 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 8, No. 3, Dec, 2004 pp. 198-206 Relation of Parity to Pregnancy Outcome in a Rural Community in Zimbabwe F Majoko1,4, L Nyström2, SP Munjanja1, EMason3 and G Lindmark4 1Department of Obstetrics & Gynaecology, University
of Zimbabwe, Harare, Zimbabwe. 2Department of Public Health and
Clinical Medicine, Epidemiology, Umea University, Sweden. 3WHO
Country Office, Harare, Zimbabwe. 4Department of Women’s & Children’s
Health, Section for International Maternal & Child Health, Uppsala
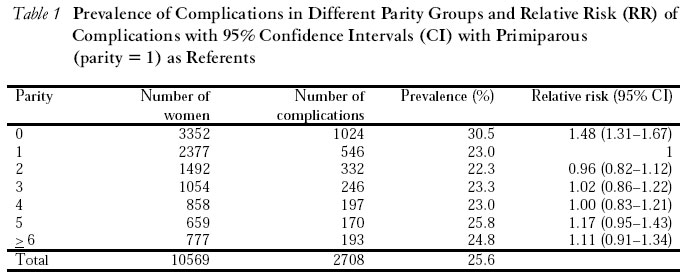
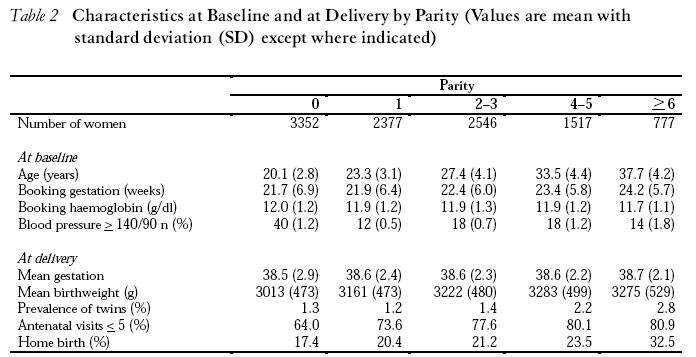
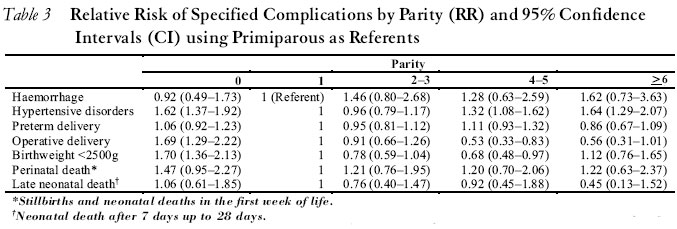
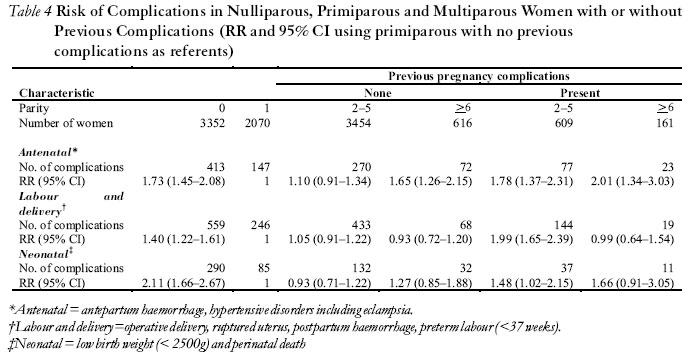
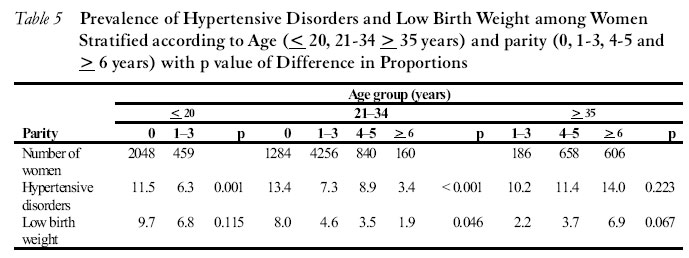
University, Sweden. Code number: rh04053 ABSTRACT This population-based cohort study was conducted to compare pregnancy complications and outcome among nulliparous, low (1-5) and high (> 6) parity women. Women who registered for antenatal care and gave birth in Gutu District, Zimbabwe, between January 1995 and June 1998 were classified into groups by parity. The women were compared for baseline characteristics, utilisation of health facilities and occurrence of pregnancy complications such as hypertensive disorders of pregnancy, haemorrhage, pre-term delivery, operative delivery, low birth weight and perinatal death. In estimating risk, primiparous (parity = 1) women were used as referents. Pregnancy records for 10,569 women were analysed. Mean ages of nulliparous and high parity (> 6) women were 20.1 and 37.7 years respectively (p < 0.001). Prevalence of anaemia at booking (haemoglobin <10.5 g/dl) was reduced in nulliparous compared to multiparous women (11.7% vs 16.8%; p > 0.001). Nulliparous women were likely to book early (< 20 weeks) for antenatal care, have a higher number of visits (> 6) and fewer home births. Nulliparous women had higher risk for low birth weight (RR 1.70; 95% CI 1.36 - 2.13). Compared to low parity women, nulliparous and high parity women had an elevated risk of hypertensive complications RR 1.62 (95% CI 1.37-1.92) and RR 1.64 (95% CI 1.29 - 2.07) respectively. The risk of developing any pregnancy complications was highest in nulliparous women (RR 1.48; 95% 1.31- 1.67). In conclusion, nulliparous women had an increased risk of pregnancy complications. High parity women with no previous complicated pregnancy were at low risk of complications. (Afr J Reprod Health 2004; 8[3] 198-206 ) RÉSUMÉ Le rapport entre la parité et le résultat de la grossesse dans une communauté rurale au Zimbabwe. Cette étude cohorte, qui est basée sur la population, a été menée afin de comparer les complications et les résultats chez les nullipares, les femmes à faible parité (1-5) et celles à haute parité ( >6). Les femmes inscrites auprès du service de la consultation prénatale et qui ont accouché dans le District de Gutu, Zimbabwe, entre janvier 1995 et juin 1998 ont été classifées en groupes selon la parité. Les femmes ont été comparée pour déterminer les caractéristiques de base, l’utilisation des infrastructures médicales et les incidences des complications pendant la grossesse telles les désordres causés par l’hypertension pendant la grossesse, l’hémorragie, l’accouchement avant-terme, l’accouchement opératoire, le poids de naissance faible et le décès prénatal. Pour évaluer le risque, les femmes primipares (parité = 1) servaient de référentes. Les dossiers de grossesse des 10.569 femmes ont été analysés. Les âges moyens des femmes nullipares et des femmes à haute parité ( 6) étaient 20,1 et 37,7 ans respectivement (p < 0, 001). La prévalence de l’anémie au moment de l’inscription (hémoglobine < 10,5g/dl) était réduite chez les femmes nullipares par rapport aux femmes multipares (11,7% vs. 16,8%; p = 0,001). Il y avait plus la chance que les femmes nullipares soient inscrites tôt ( 20 semaines) pour la consultation prénatale, qu’elles aillent plus fréquemment à la consultation et qu’elles accouchent moins à la maison. Les