 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 9, No. 1, April, 2005 pp. 49-65 Parental Factors and Sexual Risk-Taking among Young People in Côte d'Ivoire Stella Babalola1, B Oleko Tambashe2 and Claudia Vondrasek1 1Johns Hopkins University, Bloomberg School
of Public Health, Center for Communication Programs, Baltimore, Maryland. 2Tulane
University, Payson Center for International Development and Technology Transfer,
New Orleans, Louisiana. Code Number: rh05008 Abstract Côte d'Ivoire is the country worst affected by the HIV epidemic in West Africa, and young people in this country are a particularly vulnerable group. This study examined the relation between parental factors and sexual risk-taking among young people using logistic regression and survival analysis methods. Three parental factors (living in the same household as the father during childhood, perceived parental disapproval of early and premarital pregnancy, and parent-child communication about sexual abstinence) were positively associated with primary sexual abstinence (defined as yet to experience sexual debut), secondary sexual abstinence (defined as sexual abstinence subsequent to sexual debut) and reduced number of sex partners. The findings suggest that parental monitoring and control are important predictors of youth sexual behaviours and underscore the need to target parents and guardians in efforts to promote responsible sexual behaviours among adolescents. It is important to promote parent-child communication about sexual issues and empower parents and guardians to communicate effectively with their children and wards about sexual issues. (Afr J Reprod Health 2005; 9[1]: 49-65) Résumé Facteurs parentaux et la prise de risque sexuel chez les jeunes gens en Côte-d'lvoire. La Côte-d'lvoire est le pays le plus atteint par l'épidémie du VIH en Afrique de l'ouest et les jeunes gens de ce pays constituent un groupe surtout vulnérable. Cette étude a examiné le rapport entre les facteurs parentaux et la prise de risque sexuel chez les jeunes gens à l'aide de la regression logistique et la méthode de l'analyse de survie. Trois facteurs parentaux (le fait d'habiter dans la mème maison que le père pendant l'enfance, la désapprobation parentale perçue de la grossesse précoce et la grossesse prémaritale et la communication parent-enfant concernant l'abstinence sexuelle primaire (définie comme n'ayant pas encore eu l'expérience sexuelle), l'abstinence sexuelle secondarie (définie comme une abstinence sexuelle postérieure à l'expérience sexuelle initiale) et le nombre réduit de partenaires sexuels. Les résultats démontrent que la surveillance et l'autorité des parents sont des facteurs importants qui soulignent le besoin de viser les parents et les tuteurs dans les tentatives de promouvoir des comportements sexuels responsables chez les adolescents. Il est important de promouvoir la communication parent-enfant par rapport aux questions sexuelles et de capabiliser les parents et les tuteurs afin qu'ils puissent communiquer de manière effetive avec leurs enfants et leurs pupilles quant aux questions sexuelles.(Rev Afr Santé Reprod 2005; 9[1]: 49-65) Key Words: Parent, attitude, communication, sex, behaviours, Cote d'Ivoire Introduction After decades of relative peace, Côte d'Ivoire is currently experiencing one of the worst periods of political upheavals and economic downturn in its history. Inflation and rising unemployment further compound the problems of widespread insecurity and social unrest.1 Efforts aimed at achieving a vibrant, peaceful and sustainable society are undermined by the rising HIV/AIDS epidemic. With an estimated national adult infection rate of 10.8%, Côte d'Ivoire is the country worst affected by the HIV epidemic in West Africa.2 AIDS now ranks second among the leading causes of death in the country, and about one million of the 16 million Ivorians are estimated to be living with HIV/AIDS. Recent data on HIV prevalence indicate that youth are a particularly vulnerable group, with females being more at risk than males. According to the UNAIDS estimates for 2001, between 6.7% and 10% of female youth aged 15-24 years are seropositive compared to only 2.5-3.5% of their male counterparts.3 There is considerable evidence that many Ivorian youth engage in sexual behaviours that expose them to the risk of HIV infection. For example, the 1998 Demographic and Health Survey (DHS) found that the median age at first sexual intercourse was 16.5 years for males and 17.1 years for females.4 The same survey found that 56% of male and 61% of female youth had