 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 9, No. 1, April, 2005 pp. 24-31 Original Research Articles Effect of Uniplant on Liver Function in Egyptian Women with Asymptomatic Hepatitis B Virus Infection Ayman H Shaamsh1, Hosam T Salem1, Mamdouh M Shaaban1, Sharaf A Ghaneima2and Shaaban R Helal3 Departments of 1Obstetrics & Gynaecology, 2Biochemistry and 3Clinical Pathology, Faculty of Medicine, Assiut University, Egypt.
Code Number: rh05005 Abstract Uniplant is a single 35mm contraceptive implant releasing nomegestrol acetate with an effective life span of one year. This study was undertaken to evaluate the possible effects of three-year use of uniplant on some liver enzymes (SGPT, SGOT and GGT) in Egyptian women and to evaluate whether the past asymptomatic hepatitis B virus infection would predispose to any changes in these enzymes. This is an uncontrolled prospective study including 187 women of reproductive age who desired contraception for three years (three segments each year). They were apparently healthy on clinical assessment with no history of jaundice or liver diseases. They also had normal levels of liver function enzymes (SGPT, SGOT & GGT). Fasting blood samples were drawn at admission for assessing the levels of these liver enzymes and to detect anti-HBS antibodies as a marker of past asymptomatic hepatitis B virus infection (HBV) and HBS antigen to diagnose the chronic carrier state. The liver enzymes were measured at 6th, 12th, 18th, 24th, 30th and 36th month of use, and 3-6 months after implant removal. Out of 187 subjects enrolled 159, 83 and 33 women completed one, two and three years of Uniplant use respectively. The mean levels of SGPT, SGOT and GGT showed slight but significant elevations at the end of the first and second years of use compared to the pre-insertion levels. By the end of the third year, the elevated mean values of all enzymes gradually decreased to approach the pre-insertion levels without any significant differences. The percentage of anti-HBS antibodies positive titre due to past asymptomatic infection was 23.3% (n = 41) while HBsAg positive antigenaemia (i.e., carrier state) was 3.4% (n = 6). In both groups of women - anti-HBS antibodies positive (n = 41) without antigenaemia and anti-HBS antibodies negative (n = 129) - the changes in the mean levels of all enzymes during uniplant use were closely similar without any statistical significance. These results demonstrated that: (1) uniplant induced slight but significant elevations in the mean levels of SGPT, SGOT and GGT; these elevations were within the normal ranges, completely reversible and of doubtful clinical significance. (2) The non-carrier women who had been exposed to past asymptomatic HBV infection showed no significant effects on the studied liver enzymes compared to the normal women during long-term use of Uniplant. (Afr J Reprod Health 2005; 9[1]: 24-31) Résumé L'effet de l'Uniplant sur le fonctionnement du foie chez les femmes égyptiennes atteintes de l'infection hépatite virale B. L'Uniplant est un seul implant contraceptif de 35mm qui libère l'acétate nomegestrol ayant une durée de vie d'une année. Cette étude a été menée pour évaluer les effets possibles d'une utilisation de trios années de l'Uniplant sur certains enzymes du foie (TGPS, TGOS et TGG) chez les femmes égyptiennes et pour vérifier si une hépattite virale B asymptomatique ultérieur pourrait disposer à des changements dans ces enzymes. Il s'agit d'une étude prospective sans contrôle qui comprend cent quatre-vingt-sept femmes en âge de reproduction qui avaient de la contraception pour trios ans (trois segments chaque année). Elles étaient apparamment en bonne santé selon une évaluation clinique sans aucune histoire de la jaunisse ou de la maladie du foie. Elles avaient les niveaux normaux des enzymes du fonctionnement du foie (TGPS, TGOS et TGG). Les échantillons de sang à jeun ont été collectés le moment de l'admission pour détecter les anticorps anti-HBS comme marqueur de l'hépatite virale B (HVB) ultérieure et l'antigène HBS pour diagnostiquer l'état de porteur chronique. Les enzymes du foie ont été mesurés après le 6ème, 18ème 24ème, 30ème et 36ème mois d'utilisation et entre trois et six mois de l'enlèvement de l'implant. Sur les 187 sujets inscrits, 159, 83 et 33 ont terminé un, deux et trois ans de l'utilisation de l'Uniplant respectivement. Les niveaux moyens des TGPS, TGOS et TGG