femmes nullipares étaient plus en danger d’avoir des poids de naissance faibles (IRR 1,7; 95% CI 1,36-2,13). Comparées aux femmes à la parité faible, les femmes nullipares à haute parité courent le risque des complications de l’hypertension RR 1,62 (95% CI 1,37-1,92) et RR 1,64 (95% CI 1,29-2,07) respectivement. Le risque des manifestations des complications de grossesse était le plus élevé chez les femmes nullipares (RR 1,48; 95% 1,31-1,67). Pour conclure, les femmes nullipares couraient un surcroît de risque des complications de grossesse. Les femmes à haute parité qui n’avaient pas de complications de grossesse ultérieures couraient peu de risque de complications. (Rev Afr Santé Reprod 2004; 8[3]198-206) Key Words: Nulliparity, grand multiparity, pregnancy complications, risk factors Introduction The relationship between parity and pregnancy complications continues to be of interest to obstetricians.1-5 Parity has been used as a risk marker with nulliparous and grand multiparous women classified as at higher risk of pregnancy complications.6 Nulliparous women are considered to be at risk of pregnancy-induced hypertension and fetopelvic disproportion leading to operative delivery, whereas the grand multiparous are considered to be at risk for haemorrhage, malpresentation, anaemia, uterine rupture and complications associated with chronic medical problems such as diabetes and hypertension.7 In most rural settings of developing countries there is limited access to medical care and, therefore, the need to identify women whose pregnancy is at increased risk of complications is an important part of antenatal screening. There are few studies from sub-Saharan Africa that address risks of nulliparity independent of extremes of maternal age. In developed countries with universal access to antenatal care and skilled attendant at delivery, high parity is no longer considered a risk marker for pregnancy complications.2,3,5,8 There is a tendency for practitioners in developing countries to adopt practises from developed country settings and literature from well-resourced areas suggest that there are no differences in pregnancy outcome between low and high parity women. However, there is need for caution in translating such results to a rural area in a developing country. The Zimbabwe Ministry of Health and Child Welfare recommends hospital delivery for all women during the first and from the seventh pregnancy (parity > 6). Women in the second to sixth pregnancies (parity 1-5), who have had no pregnancy complications, were encouraged to utilise the local health centre for delivery. With recent studies showing no increase in risk for grand multiparous women, we evaluated the relationship between parity and pregnancy complications in a rural setting in Zimbabwe. We wanted to confirm if the view that high parity is not associated with an increase in pregnancy complications is also applicable in this setting and to assess the need to maintain current criteria for hospital delivery. Materials and Methods An antenatal care (ANC) trial conducted in Gutu District between January 1995 and June 1998 enrolled women into two antenatal care models. In this study we used data from the trial to evaluate the relationship between parity and pregnancy complications. The study had ethical approval from the Medical Research Council of Zimbabwe and the medical research Ethics Committee, Uppsalo University, Gutu District had 25 health facilities that included one district hospital, and twenty four rural health centres (RHC) that served an estimated population of 195,000. Nurse-midwives, who could not treat most obstetric complications, provided pregnancy care at the RHC. Operative deliveries were only performed at the district hospital or at a hospital in one of the neighbouring districts. It is estimated that more than 90% of women in Gutu received antenatal care at least once and that 15-25% deliveries took place at home.9-11 The majority of home births were conducted by trained traditional