 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 9, No. 2, August, 2005, pp. 76-91 What Happened to the IUD in Ghana? I Osei1, H Birungi 2, G Addico3, I Askew2 and JO Gyapong1 1Health Research Unit, Ghana Health Services. 2Frontiers
in Reproductive Health Program, Population Council, Nairobi, Kenya. 3United
Nations Population Fund, Ghana. Code Number: rh05027 Abstract The intrauterine contraceptive device (IUD) is a safe and reversible contraceptive method that requires little effort on the part of the user. Once inserted, it offers 10 years of protection against pregnancy. However, its use in Ghana has stagnated in relation to other contraceptive methods. An exploratory study was, therefore, conducted to examine the client, provider and system characteristics that affect the demand for IUD. Data were gathered through secondary analysis, in-depth interviews, focus group discussions and simulated client survey. The stagnating demand for IUD is attributed to clients' perceptions and rumours about IUD. The fear of excessive bleeding and weight loss discourages potential users. The product design was also perceived to be unacceptable. Demand creation for the IUD has been poor and the number of providers with practical experience of insertion is insufficient. Contrary to the belief that providers' bias contributes to the decline in use, findings show that providers have a favourable attitude towards the product. (Afr J Reprod Health 2005; 9[2]: 76-91) Résumé Le dispositif intra-utérin (DIU) est une méthode contraceptive reversible et sans danger qui exige très peu d'effort de la part de l'usagère. Une fois qu'il est inséré, il offre une protection de dix ans contre la grossesse. Pourtant, son emploi au Ghana a été retardé par rapport aux autres méthodes contraceptives. On a donc mené une étude d'exploration afin d'examiner les caractéristiques du client, du fournisseur et du système qui ont des effets sur la demande pour le DIU. Les données ont été recueillies à l'aide d'une analyse secondaire, des interviews en profondeur, des discussions à groupes cible et d'une enquête du client simulé. La demande diminuée pour le DIU est attribuée aux perceptions du client et aux remeurs à l'égard du DIU. La peur de l'hémorragie excessive et la perte de poids découragent les usagères potentielles. La manière dont le produit a été fabriqué était perçu comme inaceptable. La création de la demande pour le DIU a été médiocre et le nombre de fournisseurs qui ont l'expérience pratique de l'insertion n'est pas suffisant. Contrairement au déclin dans l'usage du DIU, les résultats ont montré que les fournisseurs ont une attitude favorable envers le produit. (Rev Afr Santé Reprod 2005; 9[2]: 76-91) Key Words: IUD, perceptions, eligibility, STI, HIV, demand, Ghana Introduction The IUD is a safe and reversible contraceptive method that requires little effort on the part of the user. Once inserted, it offers 10 years of protection against pregnancy. In spite of these advantages, promotion and demand for the method has been on the decline in many countries. In a number of countries, including Ghana, the use of IUD in relation to other contraceptive methods is reported to have either stagnated or declined.1,2 For instance, the use of IUD among married women declined in Indonesia from 13% in 1991 to 10% in 1994.6 In Kenya, IUD use dropped from 31% among modern method users in 1984 to 15% in 1993.3 In Guatemala, IUD use has remained stable at around 2% despite an overall increase in contraceptive prevalence from 23% in 1987 to 38% among women in union in 1998/99.4 In Ghana, national estimates from the Ghana Demographic Health Survey (GDHS) indicate that modern contraceptive prevalence doubled from 5% in 1988 to 10% in 1993, and increased to 13% in 1998. A steady increase in the use of the pill, injectables and condoms has been observed. However, use of the IUD has remained stagnant at 1% over a period of 10 years.2 Overall, couples' knowledge of family planning methods is high (89%) in Ghana, but varies by type of method. Only 35.5% of the couples had ever heard about the IUD.2 The IUD is readily available through the Ghana Health Service (GHS), Ghana Social Marketing Foundation (GSMF), Ghana Registered Midwives Association (GRMA), and Planned Parenthood Association of Ghana (PPAG) clinics. However, recent service statistics drawn from these sources show a 40% decline in the provision of the IUD, from 25,000 acceptors in 1995 to only 10,000 in 2000. Yet the Ghana situation analysis study shows convincingly that IUD, and its insertion equipment, are available at most family planning service delivery points.5 Also, information exchange on the IUD takes place in almost three quarters of provider-client interactions, and yet this does not seem to translate into increased demand for the method.5 A study among IUD acceptors in Indonesia points out that changes in the use of IUD over time have been caused by a variety of factors including availability of methods, availability of medical facilities and skilled personnel, campaigns to promote specific methods, medical barriers, side effects, management of side effects and changes in user preferences.6 With respect to side effects and health concerns, some studies show that use of the IUD is significantly associated with reproductive tract infections.7 Indeed, the World Health Organization's (WHO) medical eligibility criteria for safe use of contraceptives state that current sexually transmitted infection (STI) contraindicates IUD use, as does any previous STI that has not been cured for at least three months.8 The guidelines also emphasise that insertion of the IUD in an HIV- infected woman or one who is at high risk of