 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 8, No. 2, Aug, 2004 pp. 111-124 Planning a Family: Priorities and Concerns in Rural Tanzania T Marchant1,2, AK Mushi1, R Nathan1, O Mukasa1, S Abdulla1 and C Lengeler2 and JRM Armstrong Schellenberg1,2 1Ifakara Health Research and Development Centre,
P. O. Box 53, Ifakara, Tanzania. 2Swiss Tropical Institute, Socinstrasse
57, 4002, Basel, Switzerland.
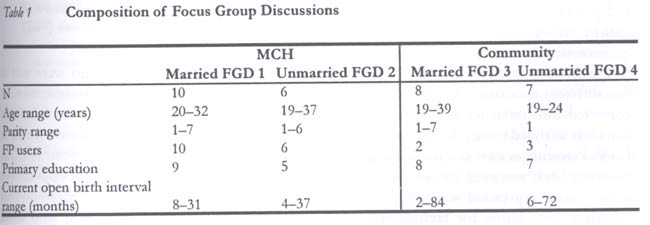
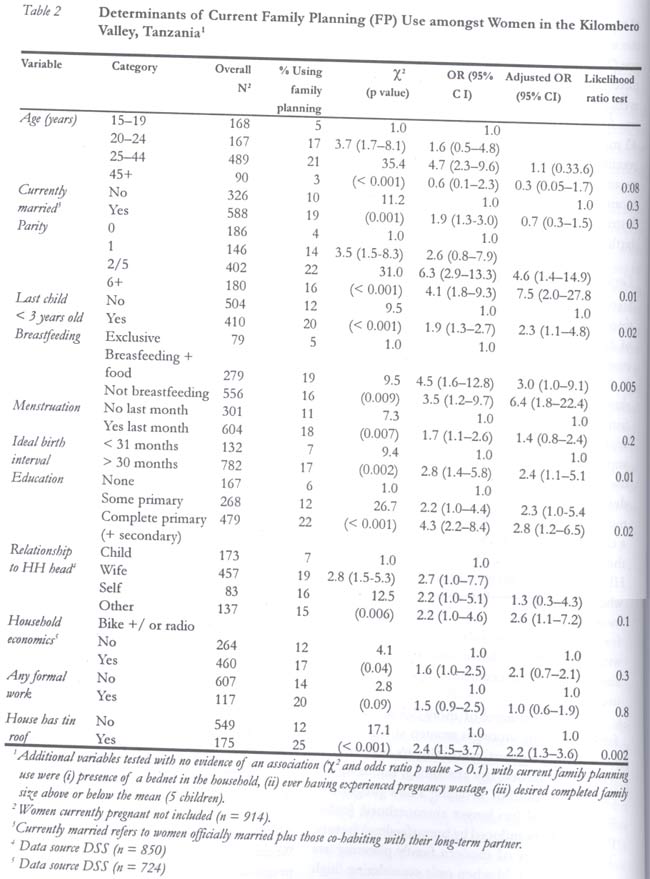
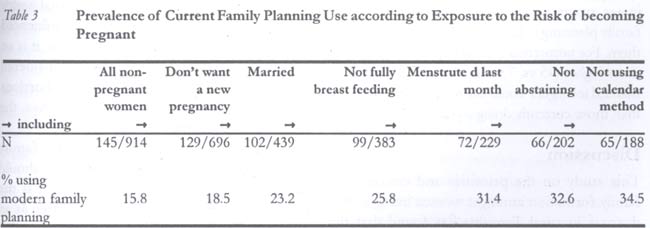
Code Number: rh04033 Abstract A fertility survey using qualitative and quantitative techniques described a high fertility setting (TFR 5.8) in southern Tanzania where family planning use was 16%. Current use was influenced by rising parity, educational level, age of last born child, breastfeeding status, a preference for longer than the mean birth interval (32 months), not being related to the household head, and living in a house with a tin roof. Three principal concerns amongst women were outlined from the findings. First, that there is a large unmet need for family planning services in the area particularly among teenagers for whom it is associated with induced abortion. Second, that family planning is being used predominantly for spacing but fears associated with it often curtail effective use. Third, that service provision is perceived to be lacking in two main areas — regularity of supply, and addressing rumours and fears associated with family planning. Reproductive health interventions in the area should ultimately be more widespread and, in particular, abortion is highlighted as an urgent issue for further research. The potential for a fast and positive impact is high, given the simplicity of the perceived needs of women from this study. (Afr J Reprod Health 2004; 8[2]:111-123 ) Key Words: Tanzania, fertility, family planning, teenagers, abortion Résumé La planification d'une famille: priorité et soucis dans la Tanzanie rurale. Une enquête sur la fertilité menée à l'aide des techniques qualitatives et quantitatives, a fait une description d'un cadre d'une haute fertilité (TFR 5.8) en Tanzanie du sud où l'emploi de la planification familiale était actuellement de 16%. L'emploi courant était influencé par la parité en hausse, le niveau de l'éducation, l'âge du dernier enfant, le statut de l'allaitement, la préférence pour une durée plus longue de l'intervalle de naissance moyenne (32 mois), le fait de ne pas être un parent du chef de la famille et le fait que l'on habite dans une maison à un toit d'étain. L'étude a précisé trois principaux soucis chez les femmes. D'abord, il y a un grand besoin non-satisfait des services de planification familiale dans la région, surtout parmi les adolescentes pour qui ils sont liés à l'avortement provoqué. Deuxièmement, qu'on se sert de la planification surtout l'espacement des naissances mais les craintes liées à la planification familiale entravent l'emploi effectif. Troisièmement, que la prestation des services n'est pas perçue comme étant suffisante dans deux domaines principaux — la fréquence de la prestation et les tentatives de resourdre les problèmes de rumeurs et des craintes liées à la planification familiale. Les interventions sur le plan de la santé publique dans le domaine devront être en fin de compte beaucoup plus répandues; et nous avons surtout précisé que l'avortement est un problème urgent qui mérite davantage des recherches. Il existe le potentiel pour un impact rapide et positif, étant donné la simplicité des besoins aperçus des femmes, d'après cette étude. (Rev Afr Santé Reprod 2004; 8[2]:111-123 ) Introduction There are good reasons to believe that Tanzania is headed towards a fertility transition as experienced in other East and Southern African countries.1-6 Steady small reductions in the total fertility rate (TFR) are evident over a ten-year period, from 6.5 in 1988 to 5.6 in 1999, and the decline is characteristically led by more urban and educated women. Demand for children remains high at present, with the average desired family size around five children. But steadily rising levels of modern contraceptive use nationwide (from 6% to 16% of women between 1991/92 and 1999) suggests an increasing desire to manage fertility and reduce the currently high number of unplanned pregnancies.4 In 1994, Tanzanian policy changed to allow all sexually active persons access to family planning services.7 Particularly, this should address