 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
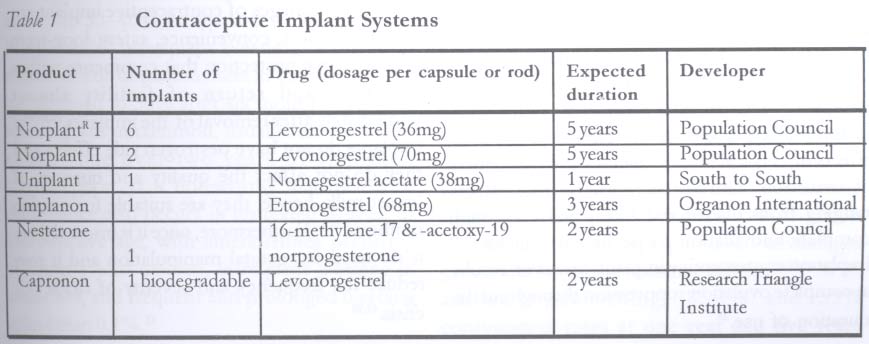
African Journal of Reproductive Health, Vol. 9, No. 1, April, 2005 pp. 16-23 Review Article Contraceptive Implants OA Ladipo and SA Akinso Association for Reproductive and Family Health (ARFH), Plot 815A Army Officers' Mess Road, Near Ikolaba Grammar School, Agodi GRA, Ikolaba, P. O. Box 30259, Secretariat, Ibadan, Nigeria. Code Number: rh05004 Abstract In response to the need of some women for long-acting, effective and safe contraceptives, the scientific community developed non-biodegradable progestational subdermal implants that act by making the cervical mucus viscous, with ovulation inhibition and thinning of the endometrial lining. The contraceptive protection is within 24 hours and the cumulative failure rate is low. Contraceptive implants require little or no motivation following adequate counselling. In current use are multirod implants (Norplant I and Norplant II Jadelle) and single rod implant (Implanon and Uniplant). Although menstrual symptoms associated with progestational regimens are the major compliance and acceptability factors within the first year of use, menstrual disturbance generally improves. Continuation rates for implant use are high among those who have had adequate pre-insertion counselling because the perceived advantages greatly outweigh the nuisance effects. Other side effects of implants are similar to those observed with hormonal pills - headache, weight changes, mood swings and abdominal bloating. Training of physicians and nurses in the art of insertion and removal techniques is a pre-requisite for a successful implant programme. This should also be backed by integration of implants into the national commodity logistics systems to ensure adequate local budgetary provision for contraceptive implant procurement rather than reliance on donor supply. (Afr J Reprod Health 2005; 9[1]: 16-23) Key Words: Contraception, implant, counselling, insertion, removal Résumé Les implants contraceptifs. En réponse au besoin des femmes des contraceptifs à longue durée d'action, efficace et sans danger, la communauté scientifique a produit des implants sous-dermiques progestatifs qui ne sont pas biodégradables et qui agissent par rendre visqueux les mucosités cervicales, avec la mise au repos de l'ovaire et l'amincissements de la muqueuse andométriale. La protection contraceptive dure pendant 24 heures et le taux d'échec cumulatif est faible. Les implants contraceptifs n'ont besoin que de très peu de motivation ou aucune si l'on suit assez de conseil. Les implants multi-bacilles sont utilisés actuellement (Norplant II et Norplant II Jadelle) et ainsi que les implants mono-bacilles (Implanon et Uniplant). Quoique les symptômes menstruels liés aux schémas progestatifs constituent les facteurs majeurs de conformité et d'acceptablilité au cours de la première année d'utilisation, le désordre menstruel s'améliore en général. Les taux de continuation de l'utilisation de l'implant sont élevés chez ceux qui ont eu de conseil approprié de pré-insertion parce que les avantages perçu l'emportent sur les effets embêtants. Les autres effets secondaires des implants sont semblables à ceux des pilules hormonales — maux de tête, modifications dans le poids, sautes d'humeur et la distension gazeuse abdominale. La formation des médecins et des infirmières dans la technidque de l'insertion et de l'enlèvement est une condition préalable pour assurer un programme d'implant réussi. Ceci devait être soutenu par l'intégration des implants dans les systèmes de la matière première nationale pour assurer la disponibilité d'un budget national adéquat pour l'achat de l'implant contraceptif pultôt que de dépendre des provisions de la part des donateurs. (Rev Afr Santé Reprod 2005; 9[1]: 16-23) History and Development The development of contraceptive implants was made possible by the discovery of silicone rubber in the 1940s. Silicone was found to have excellent bio-compatibility in the human body and it is widely used in various surgical applications, e.g., heart pace makers and in-dwelling drains or stunts. The search for long-acting contraceptive method that would provide continuous and prolonged actions on effectors received a remarkable impulse in 1964, when Folkman and Long1 published their study demonstrating that silastic tubes could serve as reservoir for administration of drugs. Silastic (polydimethylsiloxane) has been used thereafter for the delivery of lipophilic drugs. Two years later Dziuk and Cook2 did further studies