 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 8, No. 2, Aug, 2004 pp. 137-144 Missed Opportunities: Emergency Contraception Utilisation by Young South African Women Mmabatho Margaret Mqhayi1,2, Jennifer Ann Smit1,2, Margaret Lynn McFadyen2,3, Mags Beksinska1, Cathy Connolly4, Khangelani Zuma4 and Chelsea Morroni5,6 1Reproductive Health Research Unit, University
of the Witwatersrand. 2Africa Centre for Population Studies and
Reproductive Health. 3Pfizer Global Research and Development,
Sandwich, United Kingdom. 4South African Medical Research
Council. 5Women's Health Research Unit, University of Cape Town. 6Fogarty
AITRP, Columbia University School of Public Health, New York, South Africa.
Code Number: rh04035 Abstract Although contraceptives, including emergency contraceptives, are widely available free at public health facilities in South Africa, rates of teenage and unintended pregnancy are high. This paper analyses awareness and utilisation of emergency contraception amongst 193 young women (aged 15-24 years) attending public sector health facilities. Structured interviews were held at 17 and 14 primary health clinics in an urban and a rural area respectively. Respondents were asked about their knowledge of contraceptive methods and use, and specifically about emergency contraceptive utilisation. More sexually active young urban women (76%) were currently using a method of contraception, compared to the young rural women (53%). Only 17% had ever heard of emergency contraception, although significantly more in the urban area (p = 0.005) had heard of it. Only one woman from each site had ever used emergency contraception, although 39% had had unprotected intercourse in the previous year when they did not wish to conceive. Young South African women should be the focus of interventions aimed at improving awareness of the availability of emergency contraception and knowledge about its correct utilisation. (Afr J Reprod Health 2004; 8[2]: 137-144 ) Key Words: Emergency contraception, youth, knowledge, practice, unplanned pregnancy, South Africa Résumé Occasions manquées: ultilisation de la contraception d'urgence par les jeunes femmes sud-africaines. Bien que les contreceptifs, y compris les contraceptifs d'urgence soient généralement disponibles et à titre gratuit dans les établissements de santé publics en Afrique du Sud, les taux de grossesse chez les adolescentes et de grossesses non-voulues sont élevés. Cet article fait une analyse de la conscience et de l'utilisation de la contraception d'urgence chez 193 jeunes femmes (âgées de 15 à 24 ans) qui fréquentent des établissements de santé du secteur public. Des interviews structurées ont eu lieu dans 17 et 14 centres de santé primaires dans un milieu rural et un milieu urbain respectivement. Les répondantes ont répondu aux questions sur leur connaissance des méthodes et de l'utilisation des contraceptifs et surtout sur l'utlisation du contraceptif d'urgence. Il y avaient plus des jeunes femmes rurales sexuellement actives (76%) qui utilisaient actuellement une méthode de contraception comparées aux jeunes femmes rurales (53%). Il n'y avait que 17% qui avaient jamais entendu parler de la contraception d'urgence, bien qu'un nombre plus important dans le milieu urbain (p = 0,005) en aient jamais entendu parler. Il n' y avait qu' une seule femme de chaque milieu qui ait jamais utilisé une contraception d'urgence quoique 39% aient eu des rapports sexuels non-protégés au cours de l'année précédente, quand elles ne voulaient pas avoir des enfants. Il faut que les interventions qui visent l'amélioration de la conscience concernant la disponibilité de la contraception d'urgence et la connaissance de la bonne utlisation de la contraception soient concentrées sur les jeunes femmes sud-africaines. (Rev Afr Santé Reprod 2004; 8[2]: 137-144) Introduction Unplanned pregnancies among young women are a worldwide problem with social and economic repercussions for the unprepared young indivi-dual.1,2 In South Africa, 35% of teenage girls are reported to be pregnant by the age of 19 years.3 Teenage pregnancy rate is high despite a relatively high reported contraceptive prevalence among 15-19-year-olds, with 64% of sexually active young women in this age group reporting current use of a modern contraceptive method.3 Although legal choice of termination of pregnancy has been available in South Africa since February 1997, problems have been experienced in implementation due to provider resistance,4 and services remain inaccessible to many women, especially younger women and those from rural areas.5 Sub-Saharan Africa is also facing catastrophic proportions of HIV epidemic, with the highest incidence of new cases in young women. HIV seroprevalence among South African women under the age of 20 years was found to be 