 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 8, No. 3, Dec, 2004 pp. 38-54 Evaluation of the ATBEF Youth Centre in Lome, Togo Ilene S Speizer1, Kodjovi Kouwonou2, Stephanie Mullen3 and Emilien Vignikin4 1Associate Clinical Professor in the Department of Preventive
Medicine and Community Health at Virginia Commonwealth University. 2Statistician/demographer
for African Population Advisory Council, Lomé, Togo. 3Evaluation
researcher with John Snow, Inc. 4Director of Unité de Recherche
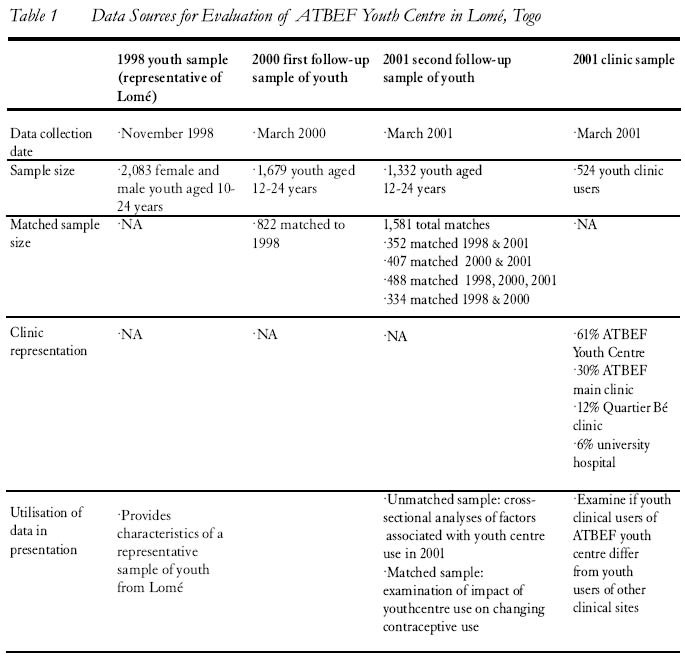
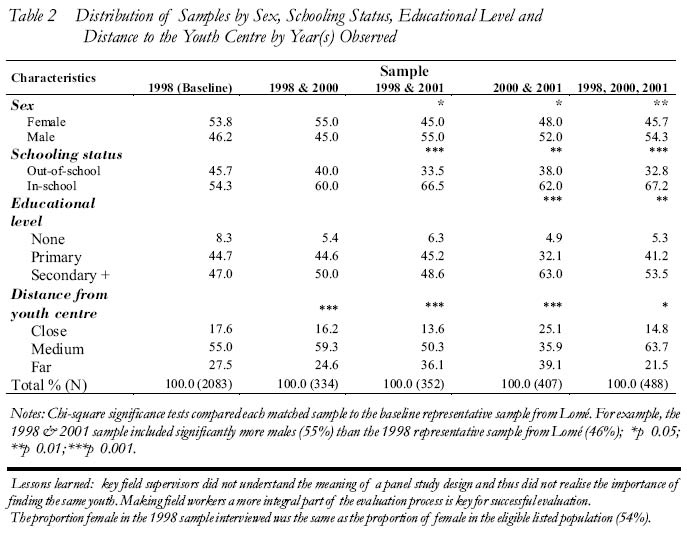
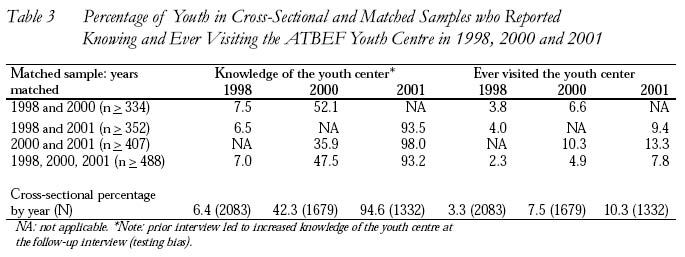
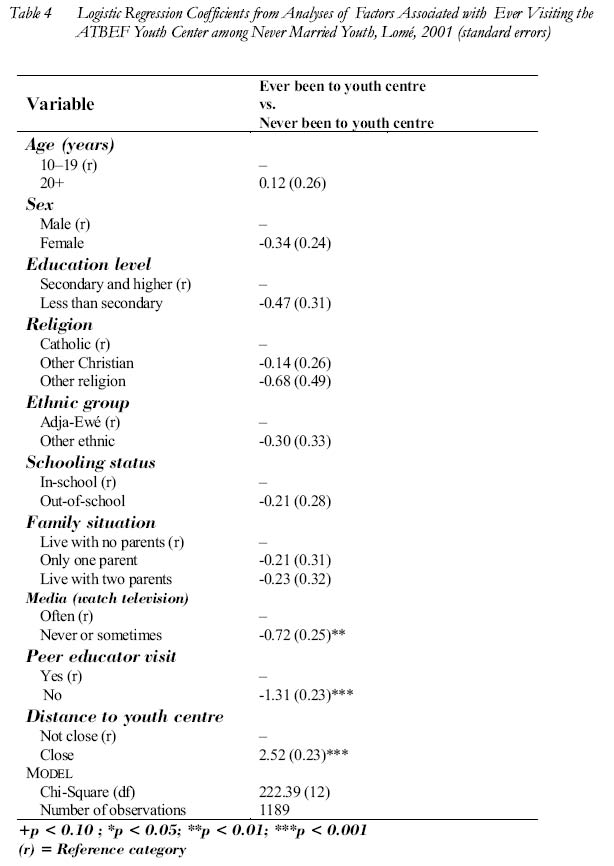
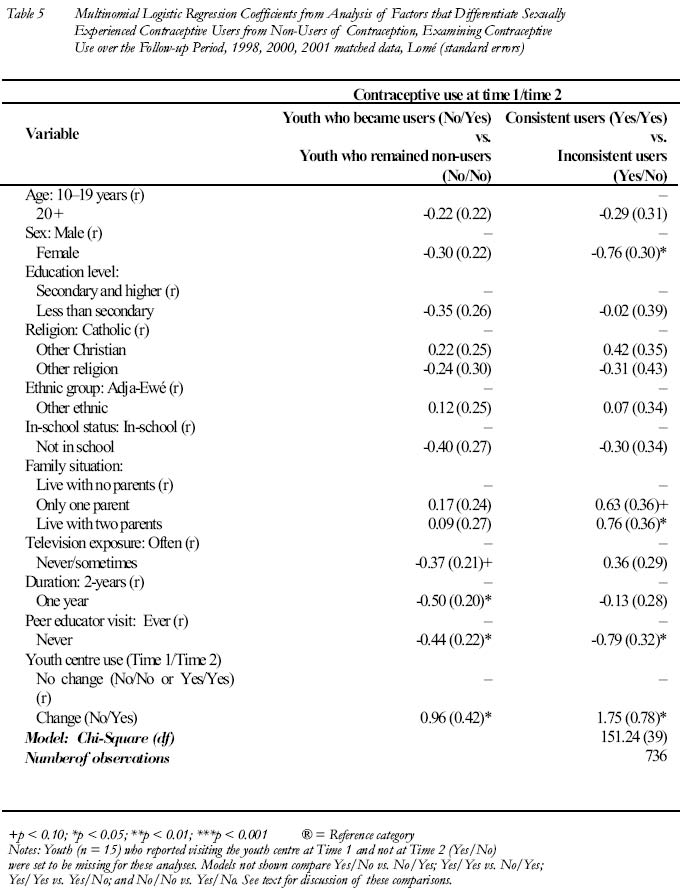
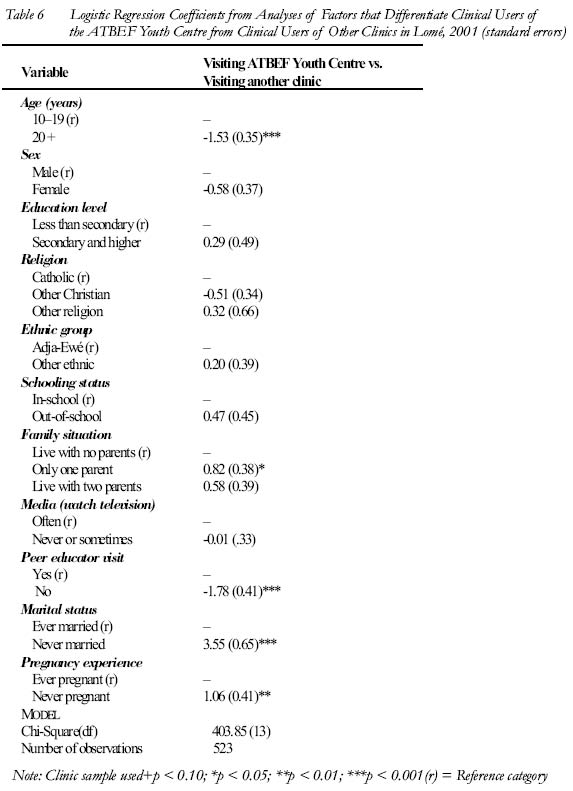
Demographique, Lomé, Togo. Code number: rh04041 ABSTRACT In 1998, the Association Togolaise Pour le Bien Etre Familiale launched a youth centre in Lomé, Togo. To evaluate the centre, a three-year panel study was undertaken. Three years after being launched, about 10% of surveyed youth had visited the centre. Youth who lived close to the centre had contact with a peer educator and were exposed to television were more likely to have visited the youth centre than all others. Visiting the youth centre and having contact with a peer educator were associated with greater contraceptive use in the matched sample. Youth centre clinical users were younger, less likely to be married and less likely to have ever been pregnant than clinical users of other sites. The youth centre is meeting its goal of providing services to high-risk youth in Lomé. To increase youth centre access for all youth, it will be necessary to increase the number of youth centres. (Afr J Reprod Health 2004; 8[3]:38-54 ) RÉSUMÉ Evaluation du Centre de la jeunesse ATBEF à Lomé, Togo. En 1998, l’Association togolaise pour le bien-être familial a lancé un centre de la jeunesse à Lomé, Togo. Pour évaluer ce centre, nous avons entrepris une étude de groupe qui a duré trois ans. Trois ans après le lancement, environ 10% des jeunes enquêtés avaient visité le centre. Les jeunes qui habitaient près du centre ont eu contact avec un éducateur de pair et ont été exposés à la télévision. Ils avaient la plus grande possibilité de l’avoir visité que tous les autres. La visite au centre et l’accès au parrain l’éducateur de pair étaient liés à une plus grande utilisation du contraceptif dans l’échantillon apparié. Les usagers de la clinique du centre étaient plus jeunes, avaient moins la possibilité d’être mariés où d’être jamais enceintes que les usagers des cliniques des autres centres. Le centre atteint ses buts d’assurer les services aux jeunes à haut risque à Lomé. S’il faut augmenter l’accès aux centres de la jeunesse, il va falloir augmenter le nombre de centres de la jeunesse. (Rev Afr Santé Reprod 2004; 8[3]:38-54 ) Key Words: Adolescent, youth, evaluation, contraception Introduction Throughout the world, the population of youth aged 10-24 years is estimated at about 1.7 billion.1 Eighty six per cent of youth worldwide live in the developing world.1 The proportion of youth varies modestly among regions, from a high of 33% in Africa to 28% in Asia. The most rapid future growth in absolute numbers of youth is expected to occur in Africa and the slowest in Asia and Latin America, the two regions that have experienced the earliest and most rapid declines in fertility in recent decades.2 Social and cultural changes that resulted from rapid urbanisation and modernisation have changed the dynamics of youth sexual behaviour. For example, as women and men spend longer time in school, the time between the onset of puberty and marriage is becoming longer, resulting in a higher likelihood that young people will engage in premarital sexual activity that may or may not be socially sanctioned.3 Youth who become sexually active at an early age are at risk of an unintended pregnancy and sexually transmitted infections (STI) including HIV. The risk of these outcomes is higher for youth than adults because young people often fail to use contraception consistently and effectively.4 Furthermore, youth change sexual partners often, resulting in increased risk of exposure to STIs and HIV. To prevent these negative outcomes among youth, a number of reproductive health (RH) programmes have been developed. Reproductive health programmes for youth generally have one or more of the following three goals: (1) to provide a supportive environment for youth; (2) to improve youth knowledge, attitudes, skills and practices; (3) and to