infection is not usually recommended. Safety concerns for HIV positive women using IUDs include the fear that a woman's immune system may be weakened and unable to fight off infections, such as another STI that could lead to pelvic inflammatory disease (PID). Findings from a recent study in Kenya, however, raised questions about the WHO guidelines. The study found that 156 HIV-infected women, including those whose immune systems were suppressed at the time of the IUD insertion, had no more overall complications (i.e., PID, removal due to pain, bleeding or pain, expulsion or pregnancy) following insertion than did the 493 uninfected women.9 Regardless of such findings, in certain settings these guidelines seem to have decreased demand for IUD as well as brought about discontinuation among existing acceptors. In the Philippines, side effects and/or health concerns were the most commonly cited reason for discontinuing use of the IUD. Program statistics show that 22% of IUD users discontinued use within a year of adoption because of side effects and health concerns.1 A study in Kenya identified five interrelated factors for the declining trend in the use of IUD: fear of HIV acquisition/transmission, poor quality of care, poor product image, provider bias or preference, and changing client method preferences.3 At the program level, the critical question for understanding the determinants of contraceptive method choice is whether use of a method is predominantly provider or client driven.3,10 Provider-driven practices include the provider favouring some methods and discouraging others in the absence of sound medical rationale as well as failing to ascertain and consider the preferences of the client.11 In an ongoing study to assess the declining use of IUD in Guatemala, Brambila4 argues that such problems possibly originate from the lack of IUD training among service providers, who may not feel confident to offer the service to potentially interested women or, based on personal experiences, providers might have personal preferences. Providers might simply have a generalised negative feeling towards the IUD. On the other hand, method choice is also substantially affected by client or individual's fears of health side effects, whether these are real or based on unfounded rumours.12,13 Given the lack of understanding of the reasons IUD use in Ghana has stagnated and may well have declined, an in-depth assessment was carried out from March to November 2002 to: (1) examine the determinants and switching pattern/behaviour of IUD users; (2) assess the role of socio-cultural perceptions and misperceptions on the use of the IUD; (3) assess providers' and clients' attitudes towards the use of the IUD; (4) assess the content and quality of information exchange between the provider and client on the IUD; and (5) identify provider and other system barriers including pre-service and in-service training, logistics, supply and cost issues that may restrict clients' access to the IUD. Methods The assessment included both quantitative and qualitative methods of data collection. The first part of the study was a secondary analysis of data from the Ghana Demographic Health Surveys (GDHS), Ghana Situation Analysis (GSA) and existing service statistics, to explore trends in the use of the IUD. The second component of the study involved the collection of qualitative data through in-depth interviews, focus group discussions and the use of simulated clients. Data were collected at the national level and three regions. The ten regions in the country were first grouped according to the patterns of IUD use. Greater Accra, Eastern and Volta Regions were then selected on the basis of trends (increasing, decreasing and non-use respectively) in the proportion of married women currently using contraceptives that are using the IUD. The region with the highest contraceptive prevalence level was purposively selected to maximize familiarity with the method, but also to understand factors that shape fluctuation in the use patterns of IUD particularly in the case of the Greater Accra Region. Two districts (rural and urban) were randomly selected from each region, then two sub-districts were randomly selected from each district, giving a total of 12 sub-districts. One government health facility in each sub-district and the district hospitals were included in the study. In addition, two private facilities were randomly selected from each region. At least one family planning service provider from each of the selected service delivery points (SDP) was randomly selected and interviewed. A total of 35 providers were interviewed. The majority of providers interviewed were midwives (26), with few community health nurses (7) and medical officers (2). In-depth interviews were conducted at both the national and regional levels to explore contextual and programmatic factors expected to influence provision of the IUD. At the national level, in-depth interviews were held with senior policymakers in the Reproductive and Child Health Unit of the Ghana Health Services and the National Population Council (NPC). Key staff at IUD distributing sources in the country, IUD insertion training institutions, and USAID collaborating agencies were also interviewed. Focus group discussions (FGDs) were held in all the three study regions to examine contraceptive choice determinants among potential family planning clients. IUD is a method that is usually recommended for spacing or limiting the number of pregnancies. Thus, in order to understand the demand factors for the IUD, group discussions were arranged around two strata: women who were interested in having additional children but wanted to space them and