15.4% in 2001.6 The current South African government is supportive of reproductive health rights and expanding contraceptive choice. The new contraceptive policy has been influenced by the need to use barrier methods, such as the male and female condom, to attempt to reduce the incidence of sexually transmitted infections (STIs) and HIV as well as unwanted pregnancy. Emergency contraception (EC) is an important backup method when barrier methods fail.7 In South Africa, EC is most commonly available in the form of "cut-up" ovral-28® oral contraceptive pills, and less widely (due to cost) as dedicated progesterone-only or combined oestrogen/progesterone products. The intrauterine contraceptive device (IUCD) is rarely used at primary health care clinics and is rarely considered for emergency contraception. Contraceptives, including emergency contraceptive pills, can be obtained free at public health facilities. Little is known or documented about knowledge and use patterns of EC in South Africa. In one of the few studies that asked pregnant student nurses about their knowledge of EC, many (73%) had no knowledge of the method, despite being well educated and involved in health care training.8 As a prelude to the development and implementation of an intervention aimed at promoting EC, we undertook a multi-part baseline study to determine the existing knowledge and use of EC amongst women aged 15-49 years attending public health facilities in three provinces of South Africa. Findings on EC knowledge and practice for all respondents show that only 22.8% of respondents had ever heard of EC, with the younger more educated women and women living in urban areas more likely to have heard of it.9 Given the high teenage pregnancy rate and the vulnerability of young South African women to the acquisition of STIs and HIV, we regard young women as important potential users of EC. This paper focuses specifically on the prevalence of unintended pregnancy and the knowledge and use of EC among the younger women (1524 years) attending health facilities in the most rural and urban study areas. Methods Ethics The ethics committees of the Universities of Durban-Westville, the Witwatersrand and Cape Town approved the study. Permission to conduct the study at public health facilities was obtained from the relevant health authorities. Study Sites and Participants The study was conducted at 14 public health facilities in a rural area of the province of KwaZulu-Natal and 17 clinics in an urban area of Gauteng. All participating facilities offered family planning and primary health care services. Interviews were conducted between April and August 2000. For each health facility a minimum of ten women aged 15-49 years were interviewed. No incentive was offered to participate. This paper reports only on the subset of young women aged 15-24 years. Data Collection/Procedures Pre-tested structured questionnaires were used for individual interviews. Women were inter-viewed either before or after their consultation, but after they had been fully briefed about the study. They were asked personal details including home language, age, marital status, highest level of schooling and occupation. A sexual history was taken, which included sexual activity, pregnancies, age at first pregnancy, number of children, and knowledge and use of contraceptive methods. Thereafter they were specifically questioned about knowledge of emergency contraception. Those who knew of EC were asked whether they had ever used it, their reason for use and where it was obtained. Data Analysis Data were entered into a Microsoft Access 2000 database and analysed using SAS version 6.12. Descriptive statistics for key variables are presented. The association of variables was determined by means of the ordinary chi-square test. A p value < 0.05 was considered to be statistically significant.
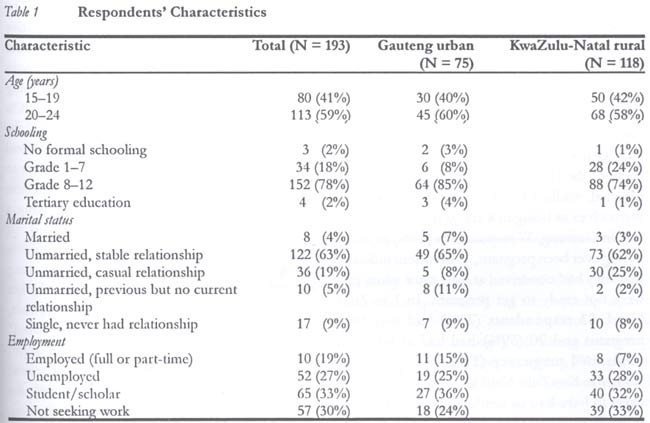
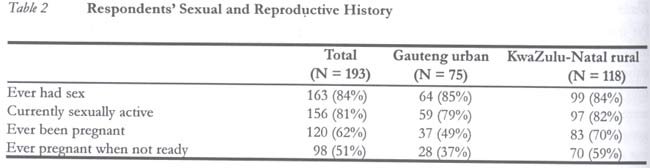
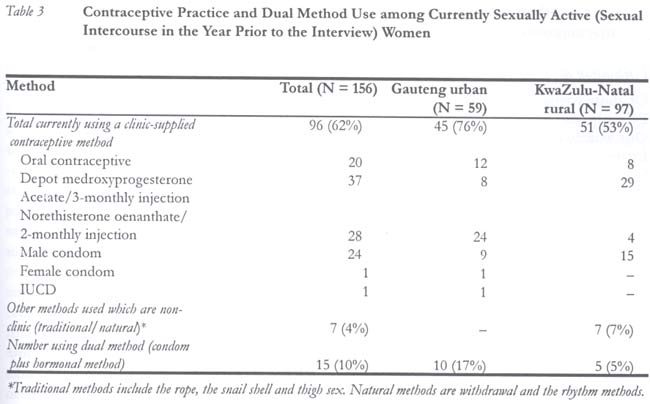
Results Demographic Characteristics of Respondents A total of 378 women were interviewed, with a response rate of over 90%. The sub-sample of 15-24-year-olds comprised 193 women (75 in Gauteng; 118 in KwaZulu-Natal). All data presented in this paper concern these young women. The demographic characteristics of respondents are summarised in Table 1. The home language of respondents in Gauteng varied, with Zulu (36%) and Sesotho (23%) being the most commonly spoken language. In KwaZulu-Natal all interviewees were Zulu speaking. The majority of young women, 85% in Gauteng and 74% in Kwazulu-Natal, had at least reached grade 8 (i.e., entered secondary level of education). Almost a third in both provinces (36% in Gauteng and 32% in KwaZulu-Natal) were still scholars, and 25% in Gauteng and 28% in KwaZulu-Natal were