 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 9, No. 1, April, 2005 pp. 128-132 Is Serum Magnesium Estimate Necessary in Patients with Eclampsia on Magnesium Sulphate? BA Ekele1 and SLH Badung2 Departments of 1Obstetrics and Gynaecology, and 2Chemical
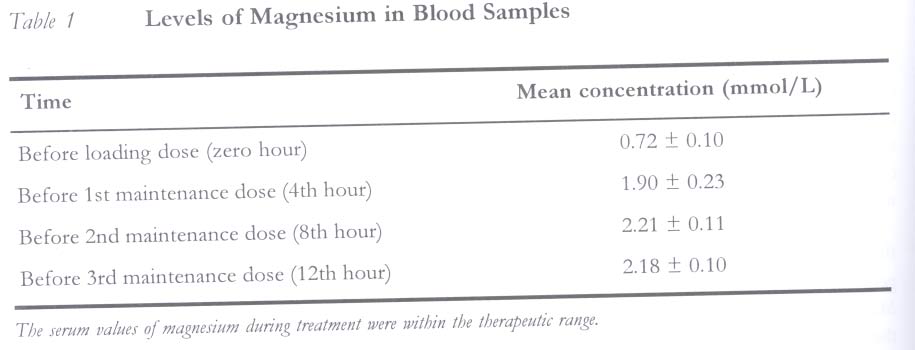
Pathology, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria. Code Number: rh05015 Abstract The therapeutic index of magnesium is said to be low, hence, there are fears of toxicity when used as anticonvulsant in eclamptic patients. The objective of this study was to determine the serum levels of magnesium in eclamptic patients treated with magnesium sulphate and relate the levels with clinical indicators. It was a prospective study involving consecutive eclamptic patients that were managed between January and December 2002, with magnesium sulphate as the sole anticonvulsant agent, using a modified Pritchard regimen. Blood samples were taken before the administration of the loading and maintenance doses of magnesium sulphate and serum levels of magnesium were estimated using the Jenway 605 colorimeter. There were 19 patients and 72 blood samples. The mean baseline serum magnesium was 0.72 ± 0.10mmol/L while serum magnesium levels when the patients were on treatment ranged from 1.95 to 2.82mmol/L. No serum magnesium level was greater than 3.0mmol/L and none of the patients had clinical evidence of magnesium toxicity. We conclude that serum magnesium levels in these patients were within the therapeutic range, therefore, routine estimation of this cation is not necessary. Even where the laboratory facility is available, it is suggested that serum estimation be limited to cases where clinical monitors suggest toxicity. (Afr J Reprod Health 2005; 9[1]: 128-132) Résumé Faut-il évaluer les concentrations sériques du magnesium chez les malades éclamptiques qui suivent un traitement du sulfate de magnesium? On dit que l'indice thérapeutique du magnesium est bas, donc l'on craint la toxicité quand il est employé comme un anticonvulsivant chez les malades éclamptiques. Cette étude avait pour objectif d'évaluer les concentrations sériques du magnesium chez les malades qui suivent un traitement du sulfate de magnesium et d'établir un rapport de ces concentrations avec des moniteurs cliniques. Nous avons mené une étude prospective des malades éclamptiques consécutives qui suivaient un traitement entre janvier et décembre 2002 en utilisant le sulfate de magnesium comme le seul anticonvulsivant à l'aide d'un Schéma de Pritchard modifié. Des échantillons de sang ont été prélevés avant d'administrer la dose d'attaque et la dose d'entrentien du sulfate du magnesium; des concentrations sériques du magnesium ont été estimée à l'aide d'un colorimètre de Jenway 605. Il y avait 19 malades et 72 échantillons de sang. La ligne de base moyenne de la sérique du magnesium était 0,72±0, 10mmol/L alors que les concentrations sériques du magnesium pendant que les malades suivaient le traitement variaient de 1.95 à 2,82mmol/L. Il n'y avait aucune concentration sérique du magnesium qui était supérieure à 3,0mme/L et aucune des malades n'avait une évidence d'une toxicité du magnesium. Nous affirmons en conclusion que les concentrations sériques chez ces malades étaitent dans les limites thérapeutiques. En conséquence, l'évaluation de routine de ce cation n'est pas nécessaire. Même là où les structures de laboratoire ne sont pas disponibles, nous proposons que l'évaluation sérique soit limitée aux cas où les moniteurs cliniques indiquent la toxicité.(Rev Afr Santé Reprod 2005; 9[1]: 128-132) Key Words:Eclampsia, serum, magnesium, toxicity, anticonvulsant Introduction Eclampsia, the occurrence of a seizure in associa-tion with pre-eclampsia, is a major cause of maternal mortality in developing countries.1-3 Morbidity and mortality in eclampsia is related to the number of convulsions. The control of convulsions is, therefore, important in reducing maternal morbidity and mortality. Until recently pharmacological treatment of the convulsions has been determined largely by geographical background, habit and prejudice. Magnesium sulphate was the drug of choice in the United States, while diazepam and phenytoin were favoured in Britain.4 None of the choices was influenced by strong scientific evidence until the collaborative eclampsia trial produced compelling support for the use of magnesium sulphate.5 Despite that, the traditional arguments against the use of magnesium sulphate centres on its perceived toxicity and the difficulties in measuring magnesium concentrations during treatment.6 This fear is widespread in other commonwealth countries, to the extent that one of the reasons advanced for not using magnesium sulphate widely in Nigeria was the inadequate laboratory services back-up.7 But do we really need such laboratory services before using magnesium sulphate? At the Usmanu Danfodiyo University Teaching Hospital, Sokoto, in Nigeria, we do not have the facility to prepare magnesium sulphate solution but we can estimate serum levels of magnesium in our laboratory. Magnesium sulphate is also not easily available in most pharmacy retail shops in the country. On request, we obtained some free supply of 50% magnesium sulphate from the Magpie co-ordinating centre, Oxford, when we were admitted to participate in the Magpie trial.8 We took the opportunity to estimate the serum levels of magnesium in eclamptic patients on magnesium sulphate treatment and related serum levels with clinical findings. Materials and Methods Patients admitted to the labour ward with eclampsia during the study period (January to December 2002) who were placed on magnesium sulphate as the sole anticonvulsant were recruited for the study. Those