women who wanted to stop having children. An intended group discussion with actual users had to be cancelled due to difficulties in recruiting participants. Altogether, 12 group discussions were held in six urban and six rural communities in the three regions. The communities were randomly selected from the catchment area of the facilities visited. The group participants were recruited from either the family planning clinics or the maternal and child health care clinics of the respective service delivery points (SDP). Simulated clients (SC) were used to examine provider knowledge and attitudes regarding IUD and whether providers recommend the IUD to women who intend to delay, space or stop giving birth.14 This component also investigated possible provider biases related to age, parity and marital status (including type of marriage). Use of the SC method originates from a need to remain as unobtrusive as possible. Concurrence to undertake the study was sought from the regional directors of health services in the respective study regions. Seven individuals, who represented seven different family planning client profiles, were recruited as SC, including:
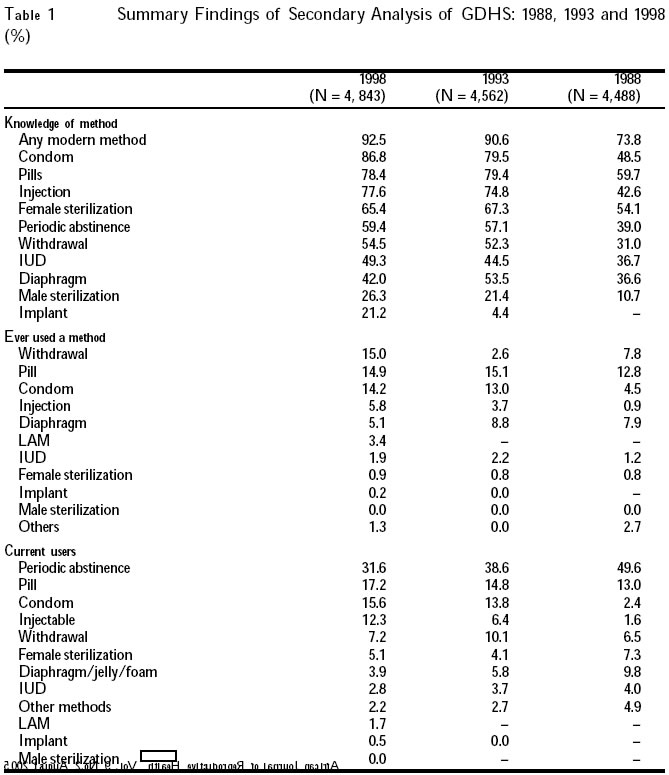
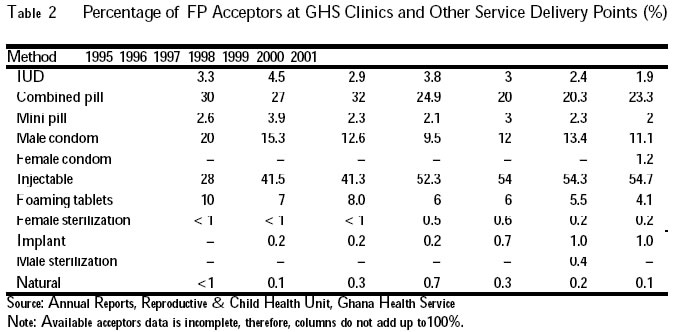
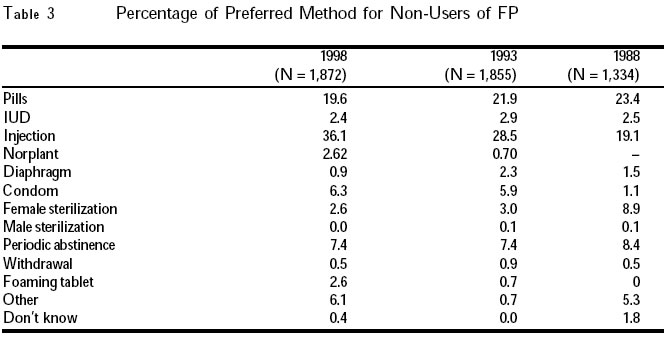
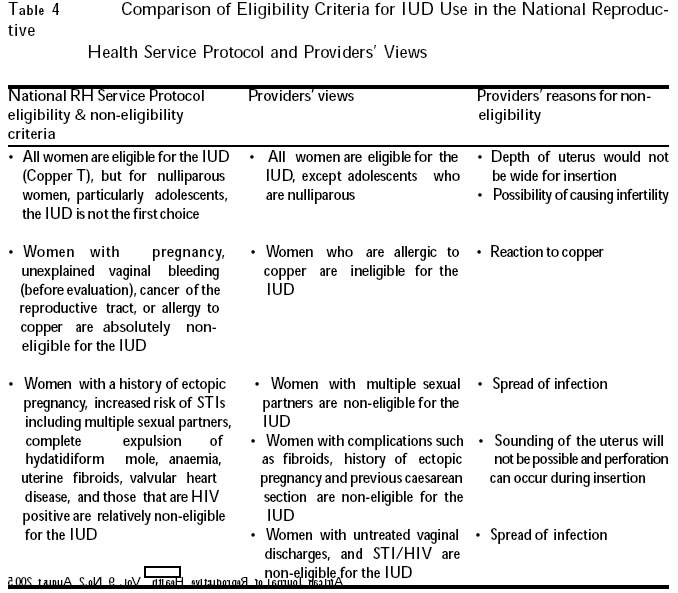
The SC were trained on the basis of a standardised scenario to ensure that they all could convincingly and accurately present it. They were women who needed information about the most effective method for delaying, spacing or stopping birth. They were to request a contraceptive method they could use for a long time (at least two years), inform the provider that they were in a stable relationship and that, to the best of their knowledge, they had no sexually transmitted diseases. Since pregnancy contraindicates most methods, the SC were advised to tell the provider that they were in the fourth day of menstruation. They were also instructed to specifically ask about the IUD if the provider did not volunteer information about it, to ensure that some information was exchanged about the method in each interaction. They were to decline a pelvic exam, and if consultation progressed to the point of inserting the IUD, the SC was to indicate that she wanted to consult with her partner first, thanked the provider and left. A de-briefing interview was held between the SC and the team leader immediately after the clinic visit. The SC together with the team leader then completed a questionnaire. Each of them made one visit to the 23 SPD using the same scenario for each visit. A total of 159 SC visits were made. The visits were undertaken on separate days to minimise suspicion and/or potential bias. Findings Trends in IUD Use Secondary analysis of the GDHS data (Table 1) shows that from 1988 to 1998, women's knowledge about the IUD has been increasing, although it was relatively low in comparison to other modern methods. A very low proportion of women contraceptive users reported ever using the IUD. Annual family planning records showed a steady increase in the acceptance rates of the injectable at service delivery points and a declining trend for all other methods including the IUD (Table 2). Similarly, data on current use among all women showed a steady decline in the use of IUD. Whereas the pill, injection and condoms have increased in usage over the years, IUD use dropped from 4% in 1988 to 2.8% in 1998; illustrating a decline over a period of 11 years. This decreasing trend was also found with female sterilisation. Preferred method for non-users (Table 3) also showed a low preference for IUD over the period (1988, 1993, 1998). The preferred future method of choice for non-users was the injection, followed by the pill. There was also an intended preference for both the condom and Norplant. The 1993 GDHS enquired about reasons for discontinuing a method. Overall, side effects were cited as the major reason for discontinuing use of the IUD. Among the 17 IUD users interviewed, nine had stopped use because of side effects. Other reasons given were desire for more children (4), religion (1), health concerns (1), infrequent sex (1), and not being married (1). Knowledge, Perceptions and Practices Knowledge about IUD All participants of the FGD had heard about family planning and could mention a few methods. The most frequently and spontaneously mentioned method was the injectable, followed by the pill, and sometimes Norplant. The IUD was mentioned occasionally and usually required some prompting by the facilitators. Many of the participants had never seen the IUD, though they had heard about it. Those who had seen it `weighing' described it as a metal thing or spring with strings attached to it. As one respondent commented: It is like the hook they use to catch small fish. Others described it as "a cross" and "a needle." One participant said the IUD is an object inserted at the entrance of the womb to prevent the entry of sperm. In general the responses given by the various FGDs were similar and lacked a good knowledge of IUD. Fears and Rumours about IUD Most of the FGD participants had never used or seen the IUD. When shown a sample, they expressed some apprehension about how such an object could be inserted into one's body. Their responses repeatedly underlined their fears. As stated: " I am afraid because of the design", "the metal in the middle is scary", "it can hurt you", "it is like a broom, it can hurt you during sex" " it is a wire, maybe it will rust and destroy you I think that is the cause of the bleeding". They speculated about the possible effects. They wondered whether such a thing would not hurt a man's genitals, cause sickness, slip