sex during the last 12 months. Multiple sexual partnership was also a relatively common practice with 49% of sexually experienced young men reporting multiple partnership during the last 12 months.4 Condom use was also very low.5,6 Premarital risky sexual behaviours are a cause for concern because they expose young people to HIV infection and they are significant predictors of sexual behaviours later in life. A number of studies have documented a correlation between premarital sexual behaviour and extramarital intercourse. For example, in their multi-country study, White et al found that in Côte d'Ivoire, the odds of engaging in extramarital sex increased with the number of sexual partners before marriage and decreased with age at sexual debut.7 Moreover, considering that young people represent a significant proportion of the population, efforts to curb the spread of the infection and prevent a generalised epidemic should focus on this age group as a key audience. An appropriate approach to effective HIV prevention involves identifying and addressing the potentially modifiable factors that affect sexual behaviours and susceptibility to HIV infection among youth. There is a growing body of literature on the links between parental factors and adolescent sexual attitudes and behaviours. Existing literature, mostly from the West, provide equivocal evidence regarding the importance of parental factors relative to other environmental influences on youth sexual risk-taking. Some developmental researchers, reflecting the behaviour genetic school of thought, argue that much of the influence attributed to parental attitudes and behaviours might in fact be due to genetic factors.8-10 Others have argued that parental influence declines steadily as the child moves into late adolescence and as young people become increasingly exposed to peer influences, poverty and other environmental factors.11,12 In contrast, researchers from the socialisation theoretical perspective assert that parental factors have considerable independent influence on youth risk-taking, and that such influence remains very strong during adolescence.13-16 Other studies have even suggested that parental attitudes and behaviours tend to mediate the potential effects of genes or peers.17-19 Traditionally, studies examining the link between young people's sexuality and parental factors have focused on parent-child communication, parent-child closeness, parental monitoring and discipline (behavioural control), and perceived parental attitudes. Other studies have examined living arrangements, with either or both parents, and parental socio-demographic characteristics such as level of education, income and marital status. Parent-child communication is the parental factor most often linked to adolescent sexual attitudes and behaviours. While there is evidence that teenagers prefer to receive information about sexuality from their parents, in reality few have this privilege.20-24 Nonetheless, research has documented that the quantity, frequency and timing of parent-child communication are important factors in sexual outcomes, including knowledge about sexuality and reproductive health, sexual attitudes and sexual behaviours and intentions.25-29 It is important to mention that a few studies have documented that parent-child communication is associated with greater sexual behaviour among youth.30 However, in such studies it is not clear which comes first, the onset of sexual behaviour or the onset of parental attempts to educate adolescents about sexuality. Strong behavioural control (parental monitoring and discipline) is increasingly recognised as an appropriate strategy to deter adolescents from engaging in risky behaviours including unsafe sexual practices.31,32 It is pertinent to note that the link between parental monitoring/supervision and adolescent sexual behaviours may also be curvilinear. Indeed, there is evidence that too much behavioural control may have a negative effect on adolescent sexual behaviour, just as too little control does.33 A few studies have examined actual or perceived parental attitudes and behaviours and found indications that these variables are related to the sexual attitudes and behaviours of youth. In general, these studies have found that parental disapproval of teen sex is associated with late sexual debut, reduced number of sexual partners, infrequent sex and decreased teen pregnancy among youth.34,35 Studies that explored the link between living arrangements in terms of the presence of one or both parents in the same household as the