 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 9, No. 1, April, 2005 pp. 88-98 HIV and Sexually Transmitted Infections among Women Presenting at Urban Primary Health Care Clinics in Two Cities of sub-Saharan Africa
Elizabeth Mukuze Mbizvo1,2,3, Sia Msuya1,2,5, Akhtar Hussain1,2, Mike Chirenje3, Michael Mbizvo4, Noel Sam5 and Babill Stray-Pedersen2 1Department of Obstetrics and Gynaecology, The National Hospital,
University of Oslo N - 0027 Oslo, Norway. 2Institute of General
Practice and Community Medicine, Department of International Health, University
of Oslo, Postbox 1130, Blindern 0317, Oslo, Norway. 3Department
of Obstetrics and Gynaecology, University of Zimbabwe, P. O. Box A- 178,
Avondale, Harare, Zimbabwe. 4Department of Reproductive Health
and Research, World Health Organization, CH 1211 Geneva - 27, Switzerland. 5Kilimanjaro
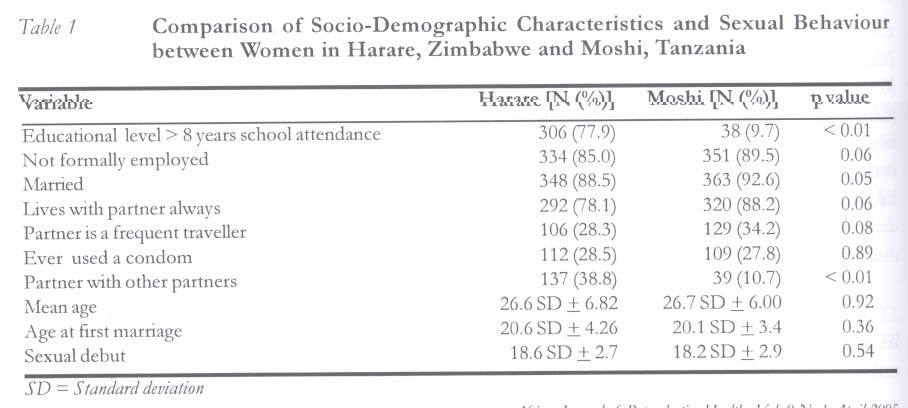
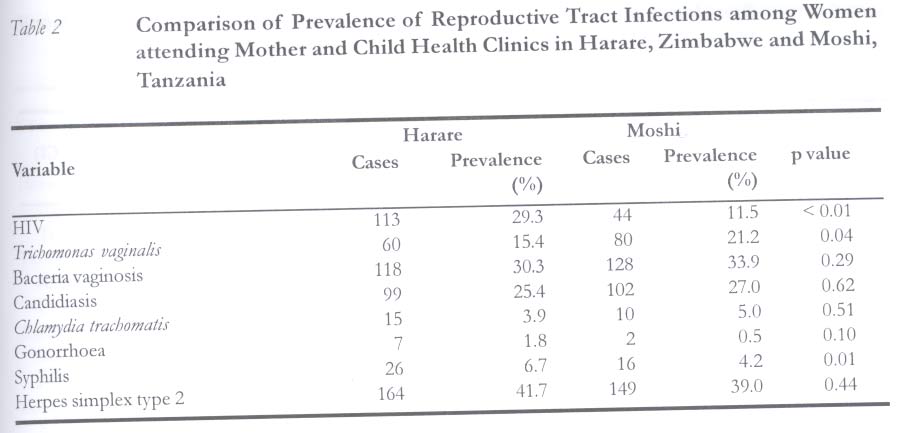
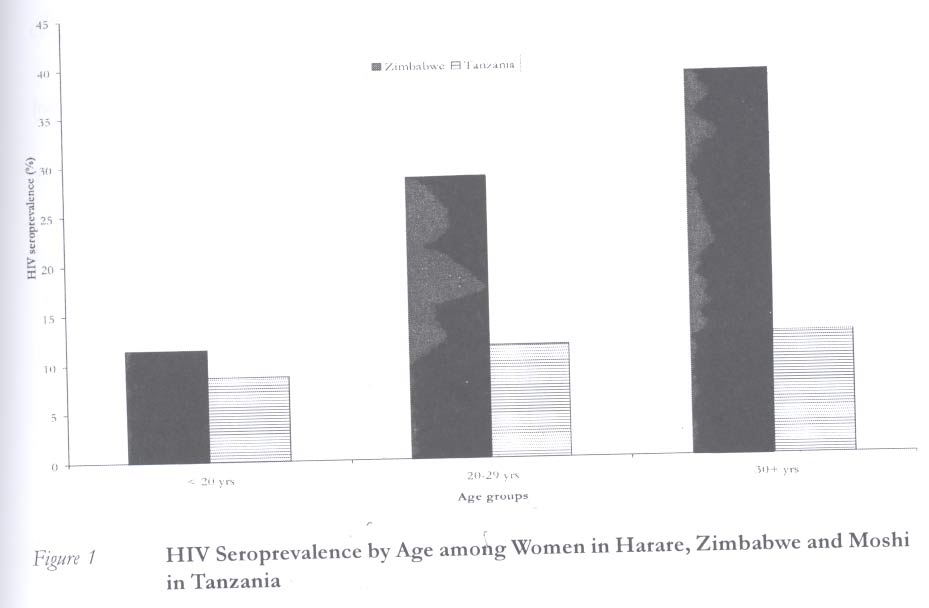
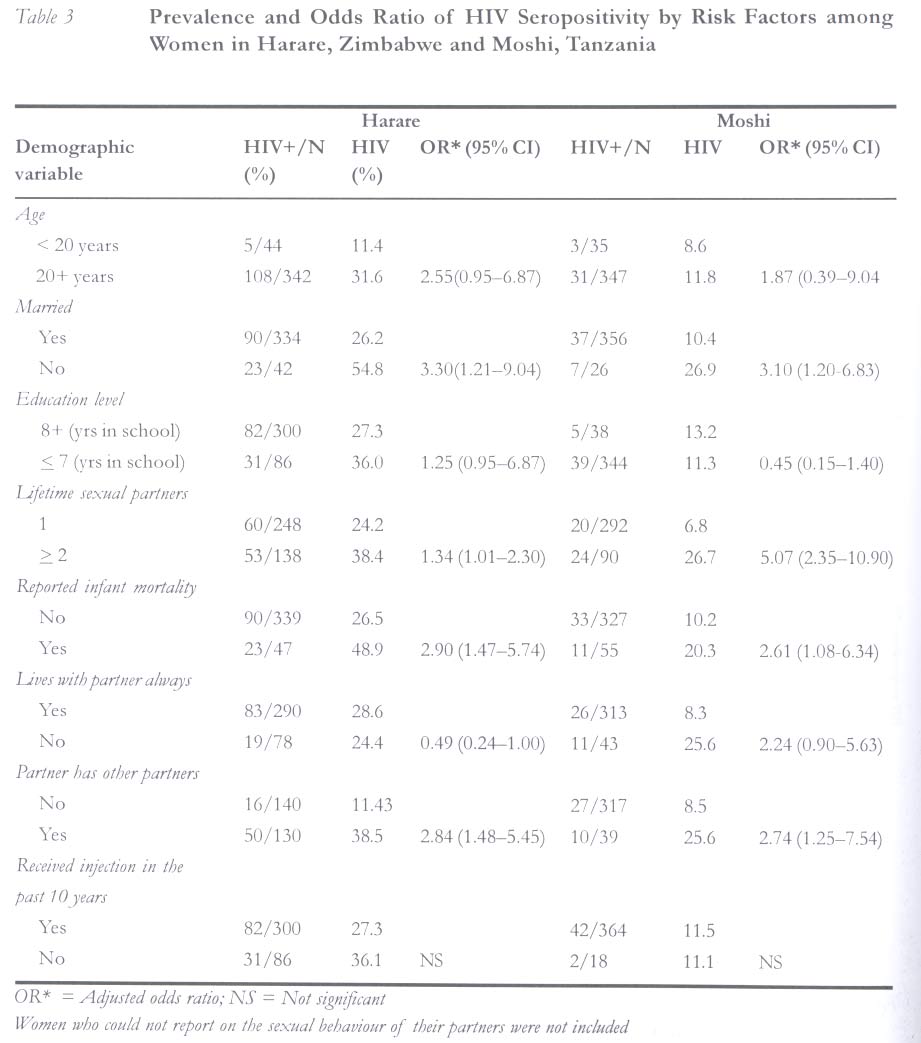
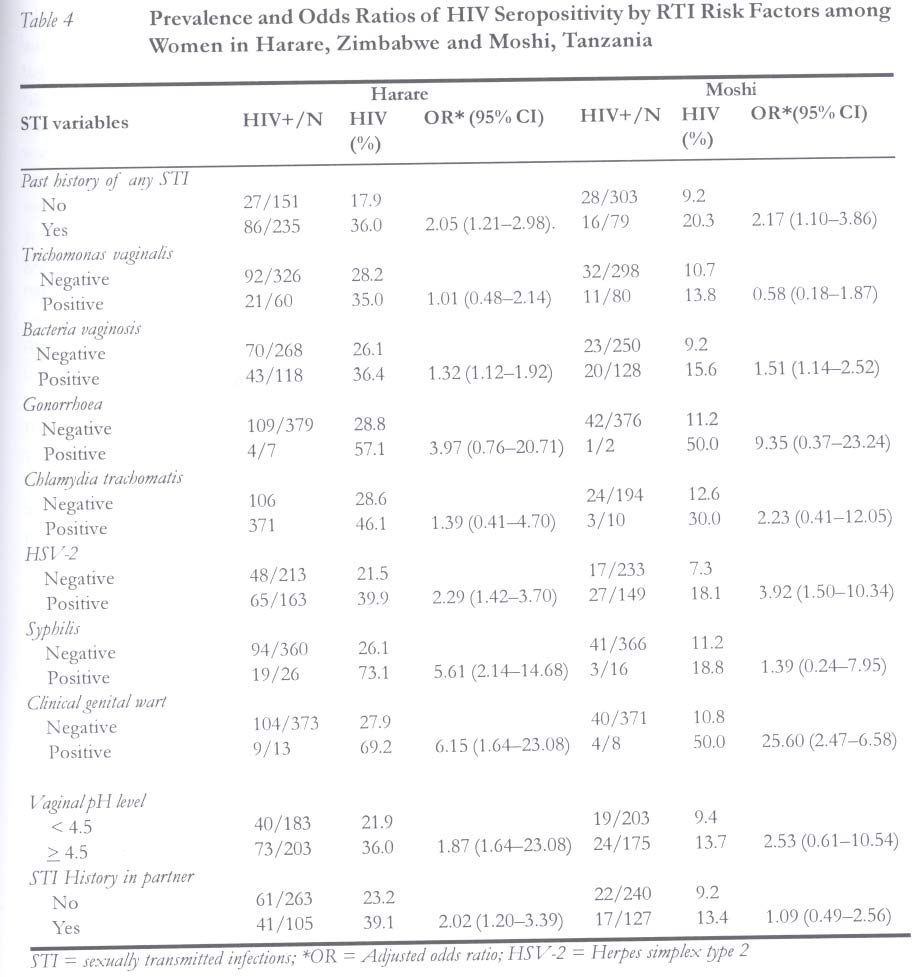
Christian Medical Centre, P. O. Box 3010, Moshi, Tanzania. Code Number: rh050101 Abstract In a cross-sectional study, 786 consenting women from two cities in Africa, Harare and Moshi, attending primary health care clinics were interviewed, examined and tested for HIV and other sexually transmitted infections (STIs). The aim of the study was to assess and compare differences in the characteristics that may affect the prevalence of HIV/STIs among women in the two cities. Multivariate analysis was used to generate odds ratio. STIs and behaviour characteristics among this low risk group of women could not fully explain the higher HIV prevalence in Zimbabwe, 29.3% compared to 11.5% in Tanzania (p < 0.01). Interventions should target identified risk factors with particular attention to youths. (Afr J Reprod Health 2005; 9[1]: 88-98) Résumé Le VIH et les infections sexuellement transmissibles chez les femmes qui fréquentent les centres de santé primaire urbain dans deux villes en Afrique sub-sahérienne. A travers une étude traversale, 786 femmes consentantes dans deux villes africaines à savoir Hararé et Moshi, qui fréquentaient les centres de santé primaire, ont été interviewées, examinées et ont fait des analyses pour determiner la présence du VIH et d'autres infections sexuellement transmissibles (ISTs). L'étude avait pour but d'évaluer et de comparer les différences par rapport aux caractéristiques qui pourraient affecter la fréquence de VIH/ISTs chez les femmes dans les deux villes. L'analyse multifactorielle a permis d'obtenir les rapports de chance. Les ISTs et les caractéristiques comportementales chez les groupes de femmes à haut risque ne pouvaient pas expliquer entièrement la fréquence plus élevée de VIH au Zimbabwe (29,3%) comparée à 11,5% en Tanzanie (p > 0,01). Les interiventions doivent viser les facteurs de risque identifiés tout en se concentrant sur la jeunesse.