inside one's body if not properly inserted, melt in the body, or irritate the partner's penis. The presence of the strings was also a cause for worry; as stated by one respondent: "I hate the strings." Discussants also worried about whether their husbands would not accidentally pull the strings during intercourse. The possibility that it could cause some discomfort for their spouses was mentioned frequently. Some respondents also said it could get pushed into the stomach by a long penis. Others felt the presence of the strings would make their partners suspect that they were up to something. As noted by one respondent: As for the men, they are troublesome. Before you realise he has seen it, and will say you have done juju (love medicine). Another added: Indeed he will think it is medicine to make him love me more. The focus group discussions also revealed several rumours surrounding the IUD. One participant narrated the story of a friend whose husband deserted her because he thought the IUD strings felt like a snake. The most frequently expressed rumour was that the IUD causes severe bleeding leading to excessive weight loss and ugliness, unlike the injectable which makes one bleed less and, therefore, leads to weight gain and beauty. Instances were cited where friends who had used the IUD felt dizzy and collapsed. There was even one death cited. Other rumours mentioned were that the IUD can cause heart disease or heart attack, infertility, offensive discharge, disease, irritation of the genital area, painful intercourse, burn the womb and lead to abdominal distension. One participant even thought the IUD, in causing abdominal distension, can then cause fibroids. There were also rumours that the IUD can shift (become displaced) and result into pregnancy, or that one can get pregnant even with the IUD in place, and that in such instances the baby may be born with it. Discussions with providers also confirmed that clients have many misconceptions about the IUD and its side effects. Clients believe that the IUD causes marital disharmony, abortion, that it can fail, and that it causes heavy bleeding, loss of weight and even death. Indeed, SC consultations exposed that providers were aware of these rumours since they made attempts to dispel them during interaction without being prompted. Eligibility criteria The 1999 Ghana National Reproductive Health Services Protocol (NRHSP)15 outlines the eligibility and non-eligibility criteria for the use of IUD and gives guidelines to be followed by service providers. It states that:
The NRHSP also emphasises that the IUD is not the first choice method for HIV positive women, and that the condom should be added to all methods. When asked about which category of women are eligible for IUD use, most providers said they would give the IUD only to women who have delivered before and to faithfully married couples or clients with single partners. Other categories of clients mentioned included women with normal menstrual flow, those who want long-term contraception but not sterilisation, any woman who chooses the IUD, and women who want to stop childbearing. Most providers frequently mentioned the category of nulliparous women as non-eligible. Certainly, some of the providers' views were the opposite of what the NRHSP recommends. Table 4 compares providers' views with the NRHSP eligibility and non-eligibility criteria. It was common for providers to discourage the use of IUD by nulliparous clients. In 22 of the 46 interactions where a nulliparous profile was presented, simulated clients were told they could not use the IUD. However, in almost all simulated interactions, clients did not have to ask providers about the IUD, but providers spontaneously discussed and explained about it. Reasons given for refusal included fear of attributing possible future infertility to IUD use and an assumption that nulliparous women have multiple partners and, therefore, are more likely to be at risk of infections. The IUD was also discouraged in three interactions involving older simulated clients because they were more than 35 years old and wanted to space childbearing. In one instance the simulated client was told: "You are already 35 and you want to space, but the IUD is for 10 years, by the time you remove it you will be in your menopause." For this reason a short-term method (i.e., the pill) was recom-mended. Almost all trainers, policymakers and programme managers interviewed were of the opinion that the IUD is a useful family planning method. One program manager stated: The IUD has a major role to play because it is a bridge between the permanent methods and the hormonal. The majority of providers interviewed viewed the IUD positively in the sense that it is the most cost-effective of all methods. They also said they would recommend it to their friends because it is non-hormonal, users have menses every month, and it is a safe and reversible long-term method. A few providers who stated that they would not recommend the IUD to a friend expressed concerns about the associated heavy and prolonged bleeding, which can lead to death. About half of the providers said they would use the IUD themselves. Those who would not use it cited reasons such as having unfaithful partners, preference for natural family planning and ineffectiveness of the IUD. Information Exchange with Simulated Clients Simulated client visits showed that providers mentioned a range of methods during all interactions. The IUD was mentioned in almost all interactions (147/159) and spontaneously mentioned in 123 of these instances. In 30 of the interactions, the SC felt that providers had over-emphasised some methods particularly the pill, condom, injection