increase service use among youth. Most of the evidence to date on effective programmes for youth in developing country settings focuses on the second of these goals, i.e., programmes that improve knowledge, attitudes, skill and practices.5 Less is known about programmes that attempt to improve the environment and increase service use among youth. Increasing service use among youth implies addressing the main barriers to youth accessing health services. These barriers include long distances to service locations and unsafe or unavailable transportation; inconvenient hours of operation; concerns about privacy and confidentiality; staff members’ attitudes and actions including scolding and moralising; fear and embarrassment; cost of services; and laws and policies that make serving youth difficult.6-9 The main strategies used to achieve increased youth service use include improving the quality of adult clinics for youth (youth-friendly services), providing clinical services in a school setting, and attracting youth to youth centres. Although a large number of service-based programmes have been implemented over the past ten years, only a small number of these programmes have been rigorously evaluated.5 This means that there is limited evidence on the effectiveness of strategies to increase adolescent access to clinical and counselling services. This study begins to fill this gap by presenting the results of a three-year evaluation study of a youth centre in Lomé, Togo. Improving Youth Access to Services Youth centres are an appealing strategy for improving youth service use because they tend to provide a supportive, non-threatening environment where youth have access to counselling, contraceptives, clinical prevention services, treatment and referral. These services are delivered alongside recreational, educational and vocational activities that draw youth to the centre on a regular basis. Youth centres often have peer educators who undertake outreach educational and referral activities in the community. The few extensive studies of youth centres undertaken recently were situation analyses undertaken by the Population Council in Ghana, Kenya and Zimbabwe.10-12 These studies generally found that most youth centre use is for recreational purposes rather than for clinical services. Furthermore, when clinical services were used, the clients were often older than the target age.10 The Kenyan study included cost measures and found that it cost about $0.31 per youth for each educational session, while it cost $102.00 for each client reached with family planning or other reproductive health clinical services.11 If use of clinical services remains low, youth centres will be cost-prohibitive especially in the long term. While situation analyses inform our perspectives on youth centre use, they fail to capture the perspectives of non-users of the facility. In the Kenya study, a community-based survey demonstrated low knowledge of the youth centre even among youth who lived rather close to the centre.11 Furthermore, an evaluation study of MEXFAM’s (the IPPF affiliate in Mexico) three youth centres in low-income areas of Mexico City showed that those youth who most needed reproductive health information and services were not those who most used the youth centres. To reach large numbers of young people, MEXFAM would have to open many more youth centres, something that would be expensive and not sustainable.13 Although youth centres are expensive and possibly not sustainable in the long term, they continue to be used for provision of RH clinical and counselling services for youth in Africa, Asia and parts of Latin America. Until these programmes are fully evaluated, their impact on adolescent reproductive health outcomes remains unknown. This study fills a gap in our knowledge of the effectiveness of youth centres by studying a youth centre in Lomé, Togo. The focus of this study is on evaluating youth centre impacts on contraceptive use and determining the appropriateness of a youth centre as a service delivery model. No cost data are included in this study, the emphasis is therefore only on programme impact. Intervention: ATBEF Youth Centre In 1989, the Association Togolaise pour le Bien-Etre Familiale (ATBEF), the International Planned Parenthood Federation affiliate in Togo, opened a youth centre in the coastal town of Notsé. Nine years later (1998), ATBEF launched two new youth centres in Lomé (the capital city) and Sokodé (a major city in central Togo). Each of these youth centres has the overall