adolescent have also yielded consistent results. Having been raised by both parents is associated with reduced sexual risk-taking among adolescents, while living in single-parent families is associated with increased levels of adolescent sexual risk-taking in Western countries.36,37 Similarly, a few studies have found that parental survival status and living in the same household as the father are closely linked to adolescent early sexual experimentation in African countries.38,39 Inadequate supervision and support for material needs may explain these relationships. In sum, existing literature overwhelmingly underscores the need to address parental factors in efforts aimed at promoting safe sexual practices among adolescents. Given that few of the existing studies focus on sub-Saharan Africa, studies that examine the dynamics of parental factors in adolescent sexual risk-taking in African countries are clearly indicated. Methods Study Participants The data used in this paper derive from a 2001 survey among youth aged 15-24 years in three cities in Côte d'Ivoire, namely, Abidjan, Korhogo and Bouake. Having previously determined the required sample size based on the proportion of sexually active youth that use condoms, the survey respondents were selected through a multiple-stage random process that involved selecting first enumeration areas (EAs) and then households within the selected EAs. With the assistance of the Institut National de la Statistisque in Côte d'Ivoire, the research agency randomly selected a number of EAs from each study city proportionate to the population size in the city. In each of the selected EAs, all the households were listed and 40 of them randomly selected for participation in the survey. All the young people aged 15-24 years in the selected households were targeted for interview. A total of 2,681 persons (1,262 males and 1,419 females) were successfully interviewed during the survey. Measures Criterion variables This study examined three criterion variables: 1. Age at sexual debut: This variable was derived from two questions in the survey tool. First, we asked if the respondents had ever had sexual intercourse, and those who had were asked to specify the age at which they had their first sexual experience. 2. Sexual abstinence during the past six months. We derived this indicator of secondary sexual abstinence from the question that asked sexually experienced respondents to specify how long ago they had sex. 3. Having had sex with more than one sexual partner in the past three months. This variable was used to measure the prevalence of multiple sexual partnerships and was derived from the question on the number of sexual partners. Predictor variables An extended ideation model served as the framework for the analyses. The ideation model is an analytic psychosocial model that has its genesis in demographic literature. As a concept, ideation has been defined as ways of thinking that can be diffused through communication and social interactions.39-43 It is a predictive model that incorporates behavioural predictors borrowed from leading psychosocial theories. The original ideation model has been extended for the purpose of our analysis to include parental factors, in addition to the individual factors. The predictor variables in the estimated Cox and logistic regression models are: 1. Parental factors: Three variables were used to measure parental influence:
2. Ideational variables: Five categories of ideational variables were included in the estimated models:
3. Socio-demographic variables: The estimated models also contain socio-demographic predictor variables including:
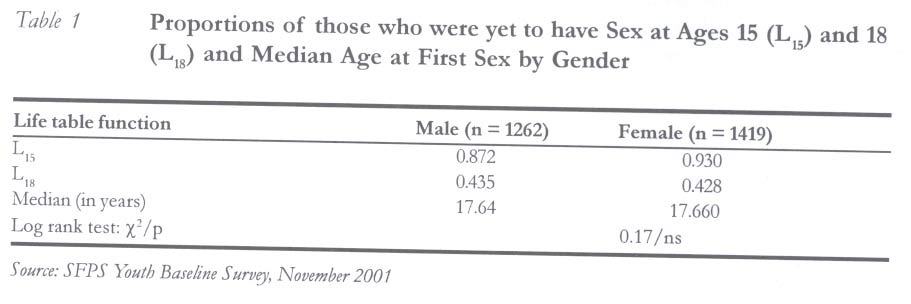
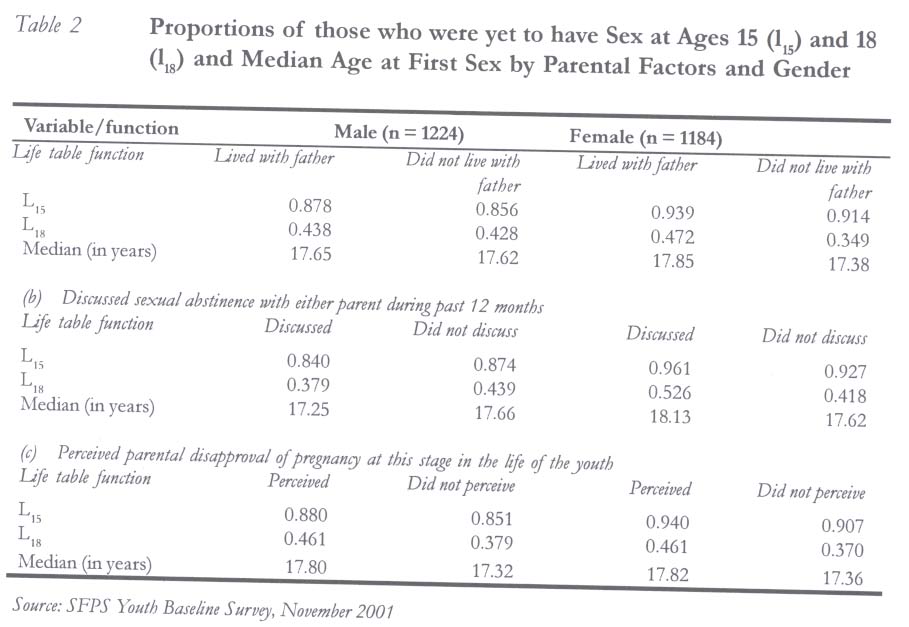
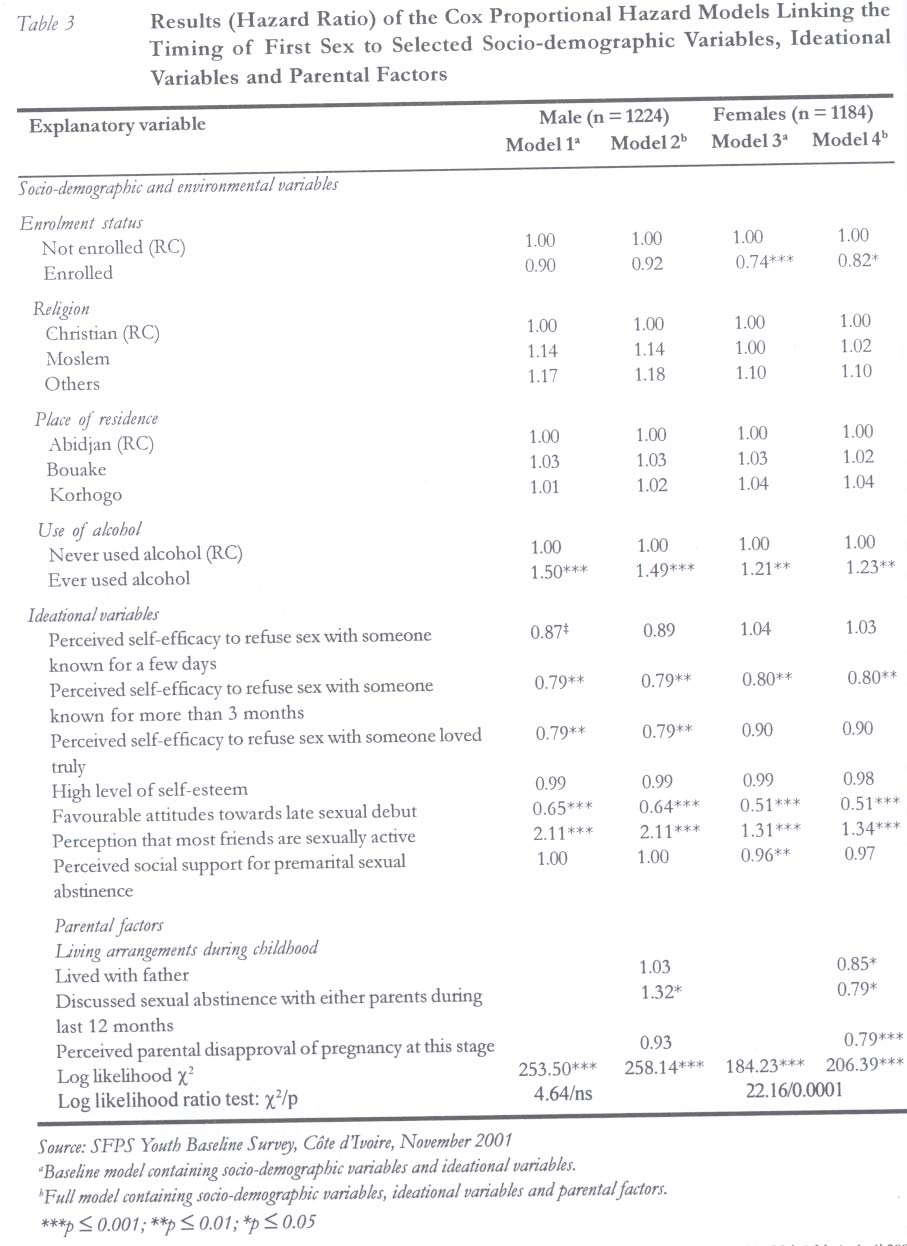
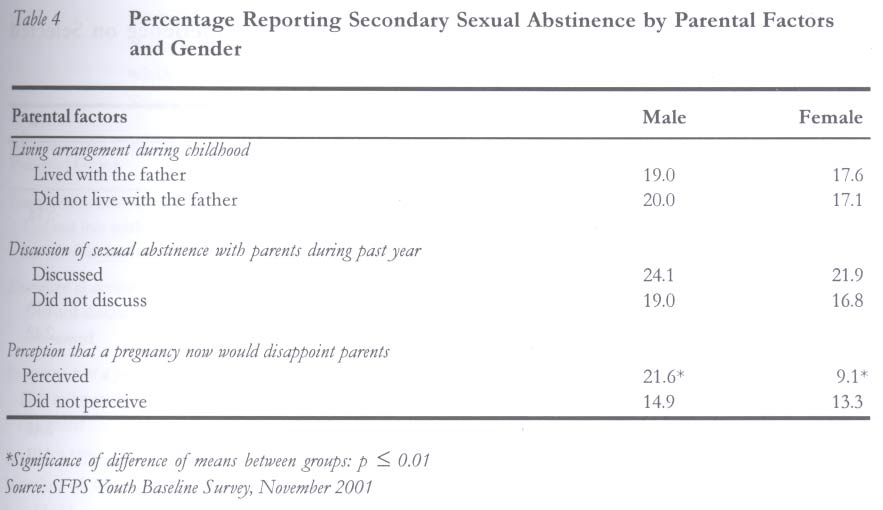
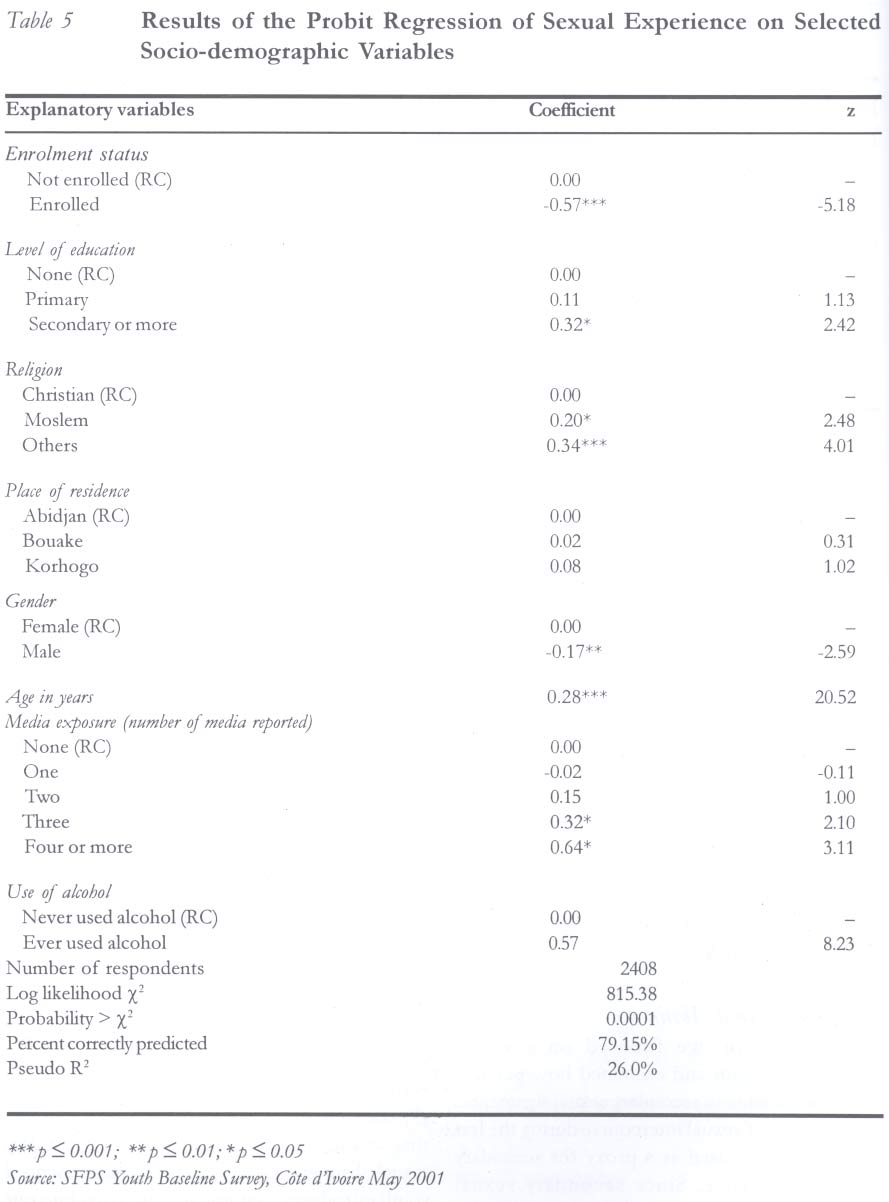
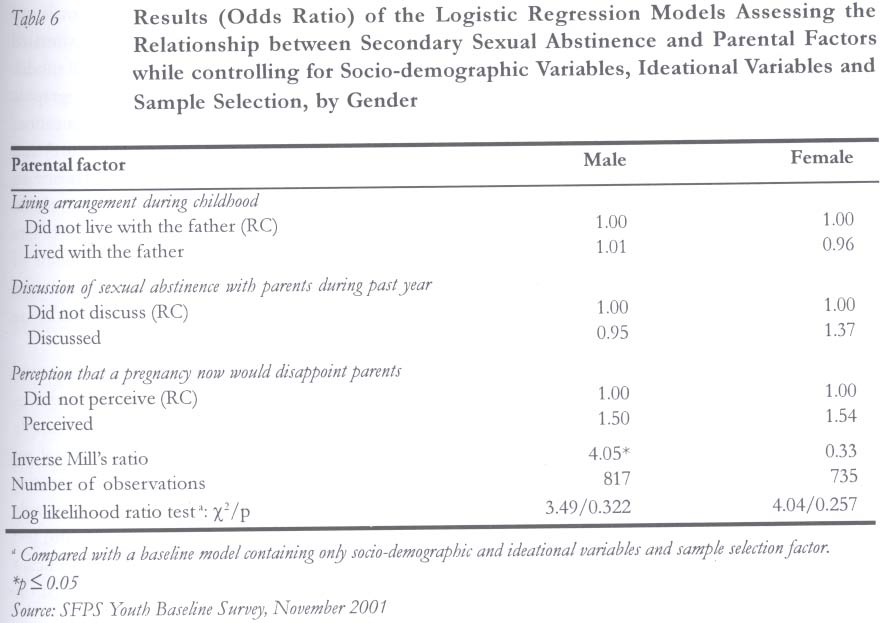
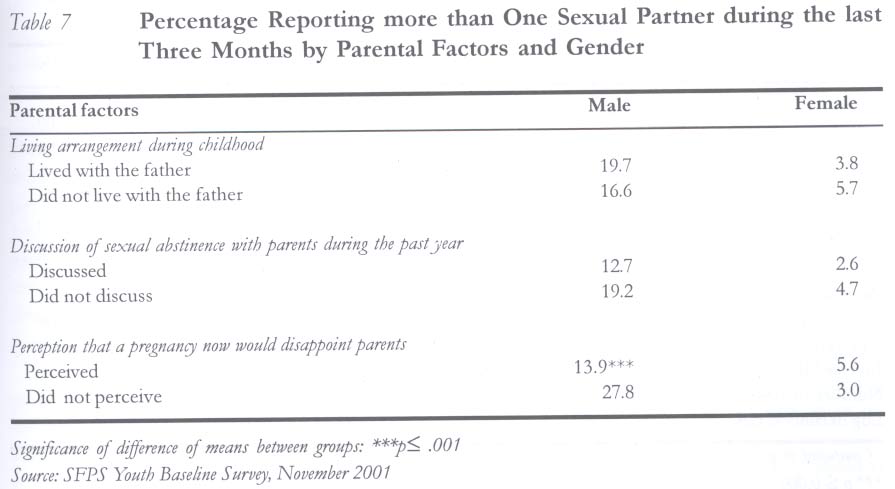
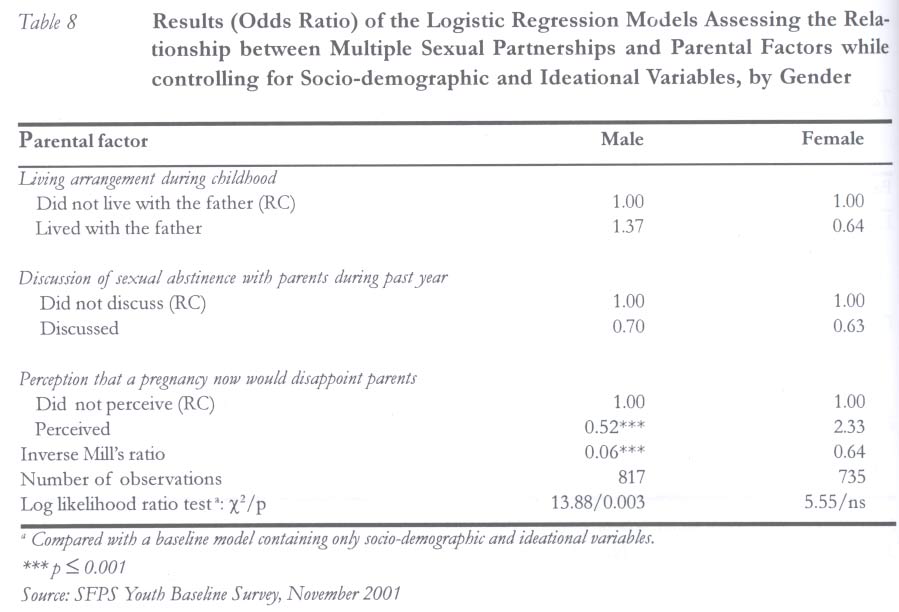