(Rev Afr Santé Reprod 2005; 9[1]: 88-98) Key Words: HIV/AIDS, STI, Zimbabwe, Tanzania, women Introduction Human immunodeficiency virus (HIV) infection in sub-Saharan Africa has become one of the greatest global challenges to public health. Preventing and mitigating its consequences require (1) a broad understanding of socio-behavioural and epidemiological features in diverse population settings and (2) tailoring messages and interventions accordingly. In 2002, cases of HIV infection in sub-Sahara Africa were estimated to be 3.5 million.1 According to the World Health Report 2002, current estimates suggest that more than 99% of HIV infections prevalent in Africa in 2001 were attributable to unsafe sex.2 African women bear the highest burden of HIV infection.3 Women of childbearing age are particularly vulnerable to HIV infection, and this has led to an increase in the number of paediatric HIV infections reported as a result of mother to child transmission (MTCT) during pregnancy, delivery and breastfeeding.4 There are, however, large variations in the prevalence of HIV infection within Africa, and much less is known on factors that confer variability to susceptibility. The variations in vulnerability to HIV infection could be a result of a number of endogenous and exogenous factors within populations, which include different patterns of sexual networking, acquisition modes, male circumcision status, condom use, effective treatment and prevention of sexually transmitted infections (STIs).3,5 Other factors that are thought to play a key role in facilitating HIV transmission are social inequality, poverty, migration and urbanisation.6 Interactions between other variables such as social background, age, race, education and gender have been implicated in making some groups more vulnerable than others.6 Ulcerative (syphilis, chancroid, herpes) and non-ulcerative STIs have been documented as enhancing infection with HIV.7-9 Elaboration of HIV prevalence and associated risk factors in similar study populations between different regions in Africa could help elucidate factors that determine the rate and extent of spread of HIV and, more importantly, provide insights into how interventions can be best targeted. The main objective of the present study was to assess and compare differences in the characteristics that may affect the prevalence of HIV/STIs among female attendees of primary health care clinics in two African countries, Tanzania and Zimbabwe. Methods Study Design Between July and December 1999, pregnant and non-pregnant women attending primary health care clinics in two African cities, Harare in Zimbabwe and Moshi in Tanzania, were invited to participate in a sexually transmitted infection study. It was a cross-sectional study involving 768 women; 386 in Zimbabwe and 382 in Tanzania. Identical protocol and questionnaire were used for recruitment of participants and data collection, and comparable laboratory methods of analysis were used for the detection of STIs. Study Sites Two Anglophone countries in Africa with different HIV prevalence, Tanzania in East Africa and Zimbabwe in Southern Africa, were selected. The first HIV reports from the two countries were in the mid 1980s.10,11 Background of Zimbabwe Zimbabwe has a population of about 11.5 million, 32% of whom live in urban areas.12 Harare, the administrative capital city of Zimbabwe has a population of 1.5 million. The health delivery system in Zimbabwe is organized into a four-tier referral system, whereby patients are initially seen at primary health clinics and then referred up the ladder to district/mission hospitals, provincial hospitals, and finally to central hospitals. Primary health