objective of contributing to the physical, psychological and social development of youth by creating a positive environment for reproductive health education and providing accessible reproductive health information and services to youth. Prior to the creation of the Lomé youth centre, influential youth who were leaders of youth groups and school groups were asked to participate in meetings with ATBEF coordinators to help inform the youth centre planning process and ensure that youth needs were clarified and addressed. The Lomé youth centre was officially launched in March 1998 but the majority of the activities were not fully functional until July 1998. The Lomé youth centre is organised in four departments, namely, clinic, library, education (reproductive health education, sewing, cooking and reading), and recreation. The clinic personnel are specially trained in reproductive health service delivery for youth. The clinic mainly serves patients who need pregnancy tests, tests for STI, reproductive health counselling, provision of family planning and general health care (physicals, malaria, illness diagnosis). The clinic has a small laboratory that does all testing, with the exception of HIV tests that are sent to the ATBEF main clinic. The majority of the youth centre use is for recreational and educational purposes. These youth come to the centre to watch educational programmes on television, play games, attend a drama, and/or participate in discussion groups. The Lomé youth centre also undertakes a number of activities throughout the city to improve the reproductive health of all youth. This includes using trained peer educators who undertake outreach and referral activities in the community. Also, ATBEF uses radio and television for advertising the youth centre and presenting organised discussions on youth reproductive health related topics. Finally, the youth centre undertakes activities with schools, which include bringing school groups to the centre and having youth centre staff visit schools to make presentations and lead group discussions. Each of these activities increases the reach of the youth centre that is based in the centre of Lomé, a large capital city. Methods Evaluation Design Evaluation of the Lomé youth centre was undertaken by the Unité de Recherche Demographique and the USAID funded FOCUS on Young Adult Project (Tulane University Department of International Health and Development). The overall aim of the evaluation was to determine whether the youth centre had an impact on youth reproductive health behaviours in Lomé. The objectives of the evaluation were: (1) to determine the characteristics of youth centre users; (2) to examine changes in knowledge, attitudes and behaviours of youth in Lomé over the follow-up period and determine if changes are associated with youth centre use; and (3) assess whether clinic users of the youth centre are different from youth users of other clinical sites in Lomé. The evaluation of the Lomé youth centre used a panel study design, that is, the same youth were interviewed at multiple time points. No comparison community was included, given that Lomé is the capital city and there are no comparable cities within Togo. Data were collected from a random sample of youth from Lomé (Table 1) at baseline (1998) and at follow-up I (2000) and follow-up II (2001). Using the demographic and health survey (DHS) sampling frame from the 1998 DHS survey in Togo, the 62 DHS enumeration areas (EA) from Lomé were categorised as being close to the youth centre, being medium distance to the youth centre, and being far from the youth centre. This provides a control for better access to the youth centre by persons who live closer. To divide the sample by location relative to the youth centre, the enumeration areas were mapped relative to the city. All enumeration areas within the main circular boulevard were considered close to the youth centre. Enumeration areas on the outskirts of the boulevard were considered medium distance, and the enumeration areas on the edges of the city were considered far from the youth centre. Three time points were used to (1) provide a longer term perspective on the youth centre’s impacts; and (2) increase the sample size of participants interviewed at a minimum of two time points. At the second follow-up (2001), we also collected information from a sample of clinic users. Four clinical sites were used to provide information on whether youth users of the youth centre clinical services were different from youth users of other