Analytical Procedures We used survival analysis methods, life table analysis and Cox proportional hazards method to identify the effects of parental factors on the timing of first sex. For many reasons, survival analytical techniques are the best indicated methods for event-history data that measure the length of time until the occurrence of an event such as age at first sex. First, in societies characterised by late sexual debut, the median age at first sex may be beyond the focal age group. Among young people, data concerning sexual debut may be considerably skewed towards sexual inexperience. In this case, the use of standard bivariate or logistic regression methods to analyse current status data (in terms of whether respondents have or have not experienced sex) may result in considerably biased estimates. Second, since the phenomenon under study is the time to an event, it is possible that the event has yet to occur by the time the survey takes place. This phenomenon is known as observation censoring. Data on the age at first sex are right-censored because not all the respondents have experienced the phenomenon under study before the survey took place. The best way to analyse such data is to distinguish between which responses (age at first sex) are observed event times and which ones are censored times. In survival analysis, a variable is introduced to reflect this distinction. In the present analyses, respondents who had had sex were considered to have experienced the failure event at their age at first sex, whereas those who were yet to experience the event were censored at their current age. Using the Kaplan-Meier life table method, we estimated the proportion surviving (that is, yet to experience first sex) at each age.48,49 In the preliminary step of the analyses, we focused on all respondents, whether married or not, to establish the overall pattern of the timing of first sex among males and females. We then used the log-rank test to assess the differences by parental factors. To assess the net relationship between the age at first sex and parental factors while adjusting for the confounding effects of selected socio-demographic and ideational variables, we used Cox proportional hazards model.50 The Cox model is a semi-parametric model that has a unique advantage of allowing the inclusion of covariates and, therefore, makes it possible to assess the effects of a specific predictor variable while holding other predictors constant. The model is based on the assumption that changes in the levels of the predictor variables will produce proportionate changes in the hazard function, independent of time. Since the indicators for secondary sexual abstinence and multiple sexual partnerships are defined as dichotomous (indicator) variables, we used logistic regression to assess their relationships with parental factors. Results Timing of Sexual Debut Data show that majority of the respondents had experienced sexual debut in their teens (Table 1). There was no significant difference in the timing of first sex by gender as shown by the results of the log-rank test for equality of survival functions. The life table proportion that was yet to experience sex at age 18 was slightly over two-fifths for either gender and the median age at first sex was about 17.6 years. In the next few paragraphs, we look at the variations in the timing of sexual debut by parental factors, starting with the bivariate relationships shown by the life table results (Table 2) and, subsequently, examining the results of the Cox Proportional Hazards models. Life Table Analysis Results More than two thirds (68.4%) of the respondents lived in the same household as their father during childhood. For some unclear reasons, males (71.3%) were more likely than females (65.5%) to reside in the same household as their father (z = 3.21, p < 0.001). The relationship between childhood living arrangements and the timing of sexual debut differed by gender. Data on the males did not show the predicted negative relationship and observed differences were not statistically significant. In contrast, among females, living with the father during childhood was significantly associated with increased age at sexual debut (log rank test χ2 = 20.72, p< 0.001). Discussion about sexual abstinence with either mother or father during the previous 12 months was used as a proxy for parent-child communication about sex. Very few (7.6%) of the respondents reported that they discussed sexual abstinence with either parent during the previous 12 months. Among males, the relationship between discussion about sex with parents and the timing of sexual debut was statistically significant (log rank test χ2 = 4.32, p < 0.05) but not in the expected direction. Parent-child communication about sex was associated with earlier sexual debut among boys. Among girls, the relationship was statistically significant (log rank test χ2 = 10.68, p< 0.001) and in the expected direction. The life table median age at sexual debut was higher by about 0.5 year among girls who reported discussion about sexual abstinence with their parents. As expected, perceived parental disapproval of pregnancy at the current stage