care clinics are staffed by qualified nurses and midwives who render most of the services offered. Adult female literacy rates are estimated at 80%. About 95% of expectant mothers attend antenatal care (ANC ) clinics at least once during pregnancy.13 Background of Tanzania Tanzania has a total population of about 32.8 million.14 Moshi, the administrative capital of Kilimanjaro Region in Northern Tanzania has an estimated total population of one million people.15 Adult female literacy rate is estimated at 57%.16 About 80% of expectant mothers attend ANC clinics at least once during pregnancy.17 Tanzania has a comprehensive health care structure, and approximately 70% of the population live within 5km of a health facility.16 Health care facilities within the structure include, from the lowest up, village health services, dispensary services, health centre services, district hospitals, and referral/consultant hospitals. The primary health care clinics are run by trained nurses. Recruitment Sites Primary health care centres (PHC) mainly serving the lower socio-economic classes in the two countries were used as recruitment sites. In Harare, women were recruited from two PHCs, while in Moshi, Tanzania, three PHCs were involved. All the clinics offer reproductive health services, child health and curative services. They were selected based on relatively high patient volumes, accessibility and feasibility of performing clinical and laboratory analysis. Study Population The study population consisted of pregnant women attending antenatal care clinics, and non-pregnant women seeking family planning services or bringing their children to the clinic for routine immunization. In Tanzania, 392 women were approached but ten of them declined participation for various reasons. In Zimbabwe, 393 women were approached, four of them participated in the interview but left the clinic before being examined and three of them had their blood drawn but declined the HIV test. Eligibility Women were eligible to participate if they were aged 15-49 years, gave consent to participate in the study, were not menstruating, had not had a hysterectomy, and had not used any systematic antibiotic or vaginal antiseptic two weeks prior to enrolment. Counselling and Interview The questionnaire used was developed in English, translated into local languages, Shona in Zimbabwe and Kiswahili in Tanzania, and then re-translated into English. The questionnaire had been pre-tested and modified accordingly. Specially trained nurses conducted the pre and post-test counselling and face to face interviews in a private setting. Data were collected on socio-demographic characteristics, including age, marital status, educational attainment, occupation, reproductive history, sexual behaviour of self and that of sexual partner, contraception and history of previous and current STIs. Clinical Procedure and Biological Sample Collection At each site, a female study physician performed a general and gynaecological examination on all women. Vaginal and cervical specimens were collected and tested either on site or in designated laboratories in the two countries. Venous blood was collected for HIV, syphilis and herpes simplex type 2 (HSV-2) serological tests. Laboratory Methods Vaginal specimens Details of the methods used have been described