 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 8, No. 3, Dec, 2004 pp. 81-91 Characteristics of Abortion Care Seekers in South-Western Nigeria Boniface A Oye-Adeniran1,5, Isaac F Adewole2,5, Augustine V Umoh3, Oluwafunmilayo R Fapohunda4 and Ngozi Iwere5 1Department of Obstetrics & Gynaecology, College of Medicine,
University of Lagos, Lagos, Nigeria. 2Department of Obstetrics & Gynaecology,
College of Medicine, University of Ibadan, Ibadan, Nigeria. 3Department
of Obstetrics & Gynaecology, University of Uyo Teaching Hospital, Uyo,
Nigeria. 4Brooklyn Hospital Center, New York, NY 11201, USA. 5The
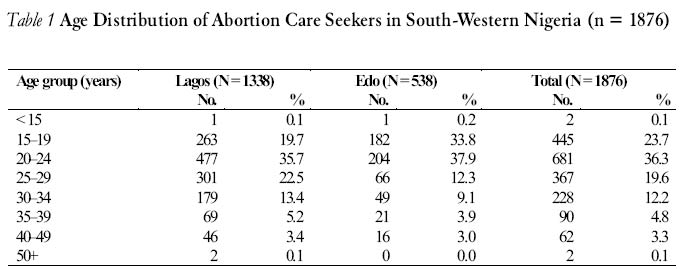
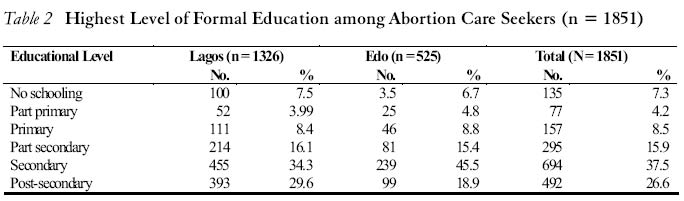
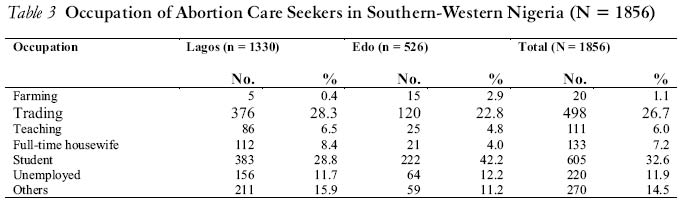
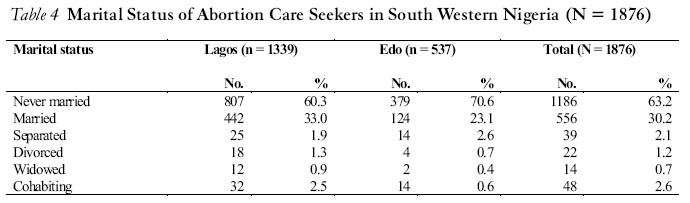
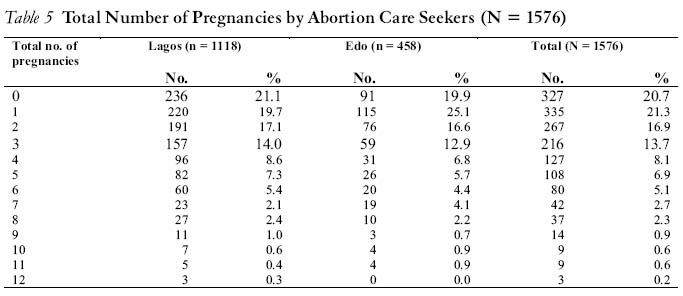
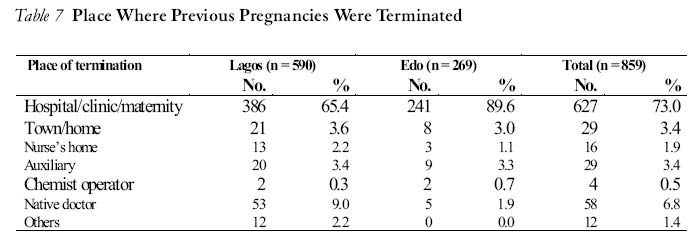
Campaign Against Unwanted Pregnancy (The CAUP) Code number: rh04044 ABSTRACT This prospective hospital-based study was carried out to understand the characteristics of abortion care seekers in south-western Nigeria. Information was obtained from a total of 1876 women seeking abortion at hospitals using a questionnaire. The results show that majority (60%) were between the ages of 15 and 24 years, of which adolescents between the ages of 15 and 19 years constituted 23.7%. Most (63.2%) of the respondents were unmarried, but married women also constituted a significant proportion (30.2%) of the abortion care seekers. Students were the single highest group, while the predominant economic activity was trading (26.7%). Respondents terminated their pregnancies mainly because they were students or because they did not desire to have children. Most (35.5%) of the women were introduced to providers by friends. Average contraceptive prevalence among the abortion care seekers was 27.4%. It is obvious from the results that young persons, especially in-school adolescents, should be targeted for comprehensive sexuality education especially in view of the current HIV/AIDS pandemic. (Afr J Reprod Health 2004; 8[3]: 81-91) RÉSUMÉ Caractéristiques des chercheuses des soins de l’avortement au sud-ouest du Nigéria.Cette étude prospective centrée sur l’hôpital a été menée pour comprendre les caractéristiques des chercheuses des soins post avortement au sud-ouest du Nigéria. Les renseignements ont été recueillis à l’aide d’un questionnaire de la part de 1876 femmes, à la recherche de l’avortement auprès des hôpitaux, les résultats montrent que la majorité (60%) avaient entre 15 et 24 ans dont les adolescentes ayant entre 1519 constituaient 32,7%. La majorité (63,2%) constituaient une proportion importante (30,2%) des chercheuses de l’avortement. Les étudiantes constituaient le seul groupe le plus nombreux, alors que l’activité économique la plus fréquemment avancées pour l’interruption de grossesse étaient le statut estudiantin et ne voulant pas avoir des enfants alors qu’elles n’étaient pas encore mariées. La plupart (35,5%) des femmes ont fait la connaissance des dispensateurs de soins grâce à leurs amis. La prévalence contraceptive moyenne chez les chercheuses des soins de l’avortement était de 27,4%. Il est évident, d’après ces résultats que les jeunes gens, surtout les adolescentes en scolarisation, devraient être les cibles de l’éducation sexuelle compréhensive surtout étant donné la pandémie actuelle qu’est le VIH/SIDA. (Rev Afr Santé Reprod 2004; 8[3]:81-91) Key Words: Abortion, abortion care seekers, unwanted pregnancy, contraceptive prevalence, young persons, Nigeria Introduction Induced abortion remains a major contributor to maternal morbidity and mortality in Nigeria, and indeed the developing world, which altogether contributes about 95% of unsafe abortions globally.1-4 In a study in Lagos,2 unsafe abortion accounted for 22.5% of maternal deaths over a ten-year period. Of these, 61% were single schoolgirls. An estimated 46 million abortions occur annually worldwide, in spite of reported increases in contraceptive awareness and usage.5 In Nigeria, an estimated 610,000 abortions occur annually despite the restrictive laws.6 The penalty for illegal abortion is fourteen years imprisonment for the provider and seven years for the seeker of induced abortion. Although abortion is permissible in Nigeria to save the live