in the life of the youth varied by age of the respondent. While 80% of respondents aged 15-19 years reported that a pregnancy at this stage of their lives would disappoint their parents, only 61% of those aged 20-24 years did. The data show that parental disapproval of pregnancy is strongly associated with delayed sexual debut among both male (log rank test χ2 = 15.6, p < 0.001) and female (log rank test χ2 = 38.3, p < 0.001) respondents. Cox Proportional Hazards Results In order to assess the net relationships between parental factors and the timing of sexual debut, we estimated a set of Cox proportional hazards models that control for the confounding influences of selected socio-demographic and ideational variables. We estimated separate models for males and females and the results are provided in Table 3. The data show that, after controlling for socio-demographic and ideational variables that have been empirically demonstrated to influence sexual activity, parental factors are strong predictors of the timing of sexual debut among females. Jointly, the parental variables contributed significantly to explain the timing of first sexual intercourse. The introduction of parental variables in Model 4 resulted in a significant increase in the explanatory power of the estimated model as the results of the log-likelihood ratio test show. Moreover, each of the parental variables was significant in predicting the timing of sexual debut. The perceived parental disapproval of a pregnancy at the present stage of the respondent's life was the most significant of the three variables. The data show that, at a given time, the female respondents who perceived parental disapproval of pregnancies and who had not yet experienced sex had a 21% decreased risk of experiencing sex compared to their peers who did not hold this perception. In addition to parental factors, other variables that were associated with delayed sexual debut among females were perceived self-efficacy to refuse sex with someone loved truly, favourable attitudes towards late sexual debut and school enrolment. In contrast, alcohol consumption and the perception that most friends are sexually active favoured early sexual experimentation. The story was different among males in relation to the role of parental factors. The results of the log-likelihood ratio test showed that taken jointly, parental factors did not contribute meaningfully to predicting the timing of the first sex. The only parental variable that had a noticeable link with the timing of sexual debut was discussion about sexual abstinence with parents and, unexpectedly, the direction of the relationship was positive. This finding strengthens the suggestion made earlier that parents tend to talk to their sons about sex only after they notice signs of sexual activity among them. Other strong predictors of the timing of sexual debut among males included alcohol consumption, perceived sexual behaviours of friends and attitudes towards late sexual debut. The perceived self-efficacy to refuse sex with someone known for more than three months and the perceived self-efficacy to refuse sex with someone loved were also strong predictors of the onset of sexual activity among males. Secondary Sexual Abstinence In this section, we focused on sexually experienced youth and examined how parental factors are related to secondary sexual abstinence. The absence of sexual intercourse during the last six months was used as a proxy for secondary sexual abstinence. Since secondary sexual abstinence was not relevant for married youth, the analyses in this section were limited to never-married youth. Overall, less than one fifth (19.3%) of sexually experienced never-married males and 17.3% of their female counterparts reported that they did not have sex during the last three months. Variations in the prevalence of secondary sexual abstinence by parental factors are shown in Table 4. The data suggest that residence with the father during childhood makes no difference in current secondary sexual abstinence. For example, of the males who lived with their father during childhood, 19% reported secondary sexual abstinence, compared to 20% who did not live with their father. In contrast, the prevalence of secondary abstinence is higher among respondents that reported discussion about sexual abstinence with the parents during the past year. It is only possible to observe secondary sexual abstinence among sexually experienced youth, but our survey covered both sexually experienced and inexperienced youth. The fact that we did not have information