ont révélé de petites hausses significatives au bout de la première et deuxième année d'utilisation par rapport aux niveaux de pré-insertion. Au bout de la troisième année, les valeurs moyennes élevées de tous les enzymes ont baissé petit à petit et s'approchaient des niveaux de pre-insertion sans aucune différence significative. Le pourcentage des titres positifs des anti-corps anti-HBS causés par une infection asymptomatique ultérieure était de 23,3% (n = 41) alors que l'antigenéanémie positive HBS (ie état de porteur) était de 3,4% (n = 6). Dans les deux groupes des femmes les anti-corps positifs anti-HBS (n = 41) sans l'antigenéanémie et les anti-corps négatifs anti-HBS (n = 129) — les changements dans les niveaux moyens de tous les enzymes pendant l'utilisation de l'Uniplant étaient très similaires sans aucune signification statistique. Les résultats ont montré que (1) L'Uniplant a provoqué quelques petites hausses à l'égard des niveaux moyens des TGPS, TGOS et TGG. Ces hausses étaient dans les limites normales, complètement réversibles et d'une signification clinique douteuse. (2) Les femmes non-porteuses qui ont été exposées à l'infection HVB asympomatique ultérieure n'ont pas eu d'effets importants sur les enzymes du foie étudiés par rapport aux femmes normales pendant l'utilisation à long terme de l'Uniplant. (Rev Afr Santé Reprod 2005; 9[1]: 24-31 )
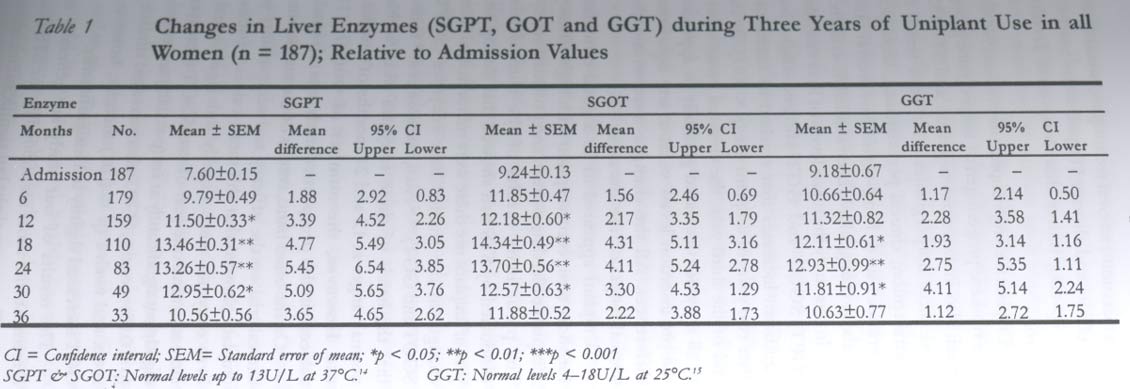
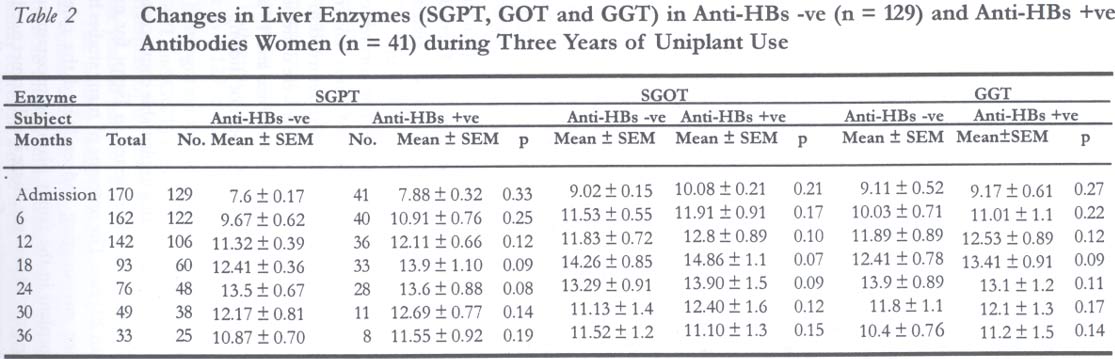
Key Words: Uniplant, liver, enzymes, antibodies Introduction Egypt is a developing country with endemic hepatic problems resulting from prevalent viral hepatic infections on one hand and endemic schistosomiasis on the other hand. Previous studies on Egyptian Norplant users showed little effects on liver functions,1 but some women with clinical and biochemical evidences of cure from hepatitis B and C infection adversely interacted with this progestin only method.2 Also, Egyptian women who experienced hepatitis in the past had significant and progressive increase in liver function tests during short-term use of combined oral contraception.3 Progress with Norplant implants has set a stage for the development of "second generation" contraceptive implants. The primary goals are (1) reduction in the number of implants, which facilitates insertion and removal, and (2) development of several new steroids with better pharmacological profiles.3 Uniplant had been tested in a single 35mm capsule with effective life span of one year. The progestogen (nomegestrol acetate) was released at the rate of 100µg/day during the first three months of use, which declined to 70µg during the last nine months. It provided a satisfactory pregnancy protection for one year in the volunteered women.5 Nomegestrol acetate (NOM-Ac) is a 19-norprogesterone derivative [3,20-oxo-6-methyl-17 á-acetoxy-19-norpregna-4, 6-diene].6 It is an orally active progestogen7 devoid of mineralo-corticoid activity8 and characterised by strong anti-estrogenic and anti-androgenic properties.9 It has been widely used in Europe as an oral progestin for more than ten years.10 NOM-Ac is synthesised by laboratoire Théraméx, Monaco, France. The South-to-South Cooperation in Reproductive Health (STS) had studied the contraceptive efficacy in 10 centres from nine countries worldwide. A total of 1803 volunteers were enrolled with over 20,000 woman-months of use. During one-year follow-up, both haematological and biochemical profiles (liver function tests - lipid and carbohydrate metabolism) showed minor but sometimes significant changes with all mean values within normal limits at six and twelve months of use.11-12 Although the study was conducted for three years continuously, the final report presented the results of one-year follow-up.13 The present work is aimed (1) to study the possible effects of long-term use (three years) of uniplant implant on some liver function enzymes (SGPT, SGOT and GGT) among women who are clinically and biochemically normal; (2) to study the percentage of seropositivity due to past asymptomatic infection with hepatitis-B virus among users; and (3) to evaluate whether this could predispose to any changes in these liver enzymes. Materials and Methods Subject Selection According to the proposed protocol of the multicentre study of the STS, 187 women were recruited from among attendees of the family planning clinic of Assiut University Hospitals, Egypt. They were allocated