who had diazepam or any other anticonvulsant agent before or at admission were excluded. A modified Pritchard regimen was used in the management of the eclamptic convulsions in which a loading dose of 4g intravenous magnesium sulphate was administered over 10 minutes, followed immediately by 10g of deep intramuscular magnesium sulphate (5g on each buttock). A maintenance dose of 5g intramuscular magnesium sulphate was then administered every four hours on alternate buttocks for 12 hours. The respiratory rate, urinary output and tendon reflexes were monitored regularly and before each maintenance dose. Absent tendon reflexes and/or respiratory rate < 16/minute were taken as clinical evidence of toxicity. Calcium gluconate (10ml of 1%) was made available for management of overdose or toxicity. Venous blood sample was taken before the loading dose and before each of the maintenance doses. Unhaemolysed serum samples separated through centrifugation were assayed for total serum magnesium using the xylidyl blue colorimetric principle and the Jenway 6051 colorimeter. Results Nineteen patients with eclampsia fulfilled the criteria for inclusion. Their mean age was 18.3 years, while their mean body mass index (BMI) was 21.9. Seventeen of the patients were primigravida, while intrapartum eclampsia was the most common type (12 patients). One patient had recurrent fit within 30 minutes of initiating treatment with magnesium sulphate and an additional 2g of intravenous magnesium sulphate abated the seizure. There was no loss of deep tendon reflexes or respiratory depression in any of the patients. The first maintenance dose in one patient was skipped when oliguria was noticed after the loading dose. Subsequent maintenance doses were resumed in the patient when urinary output was adjudged adequate. There was no maternal death. Seventy two blood samples were assayed for serum magnesium. The baseline mean serum level of magnesium before commencement of treatment was 0.72 ±0.10mmol/L. The mean serum levels before the four-hourly maintenance doses are shown in Table 1. Discussion The Pritchard regimen9 of magnesium sulphate administration in which the maintenance dose is administered by the intramuscular route every four hours was chosen in preference to the Zuspan10 intravenous route because we do not have infusion pumps; for careful infusion by gravity is said to be difficult to control.11 The intermittent intramuscular injections also made it possible for blood samples to be taken just before the administration of the next dose of the magnesium sulphate. The baseline mean serum magnesium concentration for the eclamptic patients in this study was 0.72mmol/L. This value is lower than 0.85 ± 0.11mmol/L found for patients with severe pre-eclampsia in a Dutch study.12 For human serum, the reference value for total magnesium is 0.70-1.00mmol/L.13 Therefore, the values obtained for these eclamptic patients can be described as low normal. The mean serum magnesium level before the first maintenance dose was 1.95mmol/L, which is the lower limit of the suggested therapeutic level of 2.0-3.5mmol/L14, while subsequent serum levels remained at a mean of 2.1mmol/L. That only one patient had a recurrent fit despite this therapeutic level is instructive. We suspect that the relatively young and small size of our patients might be responsible for the good seizure control despite the apparently low therapeutic levels. The absence of clinical signs of magnesium toxicity in any of the patients was corroborated by the serum levels that were within the therapeutic range. The only patient that had oliguria after the loading dose had positive tendon reflex, but the first maintenance dose was skipped and serum magnesium levels were under 3.0mmol/L. In fact the therapeutic index of magnesium is not as narrow as was previously thought. The first warning sign of impending toxicity in the mother is the loss of the patellar reflex at plasma concentrations between 3.5 and 5mmol/L, while respiratory paralysis is said to occur at 5-6.5mmol/L, cardiac conduction is altered at greater than 7.5mmol/L, and cardiac arrest is expected when serum magnesium concentration exceeds 12.5mmol/L.14 Therefore, meticulous monitoring of the clinical parameters should reveal early signs of toxicity for appropriate steps to be taken. We did not have course to use calcium gluconate in any of the patients in our series. A similar study from Thailand also suggested that in most situations, clinical assessment of deep tendon reflexes, respirations and urine output is adequate to monitor maternal magnesium toxicity without the need to determine actual maternal serum levels.15 There was no maternal mortality in this series. Even though our number is small, other workers have reported significant reduction in maternal mortality with the introduction of magnesium sulphate.16 In conclusion, serum magnesium levels of eclamptic patients on magnesium sulphate as the sole anticonvulsant drug using a modified Pritchard regimen17 were within the therapeutic range. Absence of clinical evidence of magnesium toxicity correlated well with the serum magnesium levels. It is recommended that there should be more widespread use of magnesium sulphate without the need for serum magnesium estimation, provided clinical monitors are satisfactory. Acknowledgments We are grateful to the Magpie Trial Co-ordinating Centre at Oxford for providing some of the magnesium sulphate used for this study. We also thank Mr. A. Adesoji and Mr. Bitrus of the Chemical Pathology Department for their assistance. References
© Women's Health and Action Research Centre 2005 The following images related to this document are available:Photo images[rh05015t1.jpg] |
| |||||||||

{kind=link}