on secondary sexual abstinence for the sexually inexperienced youth introduces a sample selection bias into our data, a situation that may result in inefficient estimates. To control for possible sample selection bias, we considered the youth's decision to have sex in our estimation of the linkages between parental factors and secondary sexual abstinence using the two-stage sample selection correction procedure suggested by Heckman.51 In the first stage of this procedure, we used probit regression to estimate sexual experience from a set of socio-demographic variables that are susceptible to influence the decision to have sex (Table 5). Using the probit results, we computed the non-selection hazard (inverse Mill's ratio) for each observation. In the second stage, we included the inverse Mill's ratio along with parental factors and other explanatory variables in the logistic regression model used to estimate the odds of reporting sexual abstinence. To ensure identification of the model, alcohol consumption, a variable that strongly predicted sexual experience but was not associated with secondary sexual abstinence, was excluded from the second model. Separate models were estimated for male and female respondents. For each sex, we estimated two models: a baseline model and a full model. The baseline model included socio-demographic variables (place of residence, religion, education, enrolment status, age and media exposure) and ideational variables (perceived self-efficacy to refuse sex, perceived social support for sexual abstinence, self-esteem, attitudes towards late sexual debut, and perceived sexual behavior of friends). The full model included the parental factors as well. The results of the full model are summarised in Table 6. The male data show that the estimated coefficient on the non-selection hazard was positive and significant, which would imply selection bias such that boys who were not yet sexually active were more prone to practice secondary abstinence should they become sexually active. The results of the log-likelihood ratio test indicate that parental factors are jointly insignificant in predicting secondary abstinence. None of the factors had any independent link to secondary abstinence. As for the female data, the coefficient associated with the non-selection hazard was positive but not significant; indicating that sample selection was not present. However, similar to what the male data indicate, parental factors were jointly insignificant in predicting secondary sexual abstinence among females. Multiple Sexual Partnerships In this section, the proportion that reported more than one sexual partner during the last three months was the dependant variable and was used as a proxy for the prevalence of multiple sexual partnership. The data showed that very few of the girls (4.5%) and a noticeable proportion of the boys (18.8%) reported more than one sexual partner during the past three months. The data further showed that adolescent males (14.0%) were significantly less likely to report multiple sexual partnership than their older counterparts (22.3%). In contrast, there was no difference between adolescent females (4%) and female young adults (5%). Looking at the bivariate results (Table 7), we found that among females, multiple sexual partnerships did not appear to vary noticeably by any of the parental factors considered. As for males, the only parental factor that appeared to have had the expected significant relationship with multiple sexual partnerships was the perceived parental disapproval of pregnancy. The proportion of males that reported multiple sexual partnerships was more than twice as high among respondents that did not perceive parental disapproval of pregnancy than among their peers that perceived disapproval. To assess the net relationships between parental factors and multiple sexual partnerships, we estimated various logistic regression models that corrected for sample selection as described in the previous section. We also estimated two models for each sex: a baseline model and a full model. The predictor variables in the estimated model were the same as in the previous section. For male youth, the coefficient associated with the indicator for sample selection was significant and negative. This again shows that selectivity is an issue among males and specifically indicates that male youth that choose to be sexually inactive are less prone to multiple sexual partnerships than any randomly selected male youth. The logistic regression results showed that parental factors were jointly