to use uniplant implant for three years continuously. Uniplant is designed for one year of use; so it was replaced by the end of the first and second years. On admission, a complete medical history was taken, including contraceptive history. Both routine physical and gynaecological examinations were carried out. All the women were apparently healthy at clinical assessment, they had no history of jaundice or liver diseases at reproductive age (>18-<38 years), multiparous (>3 living), had regular cycles during the last 3-6 months, did not use hormonal contraception during this period, and were not lactating. They accepted to participate in the study and to be followed up clinically and biochemically every six months during implant use, and one time 3-6 months after removal. The local ethical committee approved the study. From each woman, a 5ml venous blood sample was collected after overnight fasting. Standard liver function tests were done, including serum glutamate-pyruvate transaminase (SGPT), glutamate-oxaloacetate transaminase (SGOT) and gamma glutamyl transferase (GGT). Out of 187 women included in the study, 176 accepted to carry out serological tests for diagnosis of asymptomatic hepatitis B virus (HBV) infection. These serological tests included antibodies to HBV surface antigen (anti-HBs) as a marker for past asymptomatic infection, and HBV surface antigen (HBsAg) as a marker for a chronic carrier state. All of the women had no risk factors for HBV infection such as clinical schistosomiasis, blood transfusion, previous surgery or chronic parenteral therapy. Uniplant Description The uniplant implant is hand-made from medical grade dimethyl-polysiloxane (silastic) tubing (Tower Daul Peel®tubing), Dow Corning Corporation, Midland, USA. Each implant measured 39mm of total length (35mm of filled length) and 2.4mm diameter. It was filled with 55mg (±10%) crystalline, finely ground NOM-Ac.5 Insertion-Removal Techniques Insertion was done during the first five days of the menstrual cycle. Under local anaesthesia the skin of the left upper arm was incised 3mm length with a scalpel. The uniplant was placed subdermally by an 11-gauge trocar and cannula using withdrawal technique. Removal was preceded by local anaesthesia, and then through a 3mm incision, a mosquito forceps was introduced to grasp the implant within its fibrous sheath. Following incising its sheath, the implant was pulled out of the incision. Liver Function Tests (SGPT, SGOT & GGT) These were measured using kits prepared and distributed by Boehringer Mannheim GmbH Diagnostica, Germany (test combination, calorimetric method, cat. no. 125881, 125903 & 123889). Serum samples were used for all assays, and quality control was adjusted using normal (precinorm) and pathological (precipath) sera for the same procedure.14-15 The reference values of the assayed liver enzymes are written below each table. Hepatitis B Virus Markers For antibodies to HBV surface antigen (Anti-HBs) and HBV surface antigen (HBsAg), all the methods used for qualitative and quantitative determination were based on a direct, non-competitive (sandwich) assay based on ELISA technique using kits prepared by Enzygnost (Anti-HBs), Behrigwerke, AG, Marburg, Germany and Sorin Biomedica (HbsAg), Diagnostic Divison Saluggia, Italy, respectively. Statistics This was a longitudinal uncontrolled study in which each subject was used as her own self-control. Continuous variables comparing between follow-up visits or groups were presented as mean, ±SEM and confidence interval (CI). Since the data were non-parametric, statistical significance was examined using Wilcox on test for paired data and Mann-Whitney test for non-paired data. Results The socio-demographic and clinical characteristics of the studied women show that majority of them were living in rural areas (58.29%), were illiterates (59.91%), housewives (79.67%), while 88.8% of them did not use any method of contraception since last pregnancy. Their mean age was 29.6±5.1 SD years, mean of parity was 4.8±1.9 SD and the mean body weight was 60.8±12.9 SD Kg (data not shown). Table 1 presents the changes in liver enzymes (SGPT, SGOT & GGT) of all women during three years of uniplant use. Out of 187 women enrolled, 159, 83 and 33 had completed one, two and three years of use respectively. The mean levels of SGPT, SGOT and GGT showed slight but significant elevations at the end of the first and