the value of the Z score corresponding to the level of confidence; p is the estimated proportion of respondents with any outcome attribute, q = 1-p and d is the tolerable error margin in our estimate. At 95% level of confidence, Z = 1.96 and p = 0.30, and error margin of 5%, a sample size of 323 was determined. We increased the sample size to 340 in anticipation of non-response to certain questions and the fact that we expected at least 10% of the total sample size in any cell generated in contingency tables. In all, 345 women were recruited from the two sites. An interviewer-administered questionnaire was used to collect data for the study using three trained interviewers. Majority of the questions were close-ended, while a few questions were open-ended so as to allow respondents to provide further details on some of the issues. Subjects were informed of the purpose of the study and their consent sort before the interview. The Epi Info software12 was used for data analysis. Frequency distributions were generated for all categorical variables. In testing for association in contingency tables, the chi-square statistic was used. Four-fold tables that exhibited small expected frequencies were evaluated with Fisher's exact test using the Stat-Xact software.13 Knowledge of respondents about HIV transmission was assessed using a scoring system. Every correct answer was awarded one point while a wrong answer and "Don't Know" were awarded zero point. The level of knowledge was therefore treated both as a quantitative and qualitative variable. If the level of knowledge was "Very Good" or "Good" it was considered adequate, whereas poor knowledge was considered inadequate. Comparison of mean scores by level of education and other independent variables utilised the ANOVA technique. Since the focus of this study was on MTCT, knowledge on the particular MTCT- related routes was assessed individually. Mothers who had already been tested for HIV were excluded in the analysis relating to willingness. Results A total of 345 women with ages ranging from 15 to 40 years (mean 27.7 ± 4.4 years) were involved in the study. Majority (90.4%) were between 20 and 34 years (Table 1). Christianity was the predominant religious affiliation of majority of the respondents (82.9%), and nearly all the respondents (97.7%) were married. Most of the ANC attendees had formal education and a large proportion had attained up to the secondary level education or above. Knowledge of HIV Transmission The women were generally knowledgeable about the means by which HIV is transmitted. Majority of them (52.5%) had very good general knowledge (Figure 1). Specifically, 85% knew about the three major routes of transmission, namely, sexual intercourse, blood transfusion and contaminated syringes/needles. Knowledge of mother-to-child transmission was also high. Respondents' the level of knowledge was significantly related to their level of education (p = 0.002). Ninety five per cent of those with tertiary education had adequate knowledge, while only 75% of those with non-formal or primary education did (Figure 2). Majority of the respondents (93.3%) knew of the possibility of HIV transmission from an infected mother to her baby, 5.2% indicated that transmission could not occur through this route and 1.4% did not know if transmission through such route is possible (Table 2). A little over half of the respondents (58.3%) knew that HIV could be transmitted through breast milk, 22.3% thought that HIV transmission through breast milk is not possible, while 19.4% were not sure. Knowledge of transmission during delivery was quite low; only 30.4% of the mothers knew that HIV from an infected mother could be transmitted during child delivery. Some misconceptions on HIV transmission were noted. About one third of the respondents (32%) indicated that HIV is transmitted through mosquito bites. Other prominent misconceptions include transmission through utensils (15%), clothes (10.8%) and handshake (9.8%). Perceived Susceptibility to HIV Infection Of the 345 respondents, 262 (81.6%) did not perceive themselves to be at risk of getting infected. Perceived susceptibity was significantly related to level of education (p = 0.004) but not to the age of respondents (p = 0.363) although respondents aged 30-34 years had the highest percentage of people who perceived themselves as susceptible. The more educated respondents (those with post-secondary and above) felt more at risk than their less educated counterparts. Voluntary Counselling and Testing Most of the respondents had never been tested for HIV. Of the 345 respondents, only 135 (39.2%) had been tested in the past, mostly during ANC visits in previous pregnancies. Of those who were tested, only 34 (25.2%) received pre-test counselling, 20% had post-test counselling, while 68% were informed of their test results. Counselling was mostly done by the attending physician. Table 3 shows that many of the respondents were willing to submit themselves to HIV testing in the current pregnancy, and nearly all (96.1%) were willing to be tested especially if knowledge of their status would assist in preventing HIV transmission to their babies. Of the 309 mothers who indicated willingness to be tested, 