significant predictors of multiple sexual partnerships although the only parental variable that was individually significant was the perceived parental disapproval of pregnancy (Table 7). The data showed that males who perceived parental disapproval for pregnancy at this stage in their lives were 48% less likely than their peers to engage in multiple sexual partnerships. (Table 8) As for the female data, the selectivity variable was not significant, indicating that sampling bias was not present in the data. Furthermore, for this group, the results of the logistic regression indicated that parental factors were not of importance in predicting multiple sexual partnerships. Discussion This study has examined the relationships between parental factors and sexual risk-taking among young people in Côte d'Ivoire. The results confirm that early sexual experimentation is the norm among young people: at age 18 years only about two fifths of either sex were yet to experience sexual debut. The data largely confirm what existing studies from developed countries have demonstrated and show that parental factors play some role in determining the sexual attitudes and behaviours of young people. In terms of the magnitude and direction of the relationships, the three parental factors considered have disparate influences on males compared to females. For example, living in the same household as the father during childhood was strongly associated with delayed sexual debut among females but not among males. This finding suggests the existence of a gender-based double sexual standard among parents and points to the need to target parents with messages aimed at promoting egalitarian treatment of male and female youth in sexual matters. There is need for appropriately designed communication interventions that address gender stereotypes among parents and engage them in promoting delayed sexual debut among both male and female children. The relationship between parent-child communication about sexual abstinence and the timing of sexual debut also differed by sex. The relationship was significant for both sexes; however, while it was negative among females it was positive among males. The finding that discussion about sexual abstinence with parents is associated with early sexual debut among males suggests that parents tend to talk to their sons about sex only after signs of sexual activity have become visible. It is also possible that parents tend to encourage their sons to engage in sexual intercourse. This finding has important programmatic implications. Appropriately designed strategic communication interventions should encourage parents to be proactive in initiating discussions about sex with their children, and in encouraging their children to delay sexual debut irrespective of the child's sex. It is parti-cularly important to encourage and empower parents to start to communicate with their children on sexual matters while the children are still in late childhood or early teenage years, before they become sexually active. In this regard, an effective communication intervention will be one that not only encourages and motivates parents to discuss sex with their children but actually trains them and provides them with the necessary tools to do so. It is important to mention that in Côte d'Ivoire, as in most of the other countries in the sub-region, parent-child communication about sex is not normative. Promoting parent-child communication about sex would, therefore, involve attempts to change social norms about parental role in the sexuality education of their children. Nonetheless, historical evidence has shown that while social norms are not easy to change, they are not static either. Changing the social norms about the role of parenting in adolescent sexuality education will require consistent and persistent interventions at multiple levels. Targeting individual level behaviour change alone cannot produce sustainable positive results. Effective interventions should go beyond psychosocial theories and draw on appropriate theories of structural and environmental change. In this regard, one pertinent theory is the empowerment model, which emphasises the need for empowerment at three levels: personal, organizational, and community. The data show that after controlling for confounding factors, parental attitudes towards a pregnancy made significant difference for the timing of sexual debut among females but not among males. This finding reinforces the need for parents to be consistent in denouncing early and premarital sexual activity with equal vigour