midwives (TM) and women were advised to attend the RHC as soon as possible for the baby to receive BCG vaccination. Based on population demographics we expected 4,600 women would give birth in the district each year. Women who booked for care directly at the district hospital were excluded from the ANC trial since their access to medical practitioners was different from the rest of the district. Maternal characteristics, medical and obstetric history, details of index pregnancy were recorded at the booking visit and examination findings were entered in the woman’s pregnancy record at subsequent visits. Labour and delivery outcome was recorded at time of birth and the antenatal record was retained until the postnatal visit. Labour and delivery outcome for women who had home births were collected from reports by TM and follow-up home visits. The pregnancy record was computerised and included in the ANC database. All women registering for antenatal care in the RHC were included in the database. In this analysis we classified women according to parity at enrolment for antenatal care and computed their risks of pregnancy complications. We defined parity at time of booking as the number of prior pregnancies beyond 26 weeks gestation. Thus, women in the first pregnancy were classified nulliparous and others as primiparous (parity = 1), parity 2-3, 4-5 and parity >6. The complications of interest included antepartum haemorrhage, hypertensive disorders of pregnancy, pre-term delivery (< 37 weeks), operative delivery, low birth weight (< 2500g), postpartum haemorrhage and perinatal death. We calculated risk of complications arising in the antenatal period, during labour and delivery and for the neonate for each parity group to determine the relationship between increasing parity and complications. Epi Info software (CDC/WHO) was used for computerisation and statistical analysis. We calculated the prevalence of complications for each parity group. As the prevalence for complications was constant from the second to sixth pregnancies (parity 1-5) we presented some of the data as comparison between nulliparous, primiparous, low parity (2-5) and high (> 6) parity women. In evaluating the relationship between parity and pregnancy complications including adverse perinatal outcome, we considered primiparous women (parity = 1) as referents. Relative risk (RR) with 95% confidence intervals (CI) was used to compare risks of complications and neonatal outcomes. We considered p value < 0.05 to indicate a significant difference. One-way analysis of variance (ANOVA) was used for comparison of proportions between groups. Records with missing values in a variable were excluded from the analysis relating to that variable. Results We analysed 10,569 records of women who registered for antenatal care during the study period. We expected 13,800 births in the district during a three-year period. Recruitment was for 33 months and we estimate that our sample includes 85% of births in the district during this period. Nulliparous women constituted 32% of the study population with low and high parity women making 61% and 7% respectively. We calculated the prevalence of specified complications (antepartum haemorrhage, hypertensive disorders of pregnancy, pre-term delivery, operative delivery, postpartum haemorrhage and perinatal death) for the parity groups (Table 1). Compared to women with one prior pregnancy, nulliparous women had an almost 50% increased risk of complications (RR 1.48; 95% CI 1.31-1.67) but there was no difference in risk of complications between low (2-5) and high (> 6) parity women. Nulliparous women were significantly younger and booked earlier than multiparous women (Table 2). The prevalence of anaemia at booking (haemoglobin <10.5g/dL) was lower in nulliparous than in women of parity > 6 (11.7 vs 16.8; p <0.01). The proportions of nulliparous and high parity women with blood pressure > 140/90mmHg at booking were 1.2 % and 1.8% respectively (p = 0.251). Multiple births