previously.18,19 Briefly, Trichomonas vaginalis was diagnosed by wet mount microscopy. Bacterial vaginosis was diagnosed by applying Amsel's diagnostic criteria (presence of three of the following: homogenous thin vaginal fluid that adheres to the vaginal wall, pH of vaginal fluid > 4.5, presence of clue cells on wet saline mount, and amine-like odours on addition of 10% potassium hydroxide to vaginal secretions).20 Candidiasis was diagnosed by wet mount if yeast buds and/or pseudohyphae were observed on 10% potassium hydroxide slide preparation.18,19 HIV serology was performed using the Abbot determine HIV 1/2 test (Abbott Laboratories, Tokyo, Japan), and positive tests were confirmed by enzyme-linked immunosorbent assay (ELISA) (Murex Diagnostics, Dartford, UK).21 The presence of HSV-2 antibodies was detected from serum using enzyme linked immunosorbent assay (ELISA) (Gull Laboratories Inc, Salt Lake City, USA). Details of the methods used have been fully described elsewhere.22 Serological syphilis was detected using rapid plasma reagent test (RPR) (VD-25, Murex Diagnostics Dartford, UK), and positive tests were confirmed with the Treponema pallidum hemaglutination assay (TPHA) (Fujirebio Tokyo, Japan) in Zimbabwe, while in Tanzania syphilis was screened using the Abbott rapid test and confirmed with TPHA (Fujirebio, Tokyo, Japan).18,19 Cervical specimens Neisseria gonorrhoea (GC) and Chlamydia trachomatis (CT) were detected by the ligase chain reaction (LCR) test (Abbott laboratory) in Zimbabwe, while in Tanzania cervical antigens to CT were detected using the enzyme-linked immunosobernt ELISA (Abbott laboratory), and GC was diagnosed by culture.18,19 Genital warts were diagnosed during clinical examination. STI treatment Women were treated for curable STIs diagnosed and given one week follow-up appointment. During the second visit, the women were offered post-test counselling and treated for curable laboratory-diagnosed STIs. HIV test results were disclosed to those women who wanted to know their results. Women with STIs were encouraged to refer or bring their partners for free treatment at the study clinics. Statistical Analysis Data were analysed using the Statistical Package for the Social Sciences (SPSS). Statistical comparisons between the two cities were made using the χ2 test and Fisher's exact tests when appropriate. All p values presented are two-tailed. Logistic regression was performed using STATA 5.0 (STATA corporation, College Station, Texas, USA) to generate the adjusted odds ratios for the risk factors. The variables were selected, as previous data had shown them to be significantly associated with HIV risk in this population.21,23 Ethics Data collection commenced after ethical approval for the study had been obtained from the Norwegian Ethical Committee and from the Medical Research Councils of Tanzania and Zimbabwe. Results Socio-Demographic Variables and Sexual Behaviour Seven hundred and sixty eight women participated in this study. Table 1 shows a comparison of the socio-demographic characteristics and sexual behaviour of participants from the two cities. The social backgrounds of the women in Moshi, Tanzania, and Harare, Zimbabwe, were comparable. The mean age in both cities was 26 years (p = 0.92). Most of the women were not formally employed (p = 0.06), were