278 (89.7%) were willing to pay for the cost of the test. Confidentiality seemed to be a major consideration in undertaking the test. Most of the respondents would not want to undergo testing if results would be made available to their employers. Only 22% of the women would still submit themselves for HIV testing irrespective of whether their relations would be informed of the result or not. Majority of the respondents (92.9%) indicated their willingness to inform their husbands of their test results. Willingness to undergo HIV test was not related to religion (p = 0.37) and marital status (p = 0.83). The association between level of education and willingness to undergo testing was not clearly defined, as there was no consistent pattern (p = 0.93). While almost all (94.1%) respondents without formal or only primary level were willing, only 88.8% of those with tertiary education indicated their willingness to be tested (Table 4) Awareness of Antiretroviral Drugs Only 84 (24.5%) of the respondents were aware of the existence of antiretroviral drugs. As shown in Table 5, knowledge of the existence of these drugs was significantly and positively related to respondents' level of education (p < 0.001). Even among those with university education, only 33.8% were aware of these drugs. Infant Feeding Options for HIV Positive Mothers Two hundred and twenty seven (65.8%) of the respondents would advise HIV positive mothers to use alternatives to breast milk rather than breastfeeding (Figure 3). However, 23 (6.7%) would want the mothers to breastfeed but for a shorter period, 58 (16.8%) would prefer the mothers to breastfeed normally, whereas 35 (10.1%) would advocate for breast milk substitute. Discussion The results show that majority of the pregnant women had very good knowledge of the modes of HIV transmission. However, knowledge of specific aspects of MTCT such as the probability of transmission of the virus from mother to baby during pregnancy, delivery and breastfeeding were generally lower. Specifically, only a little over half of the respondents were aware of the fact that HIV could be transmitted through breast milk. The issue of HIV transmission through breast milk, therefore, represents an area where more awareness is required in an MTCT programme. The educational level of respondents was significantly associated with knowledge of HIV transmission. Though HIV/AIDS education has not been officially integrated into school curriculum, it is obvious that the better educated the client is, the more access she would have to information on HIV. Many of the women surveyed did not perceive themselves to be at risk of HIV infection. This may be due to the fact that these women were married and may have viewed themselves as faithful partners to their spouses. Interestingly, most of those who considered themselves susceptible were in the 30-34 years age group. While the findings of the 1999 national HIV/syphilis sentinel survey among ANC clients showed the highest age-specific HIV prevalence in the 20-29 years age group, women in this age group did not view themselves as being at risk. The gap between actual and perceived risk is a major challenge in HIV prevention campaigns. Educational level was significantly related to perceived susceptibility to HIV infection with more of those with higher educational levels considering themselves to be susceptible to HIV transmission, compared to those with lower educational qualifications. This may be as a result of the greater knowledge of the diverse modes of HIV infection, which they demonstrated. Another possible explanation may be that they engage in more risky behaviours than those of lower educational background. However, there is no study available to confirm this. A large proportion of the respondents were willing to undergo HIV test in the current pregnancy. The number willing to be tested increased to 96.1% if it would assist in the prevention of MTCT of HIV. This agrees well with the results of studies carried out in other countries9,14 and among participants who had already been tested for HIV in the past. This result suggests that HIV testing may not be as unpopular as the general impression being given particularly among pregnant women. This high rate of acceptability of HIV testing is in contrast to results obtained in Kenya where only 33% of the respondents were willing.15 It must be emphasised that the present study was based on intent to undergo testing rather than actual practice. A significant difference between intent and practice has already been established in studies in Zambia.16 Unlike the study in Zambia, there was no indication in this study that educational level affects willingness to undergo HIV testing. However, only a study on actual HIV test rate, rather than willingness to undergo HIV testing, will provide a true basis for comparison. Most of the clients who indicated their willingness to be tested gave little consideration to the importance of counselling in HIV testing. With the provision of adequate counselling, the number of people willing to be tested may increase, as studies in the US have shown.17 The fact that marital status, religion or educational level was significantly associated with willingness to be