of the woman, the major cause of the procedure is unwanted pregnancy. It is believed that a vast majority of women are likely to have had at least one abortion by the time they are 45 years old.7 As a result of the restrictive nature of the abortion law in Nigeria, and the traditional societal perception of abortion, nobody would easily admit to abortion either as a provider or as a patient. Consequently, correct information on the characteristics of those who desire these services are often lacking or open to conjecture. This in turn hampers the establishment and implementation of effective and proper intervention strategies to combat the problem of unwanted pregnancy and unsafe abortion. This study, therefore, seeks to bridge this gap by studying the characteristics of abortion care seekers and their motivations. Methodology Prior to the field work, The Campaign Against Unwanted Pregnancy (The CAUP) obtained an endorsement for the study from the Nigerian Medical Association (NMA) and the Association of General and Private Medical Practitioners of Nigeria (AGPMPN). This was a prospective hospital-based study. The sample was drawn from the list of hospitals in the Nigerian Medical Directory.8 One hundred and fifty health institutions were selected (100 in Lagos and 50 in Edo State). These institutions were located in the most and least urbanised states in south-western Nigeria (Health Zone B). Every fourth hospital was selected in Lagos State, while all the hospitals in Edo State were chosen. The medical officers in these institutions who provided the abortion care were then approached and their co-operation solicited in view of the sensitive and legal nature of the procedure. They were assured of confidentiality and the fact that information obtained would be used for research purposes only. The medical officers administered a questionnaire to every abortion care seeker in the institutions over a period of six consecutive months in 1997. Trained medical officer interviewers who visited regularly ensured that the forms were properly filled and collected the forms on regular basis. A senior doctor double-checked the questionnaires and supervised the medical officers. Each medical officer covered ten hospitals and there were two supervisors per state. Data were collected on social, demographic and educational characteristics of abortion care seekers; reasons for seeking abortion; sources of information on the place of abortion; sources of income for the procedure; and contraceptive practice. Results Data were collected from a total of 1947 subjects who sought abortion services in Lagos and Edo States. However, analysis was based on 1876 subjects, as 71 questionnaires did not contain information on important identifiers such as state, location of facility, etc. Age Distribution The age distribution of abortion care seekers is shown in Table 1. Majority of the patients (60%) were between 15 and 24 years old. Specifically, women between the ages 20 and 24 years constituted the single largest category (36.3%), followed by adolescents (15-19 years) (23.7%). A higher proportion of adolescents sought abortion in Edo State (33.8%) than in Lagos State (19.7%). The mean age of abortion care seekers was 25.9 (±6.61) years. Overall, abortion care seekers were significantly (p < 0.05) younger in Edo (23.6 ± 6.5 years) than in Lagos (25.9 ± 6.6 years). Level of Formal Education Most of the abortion care seekers (53.4%) had some secondary education or had graduated from secondary school (Table 2). Occupation Majority of the abortion care seekers were students (32.6%) and a significantly larger proportion of them was found in Edo State (42.2%) than in Lagos (28.8%) (p < 0.0001). The second most common occupation in both states was trading (26.7%), which constitutes the most prominent economically active group (Table 3). Marital Status In both states, the majority (63.2%) of abortion seekers were never married. Married women constituted 30.2% while women with other status comprised 6.6% (Table 4). History of Previous Pregnancies Of the 1576 women who provided information on this variable, 327 (20.7%) had not been previously pregnant before the current one. Of those 1249 who had been pregnant before, the number of previous pregnancies ranged from one to twelve with