unemployed but seeking employment. Reason for Clinic Visit The young women interviewed had attended the clinics for varying reasons. In Gauteng, 52% presented for family planning services, compared to only 15% in KwaZulu-Natal where 35% were attending the "Well Baby Clinic" and 33% for primary health curative services. Sexual and Reproductive History of Clients Most of the young women had had sexual intercourse at some time (85% in Gauteng and 84% in KwaZulu-Natal), with a slightly lower percentage (79% in Gauteng and 82% in KwaZulu-Natal) reporting having had sexual intercourse in the previous year. This latter group was regarded as being currently sexually active. Eight of the 156 (5%) sexually active women were married, while 117 of them (75%) classified themselves as being in a stable relationship. In Gauteng, 37 respondents (49%) reported having ever been pregnant, 28 of whom indicated that they had conceived at least once when they were not ready to get pregnant. In KwaZulu-Natal, 83 respondents (70%) had ever been pregnant and 70 (59%) had had at least one unplanned pregnancy (Table 2). The young women in KwaZulu-Natal were significantly more likely to have had an unplanned pregnancy than those from Gauteng (p = 0.001). Of the 120 young women who had ever been pregnant, 79% had conceived before reaching the age of 20 (73% in Gauteng and 82% in KwaZulu-Natal). Overall, 95 out of 193 (49%) women had had teenage pregnancies. Of all 20-24-year-olds, 66 (58%) had been pregnant before the age of 20. Contraception and Barrier Method Use Contraceptive utilisation patterns are shown in Table 3. Significantly more sexually active respondents in Gauteng (76%) were currently using a modern method of contraception than those in KwaZulu-Natal (53%) (p = 0.003). The most commonly used modern contraceptive method was the progestogen injectable contraceptive (71% in Gauteng and 65% in KwaZulu-Natal). Only one woman was using IUCD. Barrier methods were found to be 26% of clinic-based contraceptive use, and 15 of the 25 barrier method users were also using hormonal contraception (dual method use), with more in the urban area (17% versus 5%). No respondent in the urban area was found to be using a traditional or a non-clinic method of contraception. In the rural area, five women were using traditional methods and two were using natural methods (withdrawal and the rhythm method). Traditional methods included thigh sex, what is referred to as the "rope" or "wool" method and the "snail shell" method. The "rope" or "wool" method involves tying a cord around the waist to which herbs are attached, with the belief that this will protect against conception. The latter involves hiding a used sanitary towel in a snail shell in a secret place and only retrieving it when the woman is ready to conceive. Knowledge of Emergency Contraception Of the young women interviewed, only 25% (n = 19) in Gauteng and 11% (n = 13) in rural KwaZulu-Natal had ever heard of EC. It was more than twice as likely that a young woman in Gauteng would have heard of EC (RR = 2.3, Chi square p < 0.005). Of those young women who had heard of EC, more in Gauteng (42%) knew the correct timing of taking emergency contraceptive pills, that is, within 72 hours of unprotected sexual intercourse, compared with far fewer (17%) in KwaZulu-Natal. The others either did not know or were unsure of themaximum length of time allowed for EC efficacy after unprotected sexual intercourse. Utilisation of Emergency Contraception Of those young women who had ever heard of EC, only one from each region had ever used it. One woman gave a burst condom as her reason for using EC, while the other said she had missed her menses. Both these women had completed their secondary education and one was a university student. In both cases, EC had been purchased on request from pharmacies rather than obtained free from public sector clinics. The source of EC knowledge was a friend in one case and a family member in the other. Both women reported that they would like to keep a pack of emergency contraceptive pills at home in case they have need of it again. Missed Opportunities for Use of EC When the young women were asked whether they had had unprotected sex in the year prior to the interview, 39% indicated that they had (24% in Gauteng and 49% in KwaZulu-Natal). Rural women were significantly more likely to have had unprotected sexual intercourse in the previous year (p = 0.001). Only one woman indicated that she had considered using EC after engaging in unprotected sex. The majority did not consider using EC because of a lack of knowledge of this method. Discussion Findings suggest that there is a high risk of unplanned pregnancies amongst young single women especially in the rural areas. Reasons for the differences between urban and rural