married (p = 0.05) and lived with their sexual partners/spouse most of the time (p = 0.06). Age at sexual debut was 18 years (p = 0.54) and age at first marriage was 20 years (p = 0.36). A small proportion (28.5% in Harare and 27.8% in Moshi) of the women in both cities had ever used a condom in their lifetime. Educational level, however, was significantly different, with more women in Zimbabwe (77.9%) having attended eight or more years of schooling, while only 9.7% of women in Tanzania had reached the same level of school attendance (p < 0.01). While none of the women in Zimbabwe had undergone female genital cutting, 17% of women in Tanzania were circumcised (data not shown). Prevalence of HIV/RTIs among the Women Table 2 presents the prevalence of HIV and reproductive tract infections (RTIs) among women in the two cities. Overall, the HIV seroprevalence was significantly higher among Zimbabwean women (29.3%) than Tanzanian women (11.5%) (p < 0.01). HSV-2 was the most prevalent STI in the two groups of women, 41.7% in Zimbabwe and 39.0% in Tanzania (p = 0.44). The prevalence of TV (21.2%) was significantly higher in Tanzania compared to Zimbabwe 15.4% (p = 0.04). Syphilis seropositivity was significantly higher among Zimbabwean women (6.7%) compared to those from Tanzania (4.2%) (p = 0.01). The prevalence of bacterial vaginosis, candidiasis, Chlamydia trachomatis and gonorrhoea were comparable at the two sites. Gonorrhoea was the least prevalent STI in both groups of women, 1.8% among Zimbabwean women and 0.5% among Tanzanian women respectively (p = 0.5). HIV Prevalence by Age Figure 1 depicts the HIV seroprevalence by age among women in Tanzania and Zimbabwe. Peak HIV seroprevalence was found among women aged 30 years or more, being 39% in Zimbabwe and 12.4% in Tanzania. Among women aged 20-29 years in Zimbabwe, HIV seroprevalence was 28.5%, compared to 11.5% in Tanzania. Among the youngest group of women (15-19 years), HIV prevalence was not significantly different in the two cities, 11.4% in Zimbabwe and 8.6% in Tanzania. Risk Factors for HIV Results of the socio-demographic risk factor analysis in the two cities are shown in Table 3. Reported sexual behaviour of the women was largely comparable. Socio-demographic risk factors common to both groups were: being single, history of having had two or more lifetime sexual partners, a partner who was known or suspected of being non-monogamous and a report of having experienced infant mortality. As shown in Table 4, past history of STI, HSV-2 seropositivity and clinically diagnosed genital warts were associated with HIV seroposi-tivity in both Moshi and Harare. Syphilis seropositivity and vaginal fluid pH > 4.5 were independent risk factors for HIV infection among women in Zimbabwe. History of STI in the participant's husband or partner was an independent risk factor in Harare. Discussion STIs have been well documented as risk factor for HIV infection.21,23 Our data show that overall the prevalence of HIV among Zimbabwean women was almost three times that of Tanzanian women. We had hypothesised that among women in Harare, with higher HIV prevalence, other STIs and reported risky behaviour would be more common. The results reveal that women in Zimbabwe, despite a high HIV prevalence, did not become sexually active at an earlier