and Norplant. This practice was common in interactions that presented a nulliparous profile. Permanent methods were rarely discussed. Contraceptive samples were used as a visual aid in over half of all the interactions. The IUD sample was given to SC in 87 of 159 interactions. Providers nearly always asked the SC about their method preference (133/159) and when the SC expressed interest in the IUD, the providers' responses varied. In 87 of 159 interactions the providers said it was okay and in 28 of 159 the providers did not like their clients' method choice. Providers discussed the long-term use of IUD; most providers stated that the IUD could be used for a period of 10 years. In 12/159 interactions duration of use was not mentioned at all. However, several of the providers did not mention that IUD is an easily reversible method. Advantages of the IUD were mentioned in 61% (97/159) of the instances. The frequently mentioned advantages include long-term (90), effective (60), easy to use (59), and quick return to fertility (61). The providers also mentioned that IUD does not "mix with blood". Disadvan-tages were mentioned in 88 of the interactions. The commonly mentioned disadvantages include irregular or heavy menstrual bleeding, abdominal cramping, and pain during insertion and removal. None of the interactions included a discussion on STI/HIV. Dual Protection and Concerns about Transmission of STI/HIV Almost all the FGD participants had heard of STIs. The most frequently mentioned were HIV and gonorrhoea, and occasionally syphilis. Regarding their opinion on whether the IUD could protect against STIs, participants were aware that the IUD does not protect against these diseases. A few respondents had the misconception that injectable would protect against diseases as well, but many felt that the condom offers the best protection. All providers said they would treat the STI before giving IUD. When asked whether they would recommend the IUD to an HIV positive client, all except one provider said they would not give the IUD. Instead they would counsel the client and recommend another method. When asked what they worried most about during insertion of the IUD, most providers expressed fear about perforating the client's uterus (24/35), as compared to concerns about infecting themselves or the client (6/35). When asked specifically about the fear of being infected with HIV during insertion, about one third said they were concerned because the gloves could not be trusted; the disease is infectious and has no cure. Those who did not worry said they use sterile gloves and proper decontamination procedures. Contrary to this opinion, some programme managers and trainers said providers were not giving the service, mainly because of the fear of personal infection with HIV. Method Preference Regarding their opinion about shifting preferences, participants mentioned that they were not aware of this observation. They, however, suggested that the many side effects and rumours as well as fear of the method could partly be responsible for the observed shifting preferences. FGD participants also said the inability of IUD to protect against STI could be a possible reason for preference of other methods. One participant remarked: The condom is easy to use, you just get up and wear it. On the other hand the advent of AIDS makes wearing the IUD difficult since it only prevents pregnancy and not prevent disease, thus one needs a condom in addition. This is double and more expensive. A little over half of the providers were of the opinion that clients were switching from the IUD to other methods. Reasons cited include infections, misconceptions and the desire to try out new methods such as Norplant. In comparison to other long-term methods such as the implants and injectable, providers said that the IUD rarely featured as a first choice method among clients seeking long-term methods. Most programme managers and trainers lamented the poor product image and misconceptions; criticising the limited effort at dispelling rumours and the absence of product promotion through advertising as is done for other products. They also opined that there is a shift from IUD to the injectable. Some programme managers said the perceived risk of HIV infection to both clients and providers may be affecting the use of IUD. As commented: I think if they don't do something about the infection prevention measures the staff will not have the confidence to do it and if the staff don't have the confidence to do it they are not going to encourage clients. The other concern was that many sexually active people do not have single partners, and because of the risk of infection many would prefer to use the condom. Some programme managers argued that the complexities in service provision were an underlying factor. They mentioned that IUD insertion has many requirements, such as the need for sterilisation equipment and pelvic examinations. Some of the interviewees had this to say: You need the clinic setting, which makes IUD insertion inconvenient in the field. Unlike the injectable, which does not require too much sterilisation equipment. According to the National Policy and Standards, only midwives are trained to insert the IUD because of the need to sound the uterus. The type of IUD available (only Copper T380A) was also suggested as being responsible for declining use, since it has been associated with abnormal discharge. As explained by one respondent: I strongly believe so because people had IUD insertion for more than 20-25 years when it was the Lippe's and did not have much problem. But now it is not so. I have heard a few people complaining about some peculiar discharges with