the inclusion of young people and people who had not yet started childbearing. However, ever-use of modern methods amongst teenage girls remains low (10% in 1999) despite the fact that 53% have been sexually active.4 Opposition from religious and community leaders often exacerbates the difficulties of implementing policies that aim to improve the sexual health of young people through education and provision of family planning services.2 Even within the health care system it has been suggested that some moral reluctance to provide family planning services to unmarried people exists.2 During the 47th session of the WHO Regional Committee for Africa, 10 objectives with specific targets were set for easing the burden of reproductive illnesses for the period 1998-2007.8 Objective 6 is: "to reduce the levels of unwanted pregnancies in all women of reproductive age" with a specific promotion of research which "reviews or undertakes opera-tional research on barriers to family planning services". In Tanzania, it has been estimated that only 56% of the total demand for family planning is currently being met, and that during the period 1994-1999 one in five births was not wanted or was considered untimely by the mother.4 A large part of the unmet need in Tanzania is due to difficulties in geographical availability and supplies.9 However, it has been argued that provision of family planning should reach further than the conventional boundary of access and should address knowledge, fear of side effects and social and familial disapproval of family planning at the community level.10 This service is largely absent in Tanzania - eight out of ten non-users in 1999 said they had been offered neither information nor family planning services in the last year.4 An analysis of the prospects for further fertility decline in Tanzania by Hinde and Mturi5 led the authors to conclude that such a decline would be largely dependant on the performance of the National Family Planning Programme - initially by meeting the unmet need already present. In some regions, for example, Morogoro Region, this unmet need would represent a doubling of the contraceptive prevalence from 16% to 33%.1 In order to assist in this goal it is important to make in-depth analysis of local level motivations from a variety of settings - particularly rural areas where three quarters of the women of reproductive age are living4 - with which to inform national level implementation policies. In the rural Kilombero Valley, within Morogoro Region, there are an increasing number of outlets for family planning under-development. However, despite this effort to increase service provision, there is a dearth of knowledge as to the current fertility levels and, perhaps more importantly, there is little information on the desires and needs of women in this area. We therefore carried out a study to describe fertility in the area, to identify the concerns of women during the process of family formation and to identify how best they would like to be served. Study Area This project was based at the Ifakara Health Research and Development Centre (IHRDC), in the Kilombero Valley of southern Tanzania. The centre started a demographic surveillance system (DSS) in Kilombero and Ulanga Districts in September 1996, which operates in 25 villages with 65,000 people living in approximately 12,000 households. Information on births, deaths, immigration and emigration is updated for the population every four months and from time to time special surveys are administered, e.g., on socio-economic status. The DSS provides a full sampling frame for in-depth studies within the area.11 Both districts are rural, and subsistence farming of rice, maize and cassava is practiced; fishing is also common. Up to one third of houses in the area have brick walls and corrugated iron roofs; many of the remainder have mud walls and thatched roofs. There are no paved roads. About 40% of the population are Muslim and 60% Christian. Each village has at least one primary school and there is one secondary school. The public health system has a network of village health workers, health posts, dispensaries, health centres and hospitals with varying quality of care. Nine of the 25 villages included in the study area have a government health facility: in total there are eight dispensaries and two health centres. Family planning services are available at all of these. There are additional three mission health facilities