placing steroid containing silastic capsules in a saline solution. They found the release rate to be constant and dependent on the wall thickness of the capsule rather than the drug concentration in the implant. These authors then placed gestagen implants subcutaneously in sheep and observed a significant oestrus reduction. Segal and Crotarto3,4 also concluded that silastic implants containing low doses of gestogens would be applicable for the control of human fertility. With this technology, the Population Council developed and patented Norplant and Norplant-2. Subdermal contraceptive implants are either biodegradable or non-biodegradable (Table 1). The former is under clinical trial. The earliest clinical trials using subdermal implants began in 1968. The silicone capsules were filled with the progestin, chlomadinone acetate.5 However, clinical trials in the United States terminated when chlomadinone acetate was linked with breast cancer in animals.6 Between 1970 and 1978 megesterol acetate-filled implants showed the development of breast nodules in dogs,7 while trials resulted in adnexal masses and contraceptive failure resulted in high incidence of ectopic pregnancies. The findings were attributed to release of low-dose progestin without inhibition of ovulation.8 Other progestins used were norethindrone, norgestrinone and levonorgestrel. The former showed low potency while norgestrinone and levonorgestrel showed low pregnancy rates and high continuation rates.4,9-11 With levonorgestrel implants, most menstrual cycles were anovulatory during first year of use,12 and it is the most widely used because of its high potency per volume.13 Norplant is a first generation contraceptive implant system while Norplant II (Jadell), which consists of two silastic-covered rods - uniplant a one-silastic covered rod and implanon, which consists of one ethylene vinylacetate (EVA) rod - is classified as second generation subdermal contraceptive implant system. Development of the second generation implants was due to the need to reduce problems associated with the six implant system (Norplant). Improvements in existing systems is also attributed to the need to make them less obvious under the skin; the need to find progestogenic compounds that are less androgenic than levonorgestrel so that acne, weight gain and perhaps other side effects would be less common; the need for biodegradable implants, thus eliminating the need for removal; and the need to use simple disposable devices to speed insertion and reduce the risk of blood-borne disease transmission.14,15 The implants currently in clinical use are Norplant, Norplant II (Jadelle), Implanon and Uniplant.
Rationale for Sustained Release Subdermal Contraceptives The rationale for the development of subdermal contraceptives is their long duration of action, continuous and steady steroid blood levels and avoidance of the `first pass' peak effect through the hepatic portal system, thus avoiding the peak plasma levels of steroids associated with oral use without compromising contraceptive efficacy.16 The higher bio-avaicavity leads to lower doses of steroids being administered with possible parallel reduction in adverse effects.17
Mode of Action of Contraceptive Implants As with other progestogen only contraceptives, the subdermal implants are thought to have three modes of action. First, the progestogen implants render the cervical mucus viscous, scanty and impervious to sperm.18,19 Secondly, suppression of oestradiol-induced cyclic maturation of the endometrial lining causing hypotrophic changes.19,20 This provides contraceptive protection in the unlikely event of the failure of the joint effects of cervical mucus changes and prevention of ovulation. Thirdly, there are ovarian effects ranging from disordered luteal phase through complete anovulation to persistent follicles.19-23 Implanon contraceptive implant, however, results in complete ovulation suppression throughout the duration of use.28 Efficacy Contraceptive implants have a high efficacy rate. Norplant-I1 has a cumulative failure rate of one per 100 users after five years of use (0.26 per 100 women yearly).24 Norplant-II (Jadelle) has a similar cumulative failure rate after three years.25 Studies on implanon implants showed no pregnancy in 1,716 women treated in 53,530 cycles (4,103 women years), resulting in a pearl index of 0.0 (95% CI 0.00-0.07).22 Implants require little user compliance or motivation following adequate counselling, hence, the use-effectiveness rates closely approximate theoretical effectiveness.