a mean of 3.7 (±2.3). The mean number of previous pregnancies was similar in the two states despite the fact that abortion seekers were much younger in Edo State (Table 5). Place Where Previous Pregnancies Were Terminated A total of 859 women admitted to previous terminations. An overwhelming majority (73.0%) of those previous terminations were done at hospitals, clinics and maternity homes. Only fifty eight (6.8%) of them were done at native (traditional) doctors’ homes (Table 7). Person Who Performed the Previous Termination Pregnancy terminations were largely done by doctors (80.5%) and nurses (5.0%). Gynaecologists carried out 1.4% of the terminations. Abortions were also carried out by non-qualified personnel such as chemist operators (2.7%) and traditional healers (0.6). Reasons Patients Did not Wish to Continue with Pregnancy The most common reason given by the women for not wanting to continue with the pregnancy was being in school, as pregnancy would interrupt their education (29.5%). The second most recurrent reason was not being married, which would make them to bear illegitimate children (19.3%). Other important reasons included having attained the desired family size (8.8%), unplanned pregnancy (5.8%) and not being ready for another child (last child too young) (10.2%). Financial constraints accounted for 8.5% of the reasons while the denial of pregnancy by spouse or break-up with fiancée accounted for 1.2%. Decision to Stop Current Pregnancy Of the 1847 respondents who provided information, the decision to stop a pregnancy was made by the patient in majority of the cases (47.8%). In 24.5% of the cases, the decision was jointly made by both the woman and her partner, i.e., woman and husband (15.1%) or woman and boyfriend (9.4%). In 19.3% of the cases, the decision was made by the partner; of these 11.9% were by the boyfriend and 7.4% by the husbands. Mothers were involved in 2.7% of cases either solely (2.2%) or with the patient (0.5%). The gynaecologist made the decision in 0.2% of cases. Person Who Paid for the Termination Majority of the women paid for the procedure by themselves, that is 631 out of the 1847 (34.2%) who supplied information on this variable. Boyfriends paid for 29.5% of the subjects while husbands took care of 20.8%. Others who contributed financially were mother (3.2%), sister and aunty (1.2%), self and brother (0.1%), boyfriend and the pregnant woman (3.1%). Attempt to Stop Current Pregnancy Before going to the health facility for termination, 30% (553 out of 1846) had attempted to stop the pregnancy either by themselves or by some other person elsewhere using a variety of methods. These included taking injections or other prescriptions from chemists (28.3%), self-medication with menstrogen tablet (10.0%), use of other unspecified drugs (10.7%), use of native medication (9.8%) and D & C done in a private clinic (6.9%). Other methods such as use of hot drinks, native rings and overdose of contraceptive pills were also mentioned but their frequencies were relatively low. Knowledge about Place Pregnancy could be Terminated Most of the subjects were introduced to the facility by friends (35.5%), or had used the facility before as a family clinic (19.1%). Some simply saw the hospital signpost and went there to inquire if services were provided (11.1%). Other sources of knowledge of the place pregnancy could be terminated were husbands (2.3%), mothers (2.3%), sisters (0.4%) and boyfriends (4.7%). History of Contraceptive Use At the time the patients became pregnant, 14.8% (270 out of 1554) indicated that they were currently using some form of family planning method. Of the 252 subjects who specified the methods they had used, 71 (28.2%) indicated oral contraceptive pills, 40 (15.9%) used condoms and 37 (14.7%) used ”safe periods”. Other methods used included IUCD (7.9%) and depo-provera (6.3%), etc. Contraceptive prevalence (percentage of respondents who had ever used one form of family planning method or another) was 27.4%. This was significantly higher (p < 0.05) in Lagos (29.2%) than Edo (24.1%) and was strongly associated with level of education of respondents. Among those without formal education, contraceptive prevalence was 18.2%, while it was 41.2% among those who had post-secondary education. The most common