in the area, which do not provide family planning services. There are also two hospitals outside the study area, but within the range of health facilities accessed by the study population. In Ifakara, the Kilombero District capital, is a well-equipped mission designated district hospital, and in Ulanga District capital, Mahenge, is a more limited hospital. The mother and child health (MCH) clinic services are well developed and vaccination coverage is high, with 78% of children receiving all Expanded Programme on Immunization (EPI) vaccines by age one year. Methods Data Collection Data for this study were collected using qualitative (focus group discussions) and quantitative (questionnaire survey) methods as well as through a review of the DSS data. Focus group discussions Four focus group discussions (FGDs) were held at the beginning of the project in order to identify local terminologies, attitudes and priorities in relation to family formation (Table 1). Two FGDs were held at a MCH with integrated family planning services to select only family planning users, and two in a neutral setting without specific selection for family planning use amongst community members of the same village (Kibaoni). In each setting there was one group each of married and unmarried women. All participants had at least one child. The FGDs were conducted in Swahili with a trained and experienced moderator who probed participants on the ideal tempo and quantum of fertility, fertility decision-makers, economic problems, problems in achieving fertility ideals, and the perceived health sector needs for women trying to plan their fertility. The discussions were taped-recorded, transcribed and translated into English. Themes emerging from the focus group discussion were analysed by manual content analysis and where appropriate the findings were incorporated into the design of a questionnaire. Questionnaire A quantitative questionnaire was undertaken in all 25 DSS villages in May 1999. A random sample of approximately 1000 women aged 15-55 years, stratified by village, was drawn. The questionnaire included a detailed pregnancy history, ideal tempo and quantum fertility questions, history of current and ever-use of family planning, and open-ended questions about the fears associated with use of modern methods. DSS Data Using the unique person identification numbers assigned by the DSS, additional data on socio-economic status and position in the household were extracted from the DSS files and merged with data from the questionnaire. Data Analysis FGD data were analysed manually and the topics and perspectives emerging summarised by the author and a social science researcher. All questionnaire data were double-entered in FoxPro (Microsoft Corporation, Seattle, WA, USA) by two different data entry clerks, and errors were corrected with reference to the original forms. Data was analysed using STATA (version 7, TX, USA). Percentages were compared using x2 tests. Student's t-test was used for comparing means, while logistic regression was used to calculate adjusted odds ratios for factors influencing current family planning use where variables had a x2 or unadjusted OR p value < 0.1. Results Priorities and Concerns Highlighted by the Focus Group Discussions In response to the questions and probes of the moderator, the three most important and consistent themes that were raised by participants across the FGDs were induced abortions, the economic burden of parenting, and service provision needs. Induced Abortions The perception of an increase in the number of induced abortions All the focus groups had strong feelings about this topic. The tone of discussion was one of a shared burden for women and feelings of sympathy for those who found themselves with unwanted pregnancies. The main risk group was considered to be teenage girls and was most visible amongst schoolgirls from primary five/six onwards. The struggle and commitment required by parents to send their children to school was emphasised and, in the event of a pregnancy, the terrible disappointment and shame experienced by the whole family, as a schoolgirl who becomes pregnant is obliged to leave school. You may find a girl who has almost completed primary when she realises that she is pregnant. With the consent of her mother she can make private arrangements with a doctor. When it is all over she can continue with her education. (FGD 3, married, 36 years) Even for teenage girls who were