age than their peers in Tanzania, and that HIV seroprevalence among the youngest group of women (15-19 years) was not significantly different. However, with increase in age, HIV prevalence doubled among women aged 20-29 years and trebled among those aged 30 years and above in Zimbabwe when compared to Tanzania. This suggests increased vulnerability and/or greater efficiency of HIV transmission among Zimbab-wean women. Two parameters were shown to be significantly more prevalent among Zimbabwean than Tanzanian women. First, more women in Zimbabwe were syphilis seropositive. This supports previous reports on the associative relationship between syphilis and HIV infection.8 The number of women who were syphilis seropositive was however small to offer full explanation of the high magnitude of HIV seroprevalence in Harare. Second, vaginal pH greater than 4.5 was more likely to be present in Zimbabwean women. Acidic vaginal pH has been associated with reduced susceptibility to both STIs and HIV infection.24 The design of this study, however, does not establish causal association in the absence of historical pH status. Nonetheless, association of HIV with high vaginal pH is an important finding in this population, where it has been documented that intravaginal practices are common.25 Women who reported that they knew or suspected that their partners were involved in non-monogamous relationships were more likely to be HIV seropositive in both cities. This calls for the need to explore sexual networking patterns among men and women. Such data will likely provide insights into whether HIV prevalence in non-core groups is a result of open or closed socio-sexual networking.26 In view of mounting anomalies in HIV infection in Africa, Thomas et al suggested that rapid propagation of STIs has been associated with core groups, which make up a small proportion of the susceptible population that is responsible for most community transmission.27 However, there is a dearth of studies from Africa in which the patterns of social networking are elaborated. Although this study did not investigate the circumcision status of the male partners of the women recruited, we previously documented that 17% of Tanzanian women were circumcised while none of the women in Zimbabwe had undergone this procedure.28 Literature review also shows that circumcision, not only of women, but also of men is a common practise in Tanzania.29 Auvert et al, in a STI study of four cities, reported low HIV prevalence among circumcised compared to non-circumcised men in two cities with low HIV prevalence.29 The present study revealed similarly high HSV-2 seroprevalence among women in the two cities, although HIV seroprevalence was three times higher in Zimbabwe. HSV-2 has been reportedly associated with increasing susceptibility to HIV infection.30 More research is needed to further define factors that may influence the variations in HIV prevalence in populations with similar HSV-2 seroprevalence as shown in this study. Although HIV seroprevalence was lowest among the youngest age group of women in both cities, this level of infection was dis-appointingly high. This underscores the need for novel prevention strategies that include sexual health and family education and counselling among adolescents. This study and other reports show