the copper ones, but I haven't seen any. Some service providers are saying that they think it is the IUD that is bringing about that type of discharge. IUD is not a preferred method. It was suggested that women do not like the IUD and that even those who use it have shifted to other methods. One programme manager remarked: The women themselves are rejecting it, so why do we want to force them? We have heard that Norplant, for example, is trying to take some of the IUD customers. Norplant does not have the associated infections and the heavy bleedings. Contextual Issues Training Although there are several institutions involved in family planning training, training in IUD insertion is limited to only a few institutions, namely, the Ghana Registered Midwives Association (GRMA); the Public Health Nursing School (PHNS), Accra; and three midwifery schools in Kumasi, Koforidua and Tamale. GRMA has identified three facilities in the country as training centres for the IUD. The other institutions run a four-week comprehensive family planning course with emphasis on IUD four times a year. The course is sponsored by UNFPA through the GHS. Table 9 shows the focus of training activities of the institutions. All 35 providers interviewed said they had had some sort of exposure to family planning training. However, only seven of them had attended the four-week comprehensive family planning course that places emphasis on the IUD. Out of the seven who had had the training, one had not done any insertions in the past year because of lack of demand for the method. One provider explained: The people here are not interested in IUD. They all prefer the injectable. Their minds are already made up before they come to the clinic. Fifteen out of thirty five providers interviewed had not done any insertions in the past year. Though a few said they did not need any training, many expressed the desire for refresher training to update their knowledge of IUD. Supplies and equipment The 1997 Ghana Situation Analysis (GSA) study of the family planning, which covered 313 service delivery points (SDP) across the country, shows that only 56% of the SDP were able to offer IUD. Supplies were available at 91% of these SDP and only 11% reported stock-out during the last six months. In this study, none of the facilities in the Greater Accra Region reported any shortage of IUD or related expendables (gauze, disinfectant, gloves) in the previous year. Out of the eight facilities visited in the Volta Region, only three offered IUD services, and only one of these had had shortages in the previous year. The remaining five facilities did not provide IUD services because of the absence of trained personnel at four facilities and the religious inclinations of a provider at one facility. In the Eastern Region all facilities visited provided IUD services and two had shortages in the previous year. The Copper T380A was the only type procured and distributed by the national FP programme. Cost Family planning services in Ghana are not free to clients. In view of this the GHS has standardised prices for the product. Pricing for related expendables is the responsibility of individual service delivery points. Simulated clients reported that they were asked to pay between 1000 and 20,000 Cedis to have an IUD inserted in public facilities, with an average cost of 10,000 Cedis (about US$1.22). At the private facilities the fee ranged from 30,000 to as high as 200,000 Cedis. Policy According to the National Population Council (NPC) and the Ghana Health Service (GHS) the current national policy is that family planning methods should be made accessible and affordable to all. The policy also embraces the concept of quality of care and emphasises giving information to individuals to enable them to make informed choices. The policy direction is for the public to have a wide range of choices with the public sector concentrating on long-term methods whilst the private sector deals with the short-term methods. However, in the context of STI/HIV and adolescent health needs, the actual practice is for both sectors (private and public) to promote condom use and dual protection. Regarding the IUD, the GHS position from the interviews conducted is that it is a method that is well tolerated by many women, and that it is also long-term and cost effective. The risk of infection is not high for women in monogamous relationships, but it increases if the partner is unfaithful. Thus, the GHS would not discourage the use of IUD, but then dual protection has to be promoted as well. One programme manager interviewed, however, challenged this position: I feel it's very democratic to have a full range of methods if you can afford it, but if you have limited resources that should also influence your choice. So we have to look at how much that extra method is going to cost per intercourse and find out whether it is cost-effective. So it depends on how much money you have, but personally I think we can minimise the range. What is the trade-off of the IUD? Is it just because it is cheaper? Demand creation Discussions with programme managers from two contraceptive promotion agencies about specific activity shift towards or against any particular method revealed that none of these agencies had a deliberate activity shift towards or against any particular family planning method. Rather, both agencies had broad and practical shifts shaped by the nature of their activities. For instance, one agency had shifted from providing family planning to the general population to targeting youth with reproductive health services and, therefore, focuses on condom and pills. Furthermore, Norplant and the injectable are considered convenient