not at school, induced abortions were considered to be a growing problem. Rejection by the father, and the threat of rejection by her parents, would be adequate reason for a girl to attempt an abortion. Without the support of mothers the options open to young girls were to visit local `grandmothers' (often traditional birth attendants) who would attempt to carry out the abortion, to drink traditional herbs, or take large quantities of chloroquine or the contraceptive pill. When a girl realises she is pregnant she will respond by drinking large quantities of chloroquine tablets to end the life of the child or even her own life to avoid disappointing her parents. (FGD 1, married, 29 years). Unanimously, women considered that increases in the cost of bringing up children (particularly food, clothes, health and education related costs) were the root cause of the increase in induced abortions. It is true that the community does not condone the practice (of induced abortion) - a person can die just trying. But some people are forced to see the sense in making such a choice and they quietly praise the girl who has successfully aborted. They consider her to be clever because she has survived a great explosion in her life. (FGD 3, married, 39 years) Economic Burden The lack of shared responsibility by fathers of children That men display a lack of responsibility towards their children and the mothers of their children was virtually unanimously agreed upon, although some concession was made for `educated men'. Participants perceived that men are ignorant of the cost of living. Whenever a wife complains of not having enough for her family the husband will compare today to the time he was born, when a piece of black cloth was hardly available for dressing. He will tell his wife that now, when there are a lot of clothes available everywhere, he doesn't see why he shouldn't have many children. (FGD 3, married, 26 years) Respondents reported that the husband is the official decision-maker regarding fertility issues in marriage. All married women attending the FGDs said at least once their preferred fertility choice had been overruled (principally related to the timing of births). The women agreed that close birth intervals pose a great danger to the health of both mother and child, and make the mother less productive economically. However, most of them felt that preventing pregnancy against the husband's wishes is a more dangerous behaviour. Without a small baby or a new pregnancy to occupy him the man may direct his attention and resources towards other women. When a child is five years old he can walk with me to the farm. But how does one work with a baby under three years who must be carried on the back? The problem for married women is that five years is too long for a husband to agree. A woman can plan anything she likes regarding her family building but if her husband doesn't like it then it is all useless. (FGD 2, unmarried, 32 years) In the FGDs both married and unmarried women agreed that the ideal birth interval is between three and five years (with the exception of FGD 4 whose members did not want to discuss having another child). This was considered optimal for work, adequate childcare and the maintenance of health and beauty of the mother. However, some participants felt that a married woman who is not pregnant or breastfeeding is in danger of inciting jealousy in her husband. Jealousy is a big hindrance (to family planning) as the husband will think that other men can be attracted to his wife's beauty when he notices the physiological changes which occur in her when she has rested. In this case he will demand that they try for a new pregnancy immediately. (FGD 1, married, 29 years) Unmarried women attending the FGDs had never married. There was a striking difference between the two unmarried groups in their attitudes to their situation. The older women (FGD 2) talked about how proud they were to be taking care of their children without the help of a man, but the younger women (FGD 4) concentrated more on the parental disapproval, shame and subsequent lack of choices open to them. So many things are caused by poverty. Some children are born unplanned because a girl may go to somebody to beg for a piece of soap. She will get the soap but she will have to pay for it in some way or other. (FGD 4, unmarried, 21 years) However, all unmarried mothers concurred that they received no support from the father(s) of their