areas are unclear, as education and employment status in the two areas were similar. Despite the high prevalence of contraceptive use among young sexually active women, pregnancy rates remained relatively high. A recent study in a rural area of South Africa, when looking at age-specific fertility rates, showed an atypical bi-modal pattern, premarital fertility (among women aged 12-26 years) and marital fertility (among women aged 15-49 years). Pre-marital fertility accounted for 47% of births among women aged 12-26 years.10 The authors believe this high rate of pre-marital fertility reflects a low incidence of contraceptive use before the first birth especially among adolescents. Many women usually start using contraceptives only after the first birth.10 This is similar to our observation in rural KwaZulu-Natal. It should be noted, however, that pregnancy and contraceptive prevalence may be overestimated in our sample, as many of these young women were seeking family planning or well baby services at these clinics. The most popular method of contraception used in both provinces was the injectable. Use of IUCD, condom and dual protection against pregnancy and STIs was found to be low. Findings point to the need for access to a broader range of contraceptive options, and EC is an important method in this context. With escalating HIV rates, promotion of either dual or barrier method use with emergency contraception as a back-up in case of method failure or non-compliance is an ideal option for young women. Awareness and knowledge of emergency contraception amongst young women was very low, especially in rural KwaZulu-Natal, despite the fact that it was available at no cost at public health facilities. This lack of knowledge denies many young women, clearly in need of a contraceptive method that can be used after unprotected sexual intercourse, the opportunity to access and use EC. It is interesting to note that the two young women who used EC in this study purchased the pills from pharmacies on advice from family members or friends. In South Africa, up till November 2000, pharmacists were legally only able to supply the combined hormonal EC products (Ovral® and E-Gen-C®) on prescription from a doctor or if they had a special permit from the Department of Health. In November 2000, it became legal for pharmacists to supply hormonal contraceptives for EC without a doctor's prescription. This, together with the January 2001 launch of a dedicated levornogestrel-only product (Norlevo®), should improve accessibility to EC. However, there are few pharmacies in rural areas. The cost of the new product (60 South African Rands) may also be a barrier for many young women most in need. Intervention efforts to increase levels of awareness of young women, with increased promotion of EC could positively impact on usage. Sexuality programmes being developed should include information about all methods of pregnancy prevention including EC. Because the time frame for seeking EC is short, young women need to be aware that emergency contraception is an option, know where to seek services and understand that it must be taken within three days of unprotected sex. Providing emergency contraceptive information and, if possible, supplies at the time of a regular contraceptive visit is one way of ensuring that young women have the resources they need to protect themselves from pregnancy in the event of unprotected intercourse or a contraceptive accident.11 Efforts should be made to ensure that information about emergency contraception is communicated to young women through counselling, health promotion, life skills training programmes and display of posters and pamphlets. This means that efforts should also be made to reach those who do not regularly attend traditional clinic facilities.12 Schools can play an important role in the sexual education of young people, as they become sexually active before they are out of school. Interventions are being planned to look at promoting closer links between schools and health service providers. Interventions should also focus on making clinics youth-friendly so as to encourage attendance by young people. Since many of the young women in this study were scholars or students, targeting educational institutions for the promotion of dual protection against pregnancy and HIV is a viable option. Acknowledgements This study was funded by the Wellcome Trust (Grant Number 050522/Z/97/Z) through the Africa Centre for Population Studies and Reproductive Health. We thank the fieldworkers, health care providers, managers, clients and data punchers who assisted us in the project. References
©Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04035t4.jpg] [rh04035t3.jpg] [rh04035t2.jpg] [rh04035t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}