tested may suggest that it is more of an individual decision. Confidentiality was found to be an important consideration affecting respondents' willingness to be tested for HIV. Fewer of the respondents indicated their willingness to be tested if employers, neighbours or relatives would be informed of the test results. The fear of loss of employment, fear of being ostracised from the family or community may serve as possible explanations for unwillingness to be tested under the above conditions. In many settings, fear of stigmatisation, lack of available drug therapies, lack of psychological support and adequate clinical care have been reported to prevent many people from seeking testing for HIV. Cost did not seem to play a significant role in the willingness of the clients to be tested, probably indicating that most of the respondents considered the present cost of the test ($3.00) as affordable, compared to the benefits that knowledge of their HIV status could bring. However, appropriate pricing or subsidy on the cost of the test is desirable. Again, findings from this study may only reflect the concerns of the ANC attendees in Lagos, which may be quite different from the general population or other ANC attendees in other parts of the country. Surprisingly, most of the women would like their husbands to be notified of their test result. This might be a confirmation of the fact that they consider their husbands to be the most likely source of their infection. On the other hand, the women may consider their spouses as the primary source of psychological and social support and, thus, the expediency of informing them. An earlier community-based survey18 seemed to suggest that the fear of divorce or separation may prevent wives from informing their husbands of their test results especially if it turns out to be positive. Many of the women were not aware of the existence of ARV drugs, which are of much value in the MTCT strategy. Even among those with higher educational qualifications, awareness remained low. Lack of awareness of ARVs represents a very important constraint to prevention of mother-to-child transmission initiative and would deprive these women of the known gains associated with antiretroviral therapy. The disparity in the percentage of the women who would advice an HIV positive mother not to breastfeed and those who were aware that HIV could be transmitted through breast milk is noted. It should be pointed out that such advice may not necessarily be totally based on their knowledge of transmission through breast milk, but to the general practice of withholding breast milk from children when the mother is sick. The propriety of doing this needs to be emphasised in the case of HIV positive mothers but de-emphasised in other instances as appropriate. Many of those who advocated for breastfeeding even when the mother is HIV positive probably did so because of the known beneficial effect of breast milk to the baby, as promoted by the baby-friendly initiative. Some may also wrongly assume that a baby born to an HIV positive mother is already infected anyway and, therefore, choice feeding options may make little difference. In view of the strong beliefs and practices in Nigeria, which regard breastfeeding as the best means of infant feeding, most mothers, as shown in this study, would still want to breastfeed their babies. As much as it is important to respect and support HIV positive mothers in their decision regarding infant feeding, they should be well informed about the various feeding options available to prevent their infants from being infected through breast milk. The fact that only a few of those who had been tested for HIV were counselled is an indication of the fact that counselling services in the country are inadequate. Also, many health care providers are yet to fully understand the importance of counselling in HIV testing and patient management. Willingness to undergo voluntary counselling and testing as seen in this study is a positive indication that the PMTCT initiative, which is about to begin in Nigeria, will likely attract a large number of beneficiaries. There is therefore a need for health workers to be adequately trained on counselling before HIV testing for PMTCT begins in any health facility. More awareness needs to be created about the availability and use of antiretroviral drugs in HIV management and MTCT. Innovative information and education techniques need to be developed for effectively providing HIV positive mothers with knowledge and skills that can enable them to make informed choices about infant feeding options as well as other forms of care. Even among women who are currently HIV negative, such knowledge and skills would enable them and their partners to adopt means that would reduce their chances of infection. Acknowledgements We acknowledge with thanks and deep sorrow the contribution of late Dr Oluseun Soretire, who assisted in the data collection for this study but passed away a few months later. References
©Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04031t2.jpg] [rh04031f2.jpg] [rh04031f3.jpg] [rh04031t5.jpg] [rh04031t1.jpg] [rh04031f1.jpg] [rh04031t3.jpg] [rh04031t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}