child(ren), and being a single parent exacerbated the poverty experienced by other members of the community. The thing about being a single mother is that we have so many things to take us away from work. Because of this we are the ones who sleep hungry at night and our children are those who miss their education. (FGD 2, unmarried, 26 years) Service Provision Needs Improvements needed in family planning services This topic was addressed in response to a direct question about how current family planning services could be changed. The women in the FGDs raised two distinct issues. There was no apparent conflict of opinion, but not all women contributed to the topic. The first was a lack of clear information about the methods of family planning available, with a more general discussion about which methods of family planning the FGD members thought were suitable or not. This was seen as an obstacle to building confidence in women who had already adopted a method and was thought to be the principal reason for discontinuation of method use by some. Lack of clear information was also a deterrent to potential family planning adopters who might hear many mixed messages. The women said that their biggest problem was the many rumours within the community concerning side effects of different methods, which were never addressed at the point of service delivery. Too often women were just told not to worry. Some women find that they bleed continuously when they start using family planning and those who face this kind of experience are the ones who discourage others; always bad news travels faster than good. (FDG 3, married, 24 years) The second problem was supply-related. Irregular supplies at family planning outlets was considered a major obstacle. An interruption in supply was said to be of particular concern for women using family planning methods in secret. Family planning services in the area are commonly integrated within mother and child health (MCH) clinics and women often use their last child as an excuse to visit the clinic once every three months as required for hormonal supplies. Indeed, some participants described complicated measures for using family planning in secret, such as leaving pills with a friend who would bring them to the well each evening when collecting water, and using code words such as `karanga' (peanuts) between friends when discussing supplies. Repeat visits in quick succession (to check whether supplies had arrived) would arouse suspicion in the husband and become difficult to justify. In addition, inability to get supplies from an outlet other than the regular one (for example, when travelling) was raised. There was a call for services to be expanded in terms of coverage rather than the range of services provided. It would be very good if a way could be devised for services to be provided everywhere. A person may be away on a journey when the date for a repeat injection comes, yet she is likely to be denied the service because her card remains at her usual clinic. We should be able to get the service wherever we happen to be. (FGD 1, married, 32 years) Quantitative Analysis Data were collected from 1,018 women with the use of a questionnaire. One hundred and eighty (18%) of them reported no pregnancies and 204 (20%) had had no live birth. The quantum and tempo of fertility was found to be typical for a high fertility setting. Median age at first birth was 18 years (interquartile range 16, 20), while 92% (768/831) of those aged 20 years or above were mothers. Only about 4% (4/93) of women aged 45+ years were childless. Mean preferred family size was five children (SD 2.0). The total fertility rate (TFR) for women aged 15-49 years over the three-year period prior to survey was 5.8 and the average parity of women aged 45+ years at survey was 6.0. The preferred mean birth interval was 43 months (SD 13.6) with 86% of all women wanting birth intervals over 36 months. Actual mean birth interval length for all women was 32.5 months (SD 0.3) when valid birth intervals were restricted to those opening and closing with a live birth within five years.12, 13 Current use of modern family planning methods Sixteen per cent (145/914) of non-pregnant women were currently using a modern method of family planning: depo provera 7% (63/914), contraceptive pills 5% (42/914), condom 2% (23/914) and tubal sterilisation 2% (17/914). Variables showing evidence of an association with current family planning use are