second years of use, compared to the pre-insertion levels. The p values were < 0.05 and < 0.01 respectively. However, the values were within the normal ranges of the enzymes measured. By the end of the third year, elevated mean values of all enzymes decreased gradually to approach the pre-insertion levels without any significant differences. From a total of 187 women enrolled, 176 accepted to carry out the serological markers for HBV to diagnose past asymptomatic infection. Six women (3.4%) had HBsAg positive titres, which signify a chronic carrier state, and they were advised to discontinue uniplant use. On the other hand, the percentage of women with anti-HBs antibodies positive titres was 23.3% (41 out of 176), which just signifies a past asymptomatic infection without chronicity, i.e., non-carrier. Table 2 shows a comparison between the changes in the studied liver enzymes in women with anti-HBs antibodies negative (n = 129) and those with anti-HBs antibodies positive (n = 41). The changes in the mean levels of all enzymes were closely similar in both groups. There were just minor differences without any statistical significance at all months of follow-up. Three to six months after implants removal, the elevated mean levels of these enzymes ((SGPT, SGOT & GGT) were returned to the pre-insertion values; these tests were done on 61 available blood samples (48 normal and 13 anti-HBs antibodies positive) (data not shown). Discussion The use of long-acting implantable contraceptives (Norplant) had been tested in Egypt for more than 20 years. The outcome of many studies have been encouraging and endorsed the role of Norplant in the family planning programme of Egypt.16-18 However, there is still unmet need for a new generation of contraceptive implants with easier insertion-removal techniques, possibly less side effects and shorter lifespan to be used for birth spacing rather than long-term fertility control. Uniplant is a single implant that releases NOM-Ac, a synthetic progestogen of norpregnane group, which also includes promegeston and ST-1435. These three norpregnanes have been tested in contraception, clinical performance, biological tolerance, and long-term hormonal and metabolic changes have been studied in women.19 In this study the mean levels of liver enzymes SGPT, SGOT and GGT showed slight but significant increases that reached its maximum after two years of uniplant use (p < 0.01). By the end of the third year, the elevated mean values of all enzymes decreased gradually to approach the pre-insertion levels without any significant differences. All the changes were within the normal ranges of the kits used. Uniplant appeared to be a good candidate for short-term contraception with high efficacy, acceptable bleeding pattern and potential safety.5 The preliminary results of the clinical trial conducted by STS had showed that during one year of uniplant use there were minor insignificant changes in the studied liver enzymes (SGPT, SGOT and GGT).11,12 Also, Barbosa et al20 found that the levels of these enzymes were within normal ranges at 12 and 24 months of uniplant use. However, the number of women (18 subjects) in this prospective study was too small. On the other hand, results of the multicentre clinical trial on the efficacy and acceptability of uniplant showed that the mean values of some liver enzymes were slightly but significantly increased after one year of use. SGOT increased slightly but significantly at six (p < 0.01) and twelve (p < 0.05) months, SGPT also increased similarly at six and twelve (p < 0.01) months; however, GGT increased slightly but insignificantly.13 The results of our study are generally in agreement with those mentioned by the STS final report. There were slight but significant increases in the mean values of liver enzymes, which were within the normal ranges at 12 and 24 months of uniplant use. However, a few points should be considered to explain such contrasts from different reports. The differences in the results may have been due to the differences in population, which suggests that dietary, genetic or other factors could influence drug metabolism and side effects. Previous studies show that the clinical performance experienced by Norplant users in Latin America was reversed among Chinese women.21 Also, experience with uniplant in other communities is not entirely relevant for our women, since their liver problems have different