Return of Fertility Contraceptive implants do not impair subsequent fertility because post-removal conception rates are virtually identical with those of IUD and injectable contraceptive users.26 Rates and outcomes of planned pregnancy were studied among users of four long-acting contraceptives: an earlier version of the rods, NorplantR capsules and two intrauterine devices. Within the first 12 months of removal of the implants, 84 per 100 rod users and 83 per 100 Norplant capsule users became pregnant, and at 24 months 92 per 100 rod users and 87 per 100 Norplant users successfully achieved a pregnancy.27
Advantages of Contraceptive Implant The key advantages of contraceptive implant are its effectiveness, convenience, safety, long-term contraceptive protection that commence within 24 hours and return of fertility almost immediately after removal of the implants.22,24,28,51 Implants do not have oestrogen side effects and they do not affect the quality and quantity of breast milk, hence, they are suitable for nursing mothers.4,51,52 Furthermore, once it is inserted there is no need for genital manipulation and it may reduce the frequency and severity of sickle cell crisis.49,50 Disadvantages Although there are disadvantages of contraceptive implants, these are of little importance, because the benefits of implants far outweigh their disadvantages. During the pre-insertion counselling, potential disadvantages should be discussed, for example, the need for a trained health provider to perform minor surgical procedure for insertion and removal of the implants, potential risk of minor surgical procedure (amenorrhoea, bruising, infection, discomfort after insertion or removal of implants, and sometimes the implant may be visible). Furthermore, implants do not protect against STI/HIV.24,25,41,47,48
Side Effects The most common side effects of contraceptive implants that limit the methods acceptable is the disruption of menstrual cycle. These include prolonged menses, spotting between periods and oligomenorrhoea. About 50-60% of implant users report irregular bleeding patterns during their first year of use,16,28 however, symptomatic improvement is generally observed the longer the duration of implant use. The changes in menstrual bleeding pattern vary widely, and currently it is not possible to predict the change a particular client may experience. Implanon and Uniplant contraceptives have similar bleeding pattern to that of Norplant, although amenorrhoea occurred more frequently at about 30-40% compared to 20-30% for Norplant.29,30 Infrequent bleeding occurred in about 50% of Implanon users in the first months but declined to 30% after six months. Frequent bleeding was uncommon, usually less than 10% at any time over two years of Implanon contraception. It is noteworthy that menstrual disturbance also occurs in untreated women of reproductive age, with amenorrhoea occurring in about 1% of women, infrequent bleeding in about 8%, and frequent and prolonged bleeding in less than 0.1%.31 The basis of action of all hormonal methods of contraception is the interference with the pituitary-ovarian cycle that controls the cyclicity of menstruation. Users of progesterone-only contraceptives are more likely to experience these side effects than users of combined oral contraceptive pills. This is because the oestrogen in the combined pill regulates bleeding in order to stimulate a pattern of normal menstruation. Prolonged and frequent bleeding among implant users are more associated with low serum oestradiol and progesterone, while bleeding irregularities are rarely observed during periods of luteal phase levels of oestradiol and progesterone.32 While there has been some progress in understanding the mechanism of normal and abnormal menstruation,33 there is a relative lack of progress in the actual prevention and treatment of the menstrual disruption associated with progesterone-only contraceptives. There is no universal treatment criteria for implant users who experience menstrual disturbances in the first few months of use; however, some patients benefit from the use of low dose combined pills compared to ethinyl oestradiol alone.34 The need to add the use of an oral method to the implant is a drawback but it should be regarded as a short-term palliative treatment of menstrual disturbance. An alternative is the use of ibuprofen or other non-steroidal anti-inflammatory drugs but not aspirin. Despite these bleeding irregularities, pro-portionately more women have increased rather than decrease in blood haemoglobin.36-38 In selecting patients for contraceptive implant, it is most important that adequate pre-treatment counselling about menstrual disturbance is understood by the patient. Continuation rates for implant use is high among those who have had adequate pre-insertion counselling because the perceived advantages greatly outweigh the nuisance effects.13,17,19 With adequate counselling, 83.4% and 53% continuation rates at one year and five years respectively have been reported for Norplant, while for Jadelle the continuation rates for one, three and five years are 88.3%, 60.0% and 41.5% respectively.25 The two years continuation rate for Implanon was reported to be 69%. Medical problems that sometimes lead to implant removal are side effects common to all hormonal methods of contraception. Their occurrence vary between 10 and 14.5%.19,35 These side effects include headache, weight changes, mood swings, abdominal bloating and discomfort, acne, loss of libido, nausea and alopecia.