presented in Table 2. After adjustment, being at higher parity was the most important determinant of current family planning use. Breastfeeding status was also an important determinant with exclusively breastfeeding mothers least likely to be users. The odds of being a current user was influenced by relationship to the household head (HHH): children of the HHH were least likely to be users while women who were not immediate family members were most likely users. Educational level, a preference for longer birth intervals, and living in a house with a tin roof (a relative wealth indicator) were also important determinants of family planning use. There is evidence of more deliberate use of family planning amongst women at high risk of becoming pregnant according to behavioural (currently married, not abstaining, not using the calendar method of avoiding a new pregnancy) and biological (no longer amenorrhoeic [either postpartum or induced by breastfeeding) factors. The prevalence of modern family planning use increases two-fold when only considering `high risk for an untimely new pregnancy' women (Table 3). Ever-use In total, 461 (45%) respondents had ever tried to avoid pregnancy using any means, including abstinence, traditional methods and the calendar method. Two hundred and ninety four (29%) of all women had ever used a modern method of contraception and 19% (57/294) of these had tried more than one modern method. One hundred and seventy women (17%) had ever tried the contraceptive pill, 129 (13%) depo provera, 36 (4%) condoms and 17 (2%) tubal sterilisation. Seventy six per cent (109/144) of unmarried women had decided to use a modern method while 15% had been advised by a nurse or doctor. Amongst married women, 46% (146/317) had decided, 33% (104/317) were advised by their husband and 17% (55/317) took the advice of a nurse or doctor. Acceptability of methods There was a difference in perceived acceptability of each method by age group of respondent (x2 p value < 0.001), except for the traditional method for which there was no difference by age. The pattern of acceptability by age for depo-provera and pills was a typical age-specific fertility shape, lowest at teenages, peaking at around 45% in the 20-29-year age group, and declining thereafter. The calendar method (peak at 30%) and condoms (peak at 19%) followed the same pattern. Forty five per cent of teenage respondents considered abstinence to be acceptable, with a steady decline in perceived acceptability for each subsequent age group to 28% in the 40+ years age group. Tubal sterilisation had the reverse pattern with less than 5% of teenagers finding it acceptable with a steady increase to 32% among women older than 40 years. Justifications and considerations: starting a method Women who had ever chosen to avoid a new pregnancy agreed that their main reasons for avoidance were: (1) to ensure a birth interval of more than 24 months 65%, (2) to finish breastfeeding the last child 41%, (3) to take care of her own health 35%, (4) because her husband wanted to space 16%, and (5) to stop bearing altogether 16%. The main considerations when choosing which method to use were safety (especially referring to maintenance of future fertility) 38%, whether husband would agree with the method 13%, secrecy 11%, having no other choice 10% and cost 9%. For each method, safety was the most important consideration, with the exception of tubal sterilisation for which preservation of the woman's health was most important. The second most important reasons for choosing each method includeed no other method available (abstinence), compliance by the husband (the contraceptive pill, the condom, traditional and calendar methods) and secrecy (depo provera). Reasons for stopping a modern method One hundred and seventy four women had ever used a modern method of family planning but were no longer doing so. Their reasons for stopping were: (1) 39% wanted a new pregnancy; (2) 24% experienced side effects (including disruption of the menstrual cycle); (3) 10% had no money to pay for supplies; (4) 9% stopped because of their husband; (5) 6% stopped because of a shortage of supplies; (6) 4% stopped for fear of side effects; (7) 4% because of an accidental pregnancy; and (8) 3% stopped when menopause started. Family planning fears All women were asked what they feared most about the different modern family planning methods in turn. Their fears could be summarised under five main headings.