methods of contraception used were the pill (32.9%), followed by IUCD (13.3%), injectables (7.6%) and safe period (rhythm) (6.4%). Various other methods were also utilised, such as native rings or herbs, douching, non-specific prescriptions from chemists, etc. For those who had used a method and stopped, various reasons were given for doing so. These included method failure (8.6%), excessive bleeding during menstruation (7.9), weight gain and irregular menses (5.8%). Many of those who had never used a contraceptive method gave no specific reasons for their behaviour (12.7%). Others gave a wide range of reasons such as poor knowledge of family planning method (8.8%), fear of complications (4.7%), or the fear of method failure (4.9%). Only two respondents gave religious affiliation as their reason while 3.4% indicated that they were scared or ashamed to ask for a contraceptive device. Assessment of Gestational Age The gestational age at which terminations were done ranged from one to 35 weeks with a mean of 8.61 (±3.66) weeks and a median of approximately eight weeks. The majority of the patients (75%) presented for termination between six and twelve weeks. Those who presented after 12 weeks constituted 9.8% of the total. Discussion Unwanted pregnancy, and consequently induced abortion, remains a major reproductive health problem in Nigeria and in most developing countries.1-4 Majority of the abortion care seekers (60%) in this study were young people (15-24 years). Similar findings were seen in other studies conducted in this country and other developing countries.9-14 It is probably a reflection of the increasing sexual activity, risky behaviour among adolescents and a decreasing age at initiation of sexual activity.10,14,18 This portends a great danger for Nigeria especially with the current HIV/AIDS pandemic and high prevalence of other sexually transmitted infections. It is no wonder, therefore, that over half of all new HIV cases have been noted in this age group.19,20 Findings of multiple sexual partners in other studies16,17,21 would further worsen the grim picture of the risks. It is also important to note that while young women in Edo and Lagos States were about 37% of the reproductive age group, they constituted about two thirds of abortion care seekers. However, this procedure is not exclusively an activity of young people, as a significant number of the older women in the reproductive age group also sought abortion. An abortion care seeker at a hospital is likely to be someone who has had at least some secondary education. This pattern was consistent in both states. Since most women in the two states engaged in trading the single most prominent economic activity of the abortion care seekers was trading (26.7%). Similarly, as in other studies in the region, students represented a significant number of abortion care seekers. This finding is consistent with their high rate of sexual activity as well as the age distribution of the abortion care seekers.15,18,22 During the student years, adolescents experiencing the development of secondary sexual characteristics become very adventurous. It is also a period they experience a lot of freedom from parental control. As a result, there is a need to provide students with comprehensive sexuality education, which should include contraceptive counselling, abstinence and safe sex. Students comprised a significantly larger proportion of abortion care seekers in Edo State (42.2%) than in Lagos State (28.8%). This probably reflects the lower contraceptive prevalence in this state. Majority of the respondents were unmarried, as would be expected among students and adolescents. However, it is worth noting that a significant number of the abortion care seekers (30.2%) were married, signifying that an appreciable number of unplanned pregnancies also occur within marriage. This has been reported in earlier studies from Lagos.2 Consequently, expanded efforts to provide family planning cannot be over emphasised. It is no surprise that the women seeking abortions in this study listed marital status and uninterrupted education as their motivation for the procedure, given that majority of the respondents were unmarried and/or students. A significant number of abortion care seekers had previous terminations. Of