popular clinical sites. This information is crucial to determine whether the youth centre is meeting its mandate of providing clinical services to youth in Lomé. If users of the youth centre resemble users of other clinics then the youth centre may be simply drawing on youth who would have received RH clinical services elsewhere if the youth centre were unavailable. Study Populations At baseline, using the 62 enumeration areas from Lomé in the 1998 Togo DHS, all households were revisited to list all youth (10-24 years) who were eligible for interview (November 1998). A random sample of 2,083 youth (10-24 years) and 1,027 adults (aged 30 years and older) were interviewed (details of the parent sample presented elsewhere14). This represented 93% of the youth population that was eligible for interview. No significant differences were found between those youth who were eligible and those who were actually interviewed by age or gender.15 In March 2000, 16 months after the baseline survey, the first follow-up survey was undertaken (Table 1). Due to logistic problems we did not find a large proportion of the baseline sample and youth not found on the first try were replaced by other youth. A total of 1,679 youth were interviewed in the first follow-up sample. This sample included 822 youth interviewed in the first round of data collection (39% of the baseline sample) and 857 new youth. To obtain a larger sample of youth with two time points of data, we undertook a third round of data collection in March 2001, one year after the first follow-up (Table 1). For this sample, we only interviewed youth who participated in the first or second round of data collection. Interviewers were instructed to request address changes to ensure finding the appropriate individuals for interview. A total of 1,332 youth were interviewed in 2001; 94% of youth from 2001 were matched with 1998 and/or 2000. The total sample was 1,581 youth for whom we had at least two observations (1998 and 2000, n> 334; 1998 and 2001, n > 352; 2000 and 2001, n > 407; 1998, 2000 and 2001, n > 488). Column 1 of Table 2 presents the characteristics of the baseline (1998) representative sample by gender, schooling status, educational level and distance from the youth centre. The table also presents demographic characteristics for the matched samples. Column 2 provides the characteristics of youth interviewed only in 1998 and 2000, column 3 provides information on youth interviewed only in 1998 and 2001, column 4 provides information for youth interviewed only in 2000 and 2001, and column 5 provides information for youth interviewed at all three time points (1998, 2000 and 2001). The table shows that the 1998 representative sample from Lomé was about 54% female. In the matched samples, the proportion of female was significantly less (except 1998 & 2000 samples), indicating that fewer female youth were found and interviewed in 2001. The distribution by in-school status indicates that the matched samples included a significantly greater proportion of in-school youth than the representative baseline sample. Similarly, two of the matched samples (2000 & 2001; and 1998 & 2000 & 2001) were significantly more educated than the baseline sample. Finally, the distributions by distance to the youth centre indicate that the matched samples were significantly different from the baseline sample. Therefore, it is important to note that our matched samples included a larger proportion of male youth, in-school youth and more educated youth than expected from a random sample of youth in Lomé. These youth are probably less mobile and easier to find at follow-up compared to their less educated out-of-school peers. In March 2001 (second follow-up period), we also collected data from a sample of youth clinic users (Table 1). Youth (aged 10-24 years) were recruited from four main clinic sites upon completion of a clinical visit. The clinics were the ATBEF Youth Centre clinic; the ATBEF central clinic; the university health centre; and a health centre in a young transient neighbourhood (Quartier Bé). These clinics were selected because they are expected to draw the largest youth client populations in Lomé. Data collection in the four health centres took place over a two-week period. A supervisor and an interviewer were assigned to each clinic and instructed to interview all youth aged 10-24 years who came for medical consultation. In the ATBEF Youth Centre clinic it was necessary to have more than one interviewer present, given that there were more youth clients