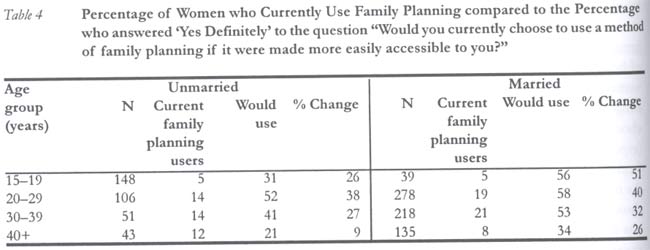
1. The fear of a method impairing the woman's own health — included the specific fears of developing cancer, stomach ulcers, increasing blood pressure, causing pain in the womb and, in the case of condoms, infection with the HIV. 2. A method not being nice or acceptable to use —included the difficulty in keeping it secret, easy to forget (especially pills), concerns that pills would not dissolve properly inside the body, that condoms would get stuck inside the vagina, or that the man would not use the condom properly. 3. Fears of method failure were exclusive to condom use. 4. Fears associated with the limitation of future fertility were almost exclusively concerned with damage done to the uterus that would not be detected until much later. This would manifest in long delays in conceiving again, destroying all the eggs inside a woman and causing infertility for some women, and causing problems in subsequent deliveries. The general consensus was that hormonal methods in particular are not suitable for all women and should not be used for prolonged periods. Median duration of use by current users of hormonal contraceptives was seven months (interquartile range: 3,15). 5. Affecting the menstrual cycle — referred to experiencing more painful menstruation, having continuous bleeding, or the total absence of bleeding. Associated fears of disruption to the menstrual cycle were related to damage to future fertility potential, and to discovery of family planning use by the husband. Unmet need Despite these fears, there was a striking unmet need for modern methods of family planning especially amongst teenagers (Table 4). Appro-ximately three times the number of current users in age groups over 19 years said they would use family planning if it were more easily accessible to them. For unmarried teenagers, this figure was six times higher (45 vs. 7 women), and 11 times more married teenagers would like to use family planning than those currently doing so (22 vs. 2). Discussion This study on the priorities and concerns of family formation amongst women living in two districts in rural Tanzania has found that the current tempo and quantum of fertility is typical for a high fertility setting and use of modern contraceptives is low. Four principal areas have been highlighted, namely, the unmet need of teenagers, adoption of family planning for spacing, obstacles and fears associated with family planning use at the community level, and obstacles in service provision. Unmet need for family planning and a strong desire to control birth intervals was evident from both qualitative and quantitative data, and was particularly urgent amongst teenagers. They were clearly experiencing pregnancy (32% of them were either mothers or currently pregnant) and 50% of teenage mothers were not married. In addition, in the FGDs the women raised concerns about a perceived increase in induced abortions amongst teenagers. These concerns were not investigated in the questionnaire, since although abortion in Tanzania is legal on maternal health grounds, in this area, which is strongly influenced by both the Christian church and Islam, it is an especially sensitive topic. It was considered inappropriate to investigate induced abortions using such a broad questionnaire; however, the topic deserves further research. The relevance of addressing the family planning needs of teenagers in this area should not be underestimated simply because it is the norm for women to start bearing children at an early age. The increased risk of infant mortality associated with teenage motherhood and with short birth intervals (which often arise from unplanned pregnancies) has been well described.14 Furthermore, there is a current emphasis in reproductive health literature on the changing needs of teenagers in this era of HIV transmission.15 An additional problem that is not always linked to reproductive health strategy is that of malaria and its associated anaemia. These are highly prevalent in this study area as in many sub-Saharan environments. It is well-established that malaria and anaemia have deleterious effects on the health of both the mother and the newborn, and that these effects are most pronounced amongst primigravidae.16,17 The effectiveness of preventative public health tools (such as insecticide-treated nets and iron prophylaxis) would be maximised if used early or even pre-pregnancy, and as such the planning of pregnancy should be seen as an appropriate goal for workers across the health sector. The second major issue raised by this study is that at present family planning is used predominantly for spacing in this high fertility setting. Data from the FGDs show a strong preference for birth spacing of 3-5 years while quantitative data show rising prevalence at middle parities, rising prevalence according to risk of exposure via the proximate determinants of fertility, and short median duration of use. This pattern has been recorded as typical in other sub-Saharan settings.18-20 However, the adoption of family planning for spacing during the early stages of fertility transition should not contradict unmet need for family planning amongst women