these 70% were performed in hospitals and 80.5% by doctors. These findings are consistent with other studies undertaken in Nigeria1,6,23,24 and from other countries where abortion laws are restrictive.6,25,26 This is worrisome because there are still many cases of unsafe abortion in the society and, hence, mortalities. Abortion care services provided by physicians at the hospital level ought to confer many advantages such as safe procedure, post-abortion care and family planning services. That 80% of the abortion care seekers who had previous abortion performed by doctors were presenting again for abortion would probably suggest non-incorporation of family planning counselling and services with the abortion care services. It is no surprise, therefore, that majority of abortion seekers (85.2%) were not using any form of contraception at the time of conception and the total contraceptive prevalence among them was only 27.4%. This was mainly among respondents from the more urban Lagos State and strongly associated with level of education. Surprisingly, a high number of respondents got pregnant while on contraceptive methods generally known to be effective, such as the IUCD and depo-provera. It could have been as a result of missed injections or dislodgement of the IUCD. However, this was difficult to confirm. In Nigeria there is only one legal indication for termination of pregnancy: ”to save the life of a woman.” Due to this restrictive law, abortion care providers are often not optimally trained.27 In order to ensure proper training of abortion care providers, it is necessary to advocate for the review of the present provisions of the criminal and penal codes on abortion. Proper training would also ensure use of safer procedures such as manual vacuum aspiration (MVA) and medical method of termination of pregnancy. In the study, parents and other relations had little influence on the decision to terminate the pregnancy. This was probably due to lack of knowledge of the situation. On the other hand, both the woman and her consort or spouse played a significant role in the decision to terminate the pregnancy. While both contributed to the payment of the cost of the procedure, partners alone (husbands and boyfriends) paid for the procedure in 50.3% of the cases. This is probably due to the financial constraint experienced by young women. The inability to afford hospital care as well as the economic constraint has been identified as a major reason for the patronage of unskilled providers.4 Peer influence has been identified as a major factor affecting the sexual behaviour of young persons and this would probably affect their decision to seek abortion or not.21 Friends suggested where to go for an abortion in 42.9% in Edo State, which incidentally also had a high number of young persons seeking abortion care. It is appropriate to assume that these friends have also at some point sought abortion for themselves or other friends. Targeting young persons in sexuality education is therefore bound to have multiplier effects, as they tend to circulate sexual information among themselves. In conclusion, abortion needs cut across all reproductive age groups but remain a major health problem of young persons, who also exhibit a large unmet need for contraception. With the current HIV/AIDS scourge, it has become even more urgent that this group of people be targeted and their needs addressed. In addition, to reduce the incidence of multiple pregnancy terminations and encourage women to seek abortion care from qualified providers, it is imperative that policymakers provide an enabling legal environment for proper training of these providers and safe delivery of the services. Acknowledgement We wish to acknowledge the invaluable contributions of our consultants, supervisors and field staff in the planning and conduct of this study. The John D. and Catherine T. MacArthur Foundation (Grant No. 27895) supported the study. The findings and conclusions are those of the authors and do not necessarily represent the views of The John D. and Catherine T. MacArthur Foundation. REFERENCES
©Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04044t2.jpg] [rh04044t4.jpg] [rh04044t1.jpg] [rh04044t5.jpg] [rh04044t7.jpg] [rh04044t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}