at this facility than the others. A total of 524 youth were interviewed in the four clinics. This represents 61.2% from the ATBEF Youth Centre, 20.8% from the ATBEF central clinic, 12.4% from the health centre in Quartier Bé, and 5.5% from the university health centre. In the sample from the ATBEF Youth Centre clinic, 59% were female, 68% were under 20, and 99% were never married. The comparable percentages from all other clinic samples combined were 91%, 14% and 32% respectively. Multivariate models were used to examine whether these differences were significant controlling for all factors simultaneously. Analyses Methods Determinants of youth centre use The first multivariate regression analysis examines factors that distinguish users from non-users of the ATBEF Youth Centre using the entire never married cross-sectional 2001 youth sample. Specifically, the dependent variable for this analysis is coded one (1) for youth who reported ever visiting the ATBEF Youth Centre and zero (0) otherwise. The independent variables in this analysis were age (10-19 years versus 20-24 years), gender, education (none or primary versus secondary or higher), religion (Catholic, other Christian, other religion), ethnicity (Adja-Ewé versus other ethnicity), schooling status (in-school versus out-of-school), peer educator contact (no versus yes), family environment (lived with both parents, lived with neither parent, lived with one parent), television exposure (never or sometimes watched versus often watched), and distance to the ATBEF Youth Centre (close versus not close). Given that single youth have less access to RH services, we focused on the never married sample of youth, which was 89.5% of the 2001 sample (82.2% of females and 95.8% of males). A logistic regression model was run on the entire never married sample, including all variables in the model simultaneously. Only the 2001 sample was used for this model because use of the youth centre was too low in the earlier years (3.3% in 1998 and 7.5% in 2000). Impact of youth centre use on contraceptive use The second multivariate regression analysis examined whether adolescent use of the youth centre over the follow-up period was associated with reported use of modern contraception. For this analysis we used the panel sample of youth who were sexually experienced at observation 1. In this case, observation 1 was either 1998 or 2000 and observation 2 was either 2000 or 2001. For youth who were interviewed at all three time periods, we examined their reported behaviours in 1998 and 2001. The dependent variable had four categories: did not use contraception at observation 1 and observation 2 (No/No 47%); used contraception at observation 1 and did not use at observation 2 (Yes/No 15%); did not use contraception at observation 1 and used at observation 2 (No/Yes 22%); and used contraception at observation 1 and observation 2 (Yes/Yes 16%). Reported contraceptive use was based on use of a modern method at last sex among sexually experienced youth. The overwhelming majority of this modern use (92%) was condom use. The main independent variable of interest in this model was use of the youth centre over the follow-up period. This variable was coded one if the youth reported first visit to the youth centre between observation 1 and observation 2 (6%) and was coded zero if the youth never visited the youth centre or reported visiting the youth centre at observations 1 and 2 (90% never visited and 4% visited at both observations). The small number of youth (n > 12) who reported ever visiting the youth centre at observation 1 but not at observation 2 were coded as missing for this analysis. Also included in this model was whether the youth had ever had contact with a peer educator (coded 1 if never had contact and zero if ever had contact), and duration between observations (2 years versus 1 year). The remaining independent variables included age, gender, level of education, religion, ethnicity, in-school status, family situation and media exposure. All of these independent variables were coded as above in the use of the youth centre analysis and measured at observation 1. Multinomial logistic regression analyses were performed, entering all variables simultaneously. The main contraceptive use comparisons presented were (a) No/Yes versus No/No (never used); and (b) Yes/Yes versus Yes/No. These comparisons provided a perspective of differences between those youth who became users over the follow-up period and those who were never users and between consistent users