and cheaper to administer in the field because trained field assistants from mobile clinics can also provide them, thus, offering a greater possibility of reaching more people. Programme managers also admitted that they were limited in their efforts to promote IUD at the community level because of the complexities in service provision of the method. One source from a distributing organisation was of the view that the IUD will always have a place in the Ghanaian market because it is an effective, long-term, non-hormonal method, and there will always be clients who prefer it. However, there will be a continuous decline in its demand because of the availability of other competing products in the market. This competition, especially from Norplant, needs to be addressed. The organisation's opinion is that until a survey is done to find out what the "hot buttons" for IUD are, they are reluctant to go out and create a market for the product. Another major limitation mentioned was that IUD, unlike other products, is unbranded, yet in social marketing the need to identify with "your" product is overriding. Thus, it is considered difficult to disseminate information on the use of the IUD or even to carry out targeted market studies. For instance, condoms and injectables have been promoted because they are branded. As stated by one programme manager, it then becomes "ours" and can, therefore, be easily monitored. Examples of such brand names mentioned include the "Famplan" pill and the "Champion" condom. Discussion The Role of Community Perceptions on the Use of IUD The findings identified several community perceptions and misperceptions about the IUD that seem to contribute to its declining trends in Ghana. The perceptions, which were mostly negative, were mainly from potential clients. Many of these clients, though, had never used or even seen the IUD, but had heard many rumours and speculation about it. Rumours about IUD, therefore, discourage its use and it is important that efforts are made to dispel them. The design of the product itself contributed to the negative image, inducing fear and apprehension in some women, as seen from the comments made by the focus group discussion participants. The design gives credence to the speculation that it could cause harm to the body. The side effect of excessive bleeding and weight loss associated with the use of the IUD is a real disincentive. This may contribute significantly to shifting client preferences away from IUD to other methods such as the injectable, which coincidentally has the side effect of amenorrhoea and proven weight gain. Information from the focus group discussions show that, socially, weight loss is associated with unattractiveness while weight gain is associated with beauty. This belief promotes the increased use of injectable against IUD. There appears to be real competition from the injectable, which has the added advantage of having a preferred route of administration. The injectable is also popular because it is thought to be medicinal, due to its mode of administration, and the fact that it gets into the blood circulation. On the contrary, IUD does not "mix with the blood", as stated by a focus group participant. The concern expressed about IUD irritating the sexual partner featured prominently and it justifies an exploration of the subject, probably through interviews with men who have partners using IUDs. Provider Attitudes Contrary to the general belief that providers' bias against IUD may contribute to the decline in use, these findings show that providers generally have a favourable attitude towards the IUD. They offer it as one of the options to clients and actually attempt to dispel associated rumours. Moreover, the assertion made by programme managers/trainers that fear of contamination during IUD insertion could prevent providers from recommending the method, is not correct. Providers' fears had mainly to do with harm to the clients during insertion rather than to themselves. This suggests that providers may not be confident of their insertion skills. If indeed providers worry about having to conduct a vaginal examination before inserting the IUD, then what about other similar situations such as delivery. Provider bias was found to be in relation to parity. Providers admitted that they would not give the IUD to nulliparous women, including adolescents. This practice is contrary to the National Reproductive Health Protocols, which states that: The IUD (Copper T) is eligible for all women, but for nulliparous women, particularly adolescents, the IUD is not the first choice. Thus, providers are not exactly acting within the guidelines, denying adolescents and nulliparous women access to a method that offers important advantages over other forms of contraception — it is non-hormonal and long-term, requires minimal compliance, and return to fertility is immediate. The NRHSP guidelines categorically stated that pregnancy is an absolute contraindication for IUD use. This may explain why providers insisted on excluding pregnancy in simulated clients before providing the method. The findings also show that providers give clients information about side effects of the method only if the client is eligible for it. No such information is given to non-eligible clients. According to the protocol, providers are expected to take a full history of the client before conducting a physical examination. However, in practice, it appears that providers do not take full history before recommending or discouraging the use of a method. Considerations for Dual Protection According to the national reproductive health service protocols, the IUD is not a first choice for HIV positive clients. The