that in both Zimbabwe and Tanzania more than 50% of women attend school at least up to primary level.13,16 The school system, therefore, offers a chance for reaching a large group of youth with reproductive and sexual health education geared at promoting positive attitudes and behaviour that reduce risk of STIs and HIV infection. Integrating reproductive and sexual education early into the primary school curriculum should be promoted. This study revealed that although only a few women reported having more than one lifetime sexual partner, this behaviour, nonetheless, was associated with HIV infection in both cities. While the interviewers that collected the data were well trained, it is possible that the responses to sexual behaviour questions could have been subject to social desirability bias.31 Ninety per cent of the women were married, therefore, their responses may also have been influenced by perceived cultural norms of behaviour, a desire to conceal socially proscribed activities or the women's perception of the views of the interviewers. The difference in HIV prevalence between Zimbabwe and Tanzania may not be an outcome of differences in the onset or stage of the epidemic, as the time of first reports of infection were made in the mid eighties in both countries.10,11 A reported history of infant mortality was associated with HIV infection in both groups of women. This could be used in risk assessment of women seeking reproductive health services and could be used as an entry point for HIV counselling and testing that may lead to the promotion of prevention of mother to child transmission (PMTCT). Conclusions The results of this study show that whereas STIs are an important factor in the spread of HIV infection in Africa there may be need for more research to find other factors that accelerate the rate of HIV acquisition or contribute to the differences in prevalence patterns. This is particularly so in the context of countries in sub-Saharan Africa such as Zimbabwe where HIV prevalence was disproportionately high compared to Tanzania, despite similar socio-demographic and behaviour characteristics. The high HSV-2 prevalence associated with HIV in both countries underscore the need for prevention and control of this viral STI. In addition, we recommend upstreaming of HIV/STI programmes that focus on adolescents before they become sexually active in both countries. Acknowledgements Our special thanks go to the women who participated in the study. We acknowledge the contribution of the investigators and staff at PHCs where the project was conducted - Moshi in Tanzania and Harare in Zimbabwe - and staff of the Department of Obstetrics and Gynaecology, University of Zimbabwe Medical School and the Kilimanjaro Christian Medical Centre. We also thank the Medical Research Councils of Zimbabwe and Tanzania and the Norwegian Ethical Committee for permission to carry out the study. We thank Dr F Ndowa for his useful comments on the paper. Funding was provided by the National Cancer Association of Norway and the Letlen Foundation. References
© Women's Health and Action Research Centre 2005 The following images related to this document are available:Photo images[rh05011t1.jpg] [rh05011t4.jpg] [rh05011t3.jpg] [rh05011t2.jpg] [rh05011f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}