and users who discontinued use. The remaining comparisons, while interesting, provided similar results as those presented. Use of the ATBEF clinic versus other clinics The final multivariate analysis used the 2001 clinical sample to examine factors that differentiate ATBEF Youth Centre clinic users (61% of users) from youth users of the other clinical sites. The dependent variable was coded one for youth interviewed in the ATBEF Youth Centre and zero for youth interviewed in all other clinical sites. In this sample, 71% (n > 371) of the youth interviewed were female. Independent variables in this analysis included age, gender, education, religion, ethnicity, in-school status, ever-had peer educator contact, television exposure, and family environment, all coded as explained. Additional independent variables in this analysis included marital status (single versus married) and pregnancy experience (yes versus no). Logistic regression models were run on the entire clinic sample, including all variables in the model simultaneously. Results Knowledge and Use of Youth Centre Table 3 presents the knowledge and use of ATBEF Youth Centre by the cross-sectional and matched sample. At baseline, only a small percentage of youth knew about the ATBEF Youth Centre, which had opened officially about seven months prior to interview, but began full operation about four months earlier. The proportion that had knowledge of the youth centre increased considerably over the follow-up period, partly due to greater exposure to peer educators and media messages promoting the facility and partly due to informants learning about the youth centre at prior interview. A realistic view of improved knowledge is seen when comparing the 1998 value at baseline (6.4%) to the proportion of the 2000 and 2001 panel sample with knowledge in 2000 (35.9%). Use of the ATBEF youth centre rose over the follow-up period as well. At baseline, 3.3% of the sample reported ever visiting the youth centre (for recreation or clinical services). By 2001, 10.3% of the cross-sectional sample reported having ever visited the youth centre. Increases in youth centre use rose by about an absolute value of 3% between the baseline and first follow-up and the first follow-up and the second follow-up. This suggests that use of the youth centre is rising over time, although slowly. Determinants of Youth Centre Use Table 4 presents the logistic regression co-efficient from the analysis of factors that differentiate users and non-users of the ATBEF Youth Centre in the 2001 cross-sectional sample of never married youth. In this case, use can be for recreation, clinical services, or counselling services. The results in Table 4 demonstrate that youth who were ever exposed to a peer educator were significantly more likely to have ever visited the youth centre than youth who never had contact with a peer educator. Further, media exposure was positively associated with youth centre use. This is not unexpected, given that ATBEF advertised the youth centre on the local television station and also presents popular round table discussions on reproductive health topics relevant to youth. Finally, proximity to the youth centre matters. Youth who lived closer to the youth centre were significantly more likely to have ever visited the youth centre than youth who lived further away. To better understand the impact of distance from the youth centre, we performed simulations of youth centre use under varying distance scenarios, holding all other variables constant. If all youth interviewed lived close to the youth centre, we would expect that about 33% of youth would have ever visited the centre (compared to about 10% in the sample from throughout Lomé). Conversely, if the entire sample did not live close to the youth centre (i.e., lived medium and far distance), only 5% of youth would have ever visited. Finally, proximity to the youth centre matters. Youth who lived closer to the youth centre were significantly more likely to have ever visited the youth centre than youth who lived further away. To better understand the impact of distance from the youth centre, we performed simulations of youth centre use under varying distance scenarios, holding all other variables constant. If all youth interviewed lived close to the youth centre, we would expect that about 33% of youth would have ever visited the centre (compared to about 10% in the sample from throughout Lomé). Conversely, if the entire sample did not live close to the youth centre (i.e., lived medium and far