among both male and female children. Parental factors were jointly insignificant in predicting secondary sexual abstinence. Although the data suggest that young people who perceived that their parents disapproved of premarital pregnancy were less likely to engage in frequent sexual intercourse, the relationship was only weakly significant. It is possible that when parents disapprove of early childbearing such attitude is typically not expressed strongly enough to discourage continued sexual activity among sexually experienced youth. The results of a positive deviance inquiry (PDI) conducted by JHU/CCP in Côte d'Ivoire as a prelude to the survey reported in this article show that pressure from parents is a threat to continued sexual abstinence in late teenage and young adulthood years. Indeed, the PDI results show that parents tend to encourage their late teenage and young adult children to become sexually active. This finding points to the need to educate parents on the threat of HIV and other STIs for youth and on methods of preventing the infection. In this way, should parents choose to encourage their children to become sexually active, they would at least be able to advice them on ways of preventing sexually transmitted infections. Taken jointly, parental factors were important in determining the practice of multiple sexual partnerships among male youth but not among their female counterparts. The absence of a strong linkage between parental factors and sexual behaviours among youth may be spurious and due to the fact that very few female respondents have had more than one sexual partner during the past three months. Among males, the only parental factor that strongly predicted multiple sexual partnerships among youth was perceived parental attitude towards early childbearing. Indeed, parental disapproval of early childbearing was a strong factor that appeared to discourage multiple sexual partnerships among male youth. This finding underscores the need to empower and encourage parents to continue providing positive role models and guidance to their sexually active children. Parents need to understand that their attitudes and behaviours matter for the sexual attitudes and behaviours of their children. In general, appropriately designed communi-cation programmes should encourage parents to be clear and unequivocal in making their values and beliefs about the timing of sexual debut, frequency of sexual intercourse and the number of sexual partners known to their children. Finally, while the data have clearly demon-strated that parental factors were strongly associated with the sexual behaviours of young people, the cross-sectional nature of the data makes it impossible to ascertain causation. Considering that parental attitudes and sexual behaviours of young people are choice variables, the observed relationships may be due to the effects of unobserved factors that influence both sets of variables. In other words, the parental factors considered in this paper (especially parental disapproval of pregnancy and discussion about abstinence) are probably endogenous to the sexual behaviours of young people. It is also possible that the observed relationships are due to reverse causation — sexual behaviours of young people prompting remedial parental attitudes and not vice versa. Cross-sectional data do not allow us to ascertain the extent to which endogeneity bias and reverse causation were relevant among the study population. Longitudinal data are necessary to understand the sequence of events in the life of a young person and ascertain the direction of causality between parental factors and the sexual behaviours of young people. Further research along this line is therefore indicated. Acknowledgments Tulane University and the Johns Hopkins University Center for Communication Programs (JHU/CCP) provided technical assistance to the Ivorian École Nationale Supérieure de Statistique et d'Économie Appliquée (ENSEA) in the design and implementation of the survey. The survey was conducted to provide baseline indicators for a youth sexuality project being implemented by the regional project, Santé Familiale et Prévention du SIDA (SFPS). Funding for the survey came from the United States Agency for International Development (USAID). References
© Women's Health and Action Research Centre 2005 The following images related to this document are available:Photo images[rh05008t8.jpg] [rh05008t3.jpg] [rh05008t7.jpg] [rh05008t5.jpg] [rh05008t2.jpg] [rh05008t1.jpg] [rh05008t6.jpg] [rh05008t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}