aetiologies. It can be generalised that in Egypt, alcohol, drug addiction and smoking can be excluded as strong a etiologic factors, while a state of malnutrition, endemic schistosomiasis and water-food pollution are not uncommon. Clinical observation indicated that many of these factors would develop progressive sub-clinical hepatic impairment and intolerance to progestin-only methods.2 Moreover, the studies show that in Egypt, seroprevalence of anti-HCV antibodies in blood donors are more than ten times greater than in western populations,22 which could increase intolerance to hormonal contraceptives and may necessitate serological screening before their use. We found that three to six months after implant removal elevations in the mean values of liver enzymes were not detectable, which possibly reflects a state of transient reversible changes. It is known that serum levels of SGPT and SGOT should be increased three times the upper limit of normal in order to suspect a mild hepatic impairment. 23 Thus, we may speculate that the slight elevations of the mean levels of these enzymes might be of just statistical significance rather than being of clinical importance; yet it could be of potential health concern that necessitates periodic check-up during long-term use of uniplant. Unfortunately, clinical studies show that HBV is now hyper-endemic all over Egypt.24-25 The causes of this hyper-endemicity are not clear; parenteral anti-schistosomal therapy had been shown as a potential risk factor for HBV infection. Other potential risk factors included history of circumcision and parenteral immunization.26 Findings from this study confirmed this fact, as the percentage of anti-HBs antibodies (due to past asymptomatic infection) among our women, who were clinically and biochemically normal, was 23.3%. In Assiut, Shaaban27 reported an incidence of nearly 20% among our people. Previous studies reported that the seroprevalence of anti-HBs antibodies among the Egyptian adult population due to past asymptomatic infection ranges from 30% to 60%.24-28 Literature contains very limited data on the safety of long-acting progestin-only methods among women with serological markers of past hepatitis BV infection. Among our women it was found that those with clinical and biochemical evidence of cure from clinical viral hepatitis B and C were still having some residual abnormalities in liver cells that adversely interacted with Norplant. It was concluded that Norplant was not well tolerated by women with previous clinical hepatitis infection, particularly those with persistent antigenaemia.2 In the present work, 41 women (23.3%) had anti-HBs antibodies positive titres due to past asymptomatic infection with HBV and without antigenaemia (HBsAg -ve); all of them were normal on clinical and biochemical assessment. In both groups of women [anti-HBs antibodies -ve (n = 129) and anti-HBs antibodies +ve (n = 41)] changes in the studied liver enzymes (SGPT, SGOT and GGT) were closely similar to minor differences of no statistical significance during three years of uniplant use. This finding could be associated to the fact that women with past asymptomatic hepatitis BV infection without antigenaemia (non-carriers) possibly represent a mild form of infection with minimal residual effects on liver functions even during long-term exposure to nomegestrol acetate. Also, this could reflect potential safety of uniplant, which has been proved in some medical disorders, such as in sickle cell patients.29 Finally, we would conclude as follows: (1) Uniplant induced slight but significant elevations in the mean levels of SGPT, SGOT and GGT. These elevations were within the normal range, completely reversible and of doubtful clinical significance. (2) The non-carrier women who had been exposed to past asymptomatic HBV infection showed no significant effects on their studied liver enzymes, compared to the normal women during long-term use of uniplant. Acknowledgments The authors gratefully acknowledge the efforts of Professor Elsimar M. Coutinho, coordinator of the uniplant multicentre study and Professor Oladapo A. Ladipo, executive secretary and programme manager, South-to-South Coopera-tion in Reproductive Health, Salvador, Bahia, Brazil. The Rockefeller Foundation, under the South-to-South programme, supported this study. References
© Women's Health and Action Research Centre 2005 |

{kind=link}
{kind=link}