distance), only 5% of youth would have ever visited. Impact of Youth Centre Use on Contraceptive Use Table 5 presents factors associated with contraceptive use in the matched panel sample of sexually experienced youth. Among non-users of contraception at observation 1, column 1 shows the factors that differentiate youth who become users over the follow-up period (No/Yes) from youth who remain non-users (No/No). Youth who visited the youth centre over the follow-up period were significantly more likely to be users at observation 2 than youth who had never visited the youth centre or youth who had visited the youth centre already by observation 1. Other factors associated with contraceptive use at observation 2 include peer educator contact and media exposure, both in the expected directions. Finally, a longer duration between interviews (two years compared to one year) was associated with becoming a user. This duration variable captures the impact of increased access to information and services over a longer time period. Column 2 of Table 5 presents the factors that differentiate consistent users of contraception to users who discontinue use over the follow-up period (or are inconsistent users). Youth who visited the youth centre over the follow-up period were significantly more likely to be users at both time periods than youth who either never visited the youth centre or youth who had already visited the youth centre at observation 1. This suggests that for contraceptive users, visiting the youth centre affirms contraceptive use behaviours. Column 2 also demonstrates that female youth were less likely to be consistent users, a consequence of young women desiring children earlier than young men or a consequence of condoms being the main method used and lack of control over condom use among young women. Youth who lived with their parents (one or two) were significantly more likely to remain users. Youth who lived on their own or with a partner were probably more likely to want to get pregnant than youth who lived with a parent. Finally, exposure to a peer educator is associated with consistent use. Use of the ATBEF Clinic versus Other Clinics The final analysis (Table 6) examined whether clinical users of the youth centre were different from users of the other clinical facilities. First, clinic users of the youth centre were significantly younger and significantly less likely to be married than clinic users of the other facilities. These are two important target groups for the ATBEF Youth Centre clinic. Further, never pregnant youth were more likely than ever pregnant youth to be visiting the youth centre. Conversely, ever pregnant youth were significantly more likely to use (or have access to) other facilities than The youth centre. Finally, peer educator contact was associated with youth centre clinic use, an indication of the importance of outreach by the ATBEF Youth Centre. Discussion and Conclusions What do these findings say about the effectiveness of a youth centre for providing reproductive health services to youth? First, it appears that peer educator outreach and youth centre activities on the television are important strategies for increasing youth centre use. However, these strategies do not result in high levels of use, given that after three years of being open, only 10% of youth surveyed had ever visited the youth centre. This may be a consequence of youth having access to reproductive health information and services and recreational activities in other locations including schools and community settings. Further, given that the main contraceptive method used among youth in Lomé is condoms, there is not a high demand for clinical primary prevention services. Additionally, we found that use of the youth centre appeared limited to those youth who lived close to the facility. To increase access throughout Lomé, it would be necessary to create more youth centres, an expensive proposition especially given that most youth centre use is for recreational rather than clinical service.15 Notably, youth centre records make the youth centre appear well-used. Unfortunately, from the information available at the youth centre, it was not possible to determine if youth visiting the youth centre were: (1) within the target age; and (2) repeat users who like to visit the centre for social activities. Youth centre use was significantly associated with contraceptive adoption and consistent contraceptive use over the follow-up period. Peer educator contact also appeared important for promoting