Drug Interaction Drugs that are liver enzyme inducers may reduce the contraceptive efficacy of hormonal implants, e.g., rifampicin and griseofulvin, and anticonvulsants, phenytoin, carbamazepine, ethosuximide and barbiturates. Clients on long-term use of these medications should be advised to use a back-up contraceptive method such as barrier method, which has additional benefit of protection from sexually transmitted infections.
The Nigeria Experience The use of Norplant was introduced into Nigeria by the author in 1985, following one-week training with Dr Frank Alverez of Dominican Republic. Training of trainers for doctors and midwives in the art of counselling, insertion and removal was subsequently conducted at the Fertility Research Unit, University College Hospital, Ibadan. As part of the pre-introductory trial of Norplant in Nigeria, FHI conducted acceptability study on women who were potential acceptors of Norplant in Ibadan, Ilorin, Jos, Benin and Zaria. Nearly half of the women interviewed expressed interest in Norplant, majority were over 35 years of age and majority had six or more children. Fifty per cent of women enrolled were using Norplant for limitation purposes. The first year use conclusion was that Norplant is a highly effective, safe and acceptable contraceptive among Nigerian women of different ethnic groups, and it is associated with a high degree of client satisfaction. The pooled continuation rate was 90.1% after 12 months, 84.9% after 24 months and 77.1% after 36 months of Norplant use. Ninety seven per cent of Norplant users were satisfied with the method. Between 1989 and 1999, the Association for Voluntary Surgical Contraception (AVSC) supported a Norplant operation research in Abeokuta, Lagos, Calabar, Port Harcourt and Maiduguri. During the study, Norplant accounted for 20% of users of clinical methods, and it did not interfere with the provision of other family planning services. The observed limited access to Norplant services at some sites was attributed to unavailability of doctors, Norplant services on a weekly basis and limited number of trained personnel. However, 94.6% of Norplant users would recommend the method to their friend. Uniplant, a single rod contraceptive implant, was introduced in 1987 as part of phase III clinical trial at Lagos, Ibadan and Jos. Uniplant is a proprietary compound of Theramex Monaco, France. The clinical experience with Uniplant was similar to that of Norplant from the point of view of effectiveness, acceptability, continuation rates and client satisfaction. It is, however, preferred to the six-rod implant because of the ease of insertion and removal.
Future of Implant Contraceptives in Nigeria If implant uptake is to increase in the future, there is need for a strong government policy commitment to family planning in view of the high fertility rate that characterises every Nigerian ethnic group. Total fertility rate of 5.9 means that our population of 120 million may double in 23 years with adverse socio-economic, political, health and environmental consequences. There is need for financial mobilisation to address key issues like poverty and illiteracy that constitute formidable barriers to the promotion of ideas of a small family. Integration of health and family planning services and provision of quality care will ensure efficient and effective delivery of services as well as help in building rapport with the community. Adequate publicity should be mounted to inform the public about the advantages of implant contraceptive using the pre-introductory national data that indicate implant safety and efficacy. Appropriate promotional IEC materials should also be developed for clients and service providers. Contraceptive implants should be integrated into the national commodity logistics system to ensure adequate local budgetary provision for contraceptive implant procurement rather than reliance on irregular and inadequate donor supply. It is essential to have adequate supply of contraceptive implants in all service centres, both private and public, in order to avoid the "out-of-stock" syndrome that tends to act as a disincentive to acceptors. Training of physicians and nurses in the art of insertion and removal techniques is pivotal to a successful implant programme. Acquisition of this skill by nurses is important in view of the limited number of doctors at service centres. In each family planning centre there should be enough trained personnel for implant insertion on every working day to ensure timely insertion for motivated clients and removal for clients who wish to discontinue. All implant service providers should also be trained in counselling, because findings from different cultural settings suggest that the provision of adequate information about implants leads to tolerance of some known side effects, in particular menstrual problems. Counselling and education remain powerful tools in overcoming barriers of poverty, illiteracy and conservative social customs in promoting the ideas of small families. Conclusion Contraceptive implants are effective and safe long-term contraceptive methods that meet the needs of women who desire long-term contraception, or women who decline sterilisation after completion of their family, or women with oestrogen intolerance. With adequate regulatory approval and financial provision for procurement, the uptake of implants by Nigerian women would improve. Counselling should precede insertion and removal, and adequate provision should be available to address any concerns of the clients. The contraceptive implants without any doubt are a worthy addition to the cafeteria of contraceptive methods, and in many African cultures the second generation of implants would appeal to many women because of the reduced number of implants, contraceptive effectiveness and safety. References
© Women's Health and Action Research Centre 2005 The following images related to this document are available:Photo images[rh05004t1.jpg] |
| |||||||||

{kind=link}