were more common in high parity women 2.8% vs 1.3% in nulliparous women (p = 0.006). Multiparous women were more likely to book late for antenatal care, have fewer visits and to have a home birth (Table 2). There was no difference in gestation at delivery across the parity groups. Multiple births were more common in high parity women 2.8% vs 1.3% in nulliparous women (p = 0.006). Multiparous women were more likely to book late for antenatal care, have fewer visits and to have a home birth (Table 2). There was no difference in gestation at delivery across the parity groups. There was no difference in the risk for haemorrhage, pre-term delivery (< 37 weeks) and perinatal death across the parity groups (Table 3). Compared to primiparous women, nulliparous and women of parity > 4 had an elevated risk of hypertensive disorders of pregnancy (RR 1.62; 95% CI 1.37-1.92; RR 1.32; 95% CI 1.08-1.62 and RR 1.64; 95% CI 1.29-2.07) for nulliparous, parity 4-5 and parity > 6 respectively. In addition nulliparous women had a higher risk of operative delivery (RR 1.69; 95% CI 1.29-2.22) and low birth weight (< 2500g) babies (RR 1.70; 95% CI 1.36-2.13) (Table 3). To control for previous complications we compared the risk for antenatal, labour and delivery as well as neonatal outcome in nulliparous, primiparous women with no previous complications and multiparous women with or without complications in a previous pregnancy (Table 4). Nulliparous women had significantly increased risk of complications at all stages of pregnancy. Although high parity women had an increased risk of antenatal complications, the majority of cases were attributed to hypertensive disorders of pregnancy. In women with no previous complications, there was no difference in risk of complications that occurred during labour and delivery or for the neonate between low and high parity women (Table 4). Women with previous complications had an increased risk of complications independent of parity. To further control for the effect of age on hypertensive disorders and low birth weight, which showed significant difference on univariate analysis, we stratified the women into age groups (Table 5). There were no women of parity > 3 under age of 20 years and only four nulliparous women older than 34 years. In each age category there was no significant increase in prevalence of hypertensive disorders with increasing parity. In women under 35 years, prevalence of hypertensive disorders decreased as parityhypertensive disorders with increasing parity. In women under 35 years, prevalence of hypertensive disorders decreased as parity increased. There were two direct maternal deaths involving women who gave birth at home. One nulliparous woman had a pre-term home delivery complicated by postpartum haemorrhage. The other woman died following a home delivery of her fourth child when she developed puerperal sepsis. Uterine rupture occurred in three women of parity 0, 4 and 6. The two parous women were admitted from home in obstructed labour whereas the nulliparous woman was in the district hospital when she experienced uterine rupture associated with prolonged use of oxytocin in obstructed labour. Discussion Our objective was to determine the relationship between increasing parity and pregnancy complications in a low resource setting. We also wanted to determine if the recommendation for hospital delivery on the basis of parity alone should continue. Our results, from a rural developing country setting, agreed with studies from developed countries that parity per se was not an independent risk marker for obstetric complications. In our study, nulliparity was associated with an increased risk for low birth weight, hypertensive disorders of pregnancy, operative delivery and perinatal death. There is no universally accepted definition for grand multiparity.12 The World Health Organization (WHO) classifies women with six previous deliveries after 24 weeks gestation as grand multiparous6 whereas the International Federation of