visits to the youth centre as well as encouraging contraceptive use. Peer educators in Lomé provide information about contraceptives and often refer youth to the ATBEF Youth Centre, even if the peer educators officially work for another family planning or HIV/STD prevention organisation. Clinical users of the youth centre who were between 10 and 24 years old were significantly different from similarly aged clinical users of other facilities. Youth centre clinic users were younger, less likely to be married, and were more likely to have no prior pregnancy experience. These were important target groups for youth centre reproductive health services, as these groups often lack access to reproductive health services in many settings. Conversely, the married youth, older youth, and youth who have ever been pregnant had more options for reproductive health services, and while they may visit the youth centre, they were more likely to be in the other clinical sites than their less experienced peers. There are two main limitations of this analysis. First and foremost, there was no control community used to determine, for example, if changes in contraceptive use and youth centre use over the follow-up period were associated with other activities underway in Lomé. Given that the youth centre was launched in the capital city, there was no obvious control site in Togo. We did, however, examine differences by proximity to the clinic to help provide some context to the presentation. Second, some problems were encountered obtaining the follow-up data desired. This meant that the follow-up samples are somewhat biased compared to the baseline representative sample from Lomé. The follow-up samples are more likely to be male, in-school and more educated, all factors possibly associated with the outcomes of interest (use of the youth centre and contraceptive use). Note, however, that while this bias affects the discussion of overall youth centre use and contraceptive use in Lomé (i.e., it is not representative), it has less effect on the relationship between the key factors examined. Therefore, we expect that even in a more representative sample that youth centre use would have a small and significant impact on contraceptive use. To conclude, youth centres are attractive because they provide comprehensive reproductive health services to youth in a youth-friendly environment. Youth centres often target the young, never married women and men, high-risk groups for unintended pregnancies and STI in sub-Saharan Africa. This study indicates that these target populations are more likely to visit the ATBEF Youth Centre clinic than the other clinics. Also, use of the youth centre (for any reason whether recreational or clinical) was found to be associated with contraceptive adoption and continuation. Therefore, we demonstrate that a youth centre can be an effective strategy for meeting youth reproductive health needs, specifically for youth who live close to the centre. In a time of increased need for STI testing and HIV voluntary counselling and testing, youth centres are an attractive, non-threatening service delivery strategy for youth. This study, however, did not examine cost data so we are unable to say whether the youth centre is a cost-effective strategy. Prior research suggests that youth centres are cost prohibitive. Future research is needed to determine how to make youth centres less costly (possibly by locating them in existing sites like a school to reduce building costs) and thus permit the strategy to be implemented in a cost-effective manner that can be replicated elsewhere. Acknowledgement The work for this article was done while the first and third authors were at Tulane University School of Public Health and Tropical Medicine, and the second author was at the Unité de Recherche Demographique. The research on which this article is based was supported by funds provided by the US Agency for International Development (USAID) to the FOCUS on Young Adults Project/Pathfinder International under cooperative agreement CCP-A-00-96-90002-00, and field support funds from the Family Health and AIDS in West and Central Africa project under agreement 624-0440-A-00-505-3-00 from USAID. The authors wish to thank Robert Magnani, Eric Seiber and B. Oleko Tambashe for their helpful comments on an earlier version. REFERENCES
©Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04041t4.jpg] [rh04041t5.jpg] [rh04041t2.jpg] [rh04041t1.jpg] [rh04041t6.jpg] [rh04041t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}