who are yet to start bearing. Even in such a rural setting, we have found evidence that women have a relatively sophisticated approach to choosing and using the methods available to them. Family planning use should be equally as dynamic for nulliparous women as it is during the childbearing years. The single biggest fear of family planning use was the extent to which it could damage and as such limit a woman's future fertility potential (37% of all responses). However, the positive influence of the socio-economic variables on family planning use - increasing education, preference for long birth intervals and living in a house with a tin roof - may be indicative of a changing response to fertility regulation.19,21 Marital status had little impact on family planning adoption after adjustment for other factors. Ten per cent non-pregnant mothers in this study had never married and their family planning prevalence was similar to currently married mothers (18% vs. 20%). However, both the qualitative and quantitative data show that men have a strong influence over fertility decisions and some women were using family planning secretly. The fact that fathers wanted to be the fertility decision-makers but were not inclined to contribute to the economics of childcare was considered too sensitive to address directly in the questionnaire. Open-ended questions about reasons for choosing different methods of family planning and reasons for stopping methods of family planning did highlight the need for secrecy amongst women and the influence husbands had over fertility behaviour. Fertility behaviour according to marital status in this area should be investigated further. There were clear differences in perceived acceptability of methods for women in different age groups. Most strikingly, older women were less likely than younger women to accept abstinence, the calendar method and condoms. Acceptability of hormonal methods followed a very similar pattern to that of a typical age-specific fertility schedule in a high fertility setting — they were thought to be most acceptable by women in the middle of childbearing with depo provera also acceptable to women at the end of childbearing. However, it is difficult to say whether such perceptions stem from the women themselves or from service providers. The perceived low acceptability of hormonal methods for young women in particular is likely to be strongly influenced by reluctance of the service providers to encourage family planning use in this group. Service delivery problems together with fear of (or actual) side effects accounted for 44% of all the reasons given by women who had stopped using modern family planning. Only 39% stopped because they wanted a new pregnancy. Fears or rumours of problems associated with family planning use were highlighted in both data sources. None of the issues highlighted in this research need to be considered as applying exclusively to the Morogoro Region of Tanzania. The problems and needs described could equally apply to women in any resource-poor setting with poor communication and limited delivery channels. In light of the apparent unmet need for services here and throughout Tanzania1 this problem should be addressed with more accessible community education in conjunction with better information at point of delivery. Family planning providers nationwide have an essential role to play in dispelling myths about family planning use by preparing women realistically for the physical changes they might experience when adopting a new method. A concerted effort by reproductive health actors now could make a large difference to the way in which women manage their fertility. In summary, this study has highlighted real concern amongst women for the good reproductive health of teenagers in this high fertility rural setting. Some cultural problems have been identified which are perceived to exacerbate the difficulties women face when building a family. But, perhaps most importantly, a clear message of unmet need for more widely accessible family planning services, together with information that specifically addresses rumours and fears, has been delivered and should be invested in as a priority. Acknowledgements We thank the women who participated in the study. This research project was carried out within the framework of the KINET project, a collaborative project built on local and international partnerships, which implements a social marketing programme for insecticide treated nets. We are grateful to Dr H Mshinda, the Director, and staff of the Ifakara Health Research and Development Centre for facilitating the study, Drs F Lwila and P Mbena (Kilombero and Ulanga District Medical Officers) and the MCH Kibaoni clinic staff. Thank you to Marcel Tanner for his support, Chrisostom Mahutanga, and to Caroline Jones for comments on this paper. Financial support was provided by the Swiss Agency for Development and Co-operation and the Government of Tanzania. T Marchant also received support from the Rudolf Geigy Foundation. References
©Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04033t2.jpg] [rh04033t3.jpg] [rh04033t1.jpg] [rh04033t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}