Gynaecology and Obstetrics (FIGO) defines five deliveries as grand multiparity, and there has been a suggestion to consider more than four deliveries as grand multiparity.4 We adopted the WHO definition for grand multiparity (parity > 6). In Gutu District, nulliparous women made greater use of the health facilities for antenatal and intrapartum care. The higher proportion of nulliparous women with more than five antenatal visits was due to registering for care earlier than multiparous women and higher compliance with antenatal care recommendations. The observation that grand multiparous women were less likely to follow antenatal advice appears to be true for this population, as high parity women booked late for antenatal care, had fewer antenatal visits and more home deliveries.13 We found an increased risk of hypertensive disorders of pregnancy in nulliparous and high parity women similar to previous reports.3,8,14-16 In our study the prevalence of hypertension at the booking visit was elevated in women of parity > 4 and appears to be a function of age not parity per se. Previous reports have not shown a consistent relationship between parity and the risk for haemorrhage. There have been reports of increased risk of haemorrhage in nulliparous women,14 in grand multiparous12,17 and of no difference.15,18 We found no difference in the risk of obstetric haemorrhage across the parity groups. The majority of reports comparing low to high parity women show no difference in mode of delivery2,12,15,17,18 or reduced operative delivery in high parity women.3,8,13 Our results showed nulliparous women had an increased risk of low birth weight babies and operative delivery. Similar to previous reports we found no difference in neonatal outcome between low and high parity women.5,14,15 Among women with no previous pregnancy complications we found no difference in intrapartum and neonatal complications between low and high parity women. We therefore consider both low and high parity women with previous uncomplicated pregnancies suitable for delivery in the RHC. The policy of recommending hospital delivery for all high parity women, which was in place in Zimbabwe and other low resource settings, needs review. In our study, the prevalence of complications was highest in nulliparous women and showed no difference across the multiparous groups. In a setting with limited access to transport for intrapartum transfer, we recommend hospital delivery for nulliparous women, as there is an increased need for operative interventions. Limitations in this study include missing values in some variables especially among women who had home births. The variable with the largest missing values was birth weight, which was recorded in 80% of cases since it was missing in the majority of home births. The effect of missing values was, however, minimised by excluding records with missing values in the analysis of each variable. Women with missing values in some variables were not different from the remainder of the sample and they contributed information in other variables. The small sample size in some of the subgroups, such as parity > 6 that constituted only 7% of the sample, may be responsible for failure to detect differences especially of the confounding effect of age on hypertensive disorders. Conclusion Our results show that nulliparous women had an increased risk of hypertensive disorders, operative delivery and delivery of low birth weight infants. High parity women with no previous complicated pregnancy were at low risk of developing complications and can be recommended for RHC delivery. Acknowledgements This antenatal care study in Gutu was funded by the Swedish International Development Co-operation Agency (Sida/SAREC) through the Sida-University of Zimbabwe Reproductive Health Research Programme. REFERENCES
©Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04053t2.jpg] [rh04053t5.jpg] [rh04053t3.jpg] [rh04053t1.jpg] [rh04053t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}