use of the condom together with another family planning method is recommended. This position is also in accordance with WHO recommendations, which state that insertion of the IUD in an HIV-infected woman or one who is at high risk of infection is not usually recommended. However, a study in Kenya has raised questions about these guidelines.9 The study found that there were no more overall complications following insertion in HIV-infected women than in uninfected women. The national STI/HIV control policy document is, however, silent on the use of IUDs in HIV-positive patients. It is also important to examine the impact of accelerated promotion of the condom in the context of STI/HIV/AIDS control on the information provided on other contraceptive methods including the IUD. This is because respondents raised concerns about the cost implications of dual protection. Given that the condom is not as effective a contraceptive and a back-up is essential, there is need to educate prospective clients on the importance of dual protection. In promoting the condom, there is need for education on the proper use of male and female condoms. Pairing the two for sale by some chemical shop owners, as mentioned, could give a wrong message that the two could be used simultaneously. This practice should be discouraged. Service Delivery System Barriers Several barriers at the service delivery level have been identified that may restrict clients' access to IUD. These include training, cost of the IUD, demand generation/promotion, logistics and supplies. IUD pre-service training for nurses and midwives appears to be inadequate, as it is limited to general training and most providers may not have the opportunity to perform any insertions, because the IUD is a low caseload method. Some providers who said they could not provide the service because they had not been adequately trained confirmed this assertion. IUD insertion is a skill requiring practice, thus, even for those trained a low caseload at the service delivery point could result in many losing the skill. There may be a need to revise the policy requirement that only trained midwives can insert the IUD. This requirement blocks nurses who qualify without having done midwifery and are, therefore, not allowed to perform pelvic examinations. This includes male nurses and nurses specialised in public health. Those who had attended family planning training said they had no confidence inserting the IUD. They had not been allowed to make any practical insertion during their course since they were not midwives. Ultimately, this limits access to the method. The information on providers' experience, which this study tried to obtain based on the number of insertions performed, was distorted because most of the providers reported on insertions by the facility and not about their personal experience. It is important that providers sign for insertions that they have personally done. This would be useful in cases of clinical audit (e.g., evaluation, tracing responsibility for complications) and for improving record-keeping. What is clear, however, is the fact that less than a quarter of providers interviewed had attended the four-week comprehensive training for the IUD, which from interviews appears to be the main in-service course, and which offers the opportunity to acquire practical insertion skills. The average cost of having an IUD inserted in public facilities was found to be 10,000 Cedis (about US$1.22). This amount, when compared to the method's 10-year lifespan, is cost effective. In contrast, the injectable costs about 2000 cedis, but has to be administered four times a year, giving a total cost of about 80,000 Cedis for a 10-year period. Thus, in real terms the cost of IUD should not be a barrier to use. However, it is possible that prospective clients find it easier paying 2,000 Cedis upfront than 10,000 Cedis, making the IUD more expensive in that instance. It is also not clear how many couples consider the cost of contraception beyond the time of purchase.5 Also, the price range of 30,000 to 200,000 Cedis reported from private facilities raises some concern and may be a real barrier to access. The general impression from the discussions is that family planning service agencies have more experience in promoting short-term than long-term methods, thus, a significant proportion of their time is spent providing these methods. This is worsened by the complexity of service provision in the case of the IUD in particular, as well as the unbranded nature of the product. The advent of HIV seems to have aggravated the problem by giving impetus to condom promotion. Even agencies such as the Ghana Health Service, who had the original responsibility for promoting IUD, have intensified their efforts in condom promotion. Both the public and private sectors should give equal attention to the IUD to make it attractive to prospective clients. Branding the product may also improve marketing and promotion.
Acknowledgements The authors acknowledge the support received from the Health Research Unit and the Reproductive and Child Health Unit, Ghana Health Service and Frontiers in Reproductive Health Program, Population Council. This study was funded by the United States Agency for International Development (USAID) under the terms of Cooperative Agreement Number HRN-A-00-98-00012-00 and the Population Council Sub-agreement Number AI02.06A. The opinions expressed herein are those of the authors and do not necessarily reflect the views of USAID. References
Copyright 2005 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh05027t2.jpg] [rh05027t1.jpg] [rh05027t4.jpg] [rh05027t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}