 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
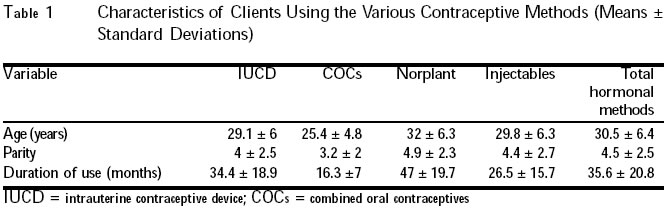
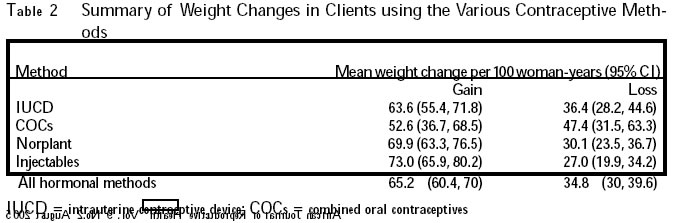
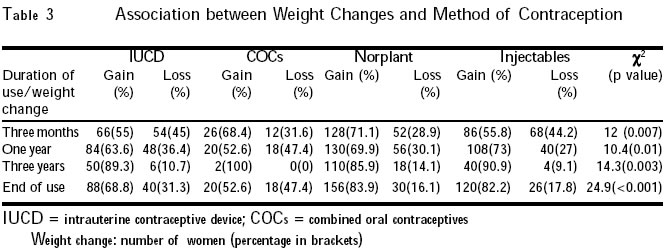
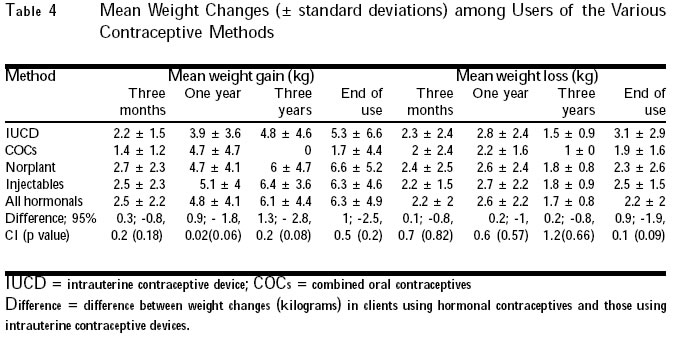
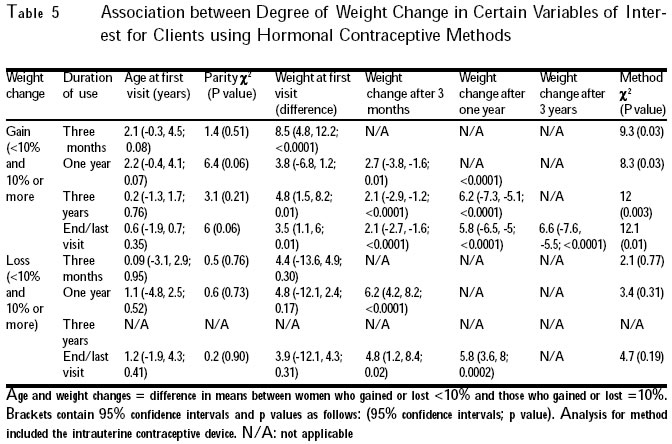
African Journal of Reproductive Health, Vol. 9, No. 2, August, 2005, pp. 92-100 Weight Changes in Clients on Hormonal Contraceptives in Zaria, Nigeria Saadatu Sule and Oladapo Shittu Correspondence: Saadatu Sule, Department of Obstetrics and Gynaecology, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria. saasule@yahoo.com Code Number: rh05028 Abstract Misconceptions exist in Nigeria about the effects of hormonal contraceptives on weight, which may have negative effects on contraceptive use. Data from case notes of clients attending the reproductive health centre at the Ahmadu Bello University Teaching Hospital, Zaria, between 1993 and 1995, were analysed to determine the effects of hormonal contraceptives on body weight, comparing them to clients using intrauterine contraceptive devices. Weight changes were not significantly different in clients using hormonal contraceptives and those using intra-uterine contraceptive devices. This information will be beneficial in contraceptive counselling for clients in this environment and provide a baseline for further research. (Afr J Reprod Health 2005; 9[2]: 92-100) Résumé Il existe des idées erronnées au Nigéria concernant les effets des contraceptifs hormonaux sur le poids, chose qui pourrait avoir des effets négatifs sur l'usage des contraceptifs. Les données recueillies des dossiers des clientes qui fréquentaient le centre de santé de la reproduction au Centre Hospitalier Universitaire Ahmadu Bello à Zaria, entre 1993 et 1995, ont été analysées pour déterminer les effets des contraceptifs hormonaux sur le poids corporel, en les comparant aux clientes qui utilisent les dispositifs inter-utérins comme méthodes contraceptives. Il n'y avait pas des différences importantes en ce qui concerne les modifications de poids chez les clientes qui utilisent les contraceptifs hormonaux et ceux qui utilisent les dispositifs intra-utérins. La consultation contraceptive profitera de ce renseignement pour les clients de ce milieu et fournira une ligne de base en vue d'une recherche plus approfondie. (Rev Afr Santé Reprod 2005; 9[2]: 92-100) Key Words: Contraception, weight, counselling Introduction Hormonal agents are the most popular and most effective non-surgical methods of contraception in the world.1 The most popular of these methods is the combined oral contraceptive pill, although in Nigeria and Africa as a whole, the injectable hormonal contraceptives are very popular especially among clients seeking terminal contraception.1,2 Both weight gain and weight loss may occur with hormonal contraceptives. Weight gain, weight loss, or no change in weight may occur with oral contraceptives,3-5 injectable contracep-tives,6-12 and progestogen contraceptive implants.13-15 Clients using the Norplant subdermal implants in Zaria have previously been reported to gain a mean of 0.3kg after one year of use, and 1.1kg after five years, or lose a mean of 0.2kg after three years.15 Among oral contraceptive users, weight gain was more likely to occur in women who were underweight at initiation of therapy as compared to those who were initially overweight.3 Oral contraceptives containing lower doses of hormones are less likely to be associated with weight gain.3,4 Weight gain among users of depo medroxyprogesterone acetate is only slightly less in clients who were initially overweight.8 Cyclofem, which is a monthly combined oestrogen and progestogen injectable contraceptive, is associated with greater weight gain among those who initially were underweight.16 Clients who gain 5% or more of their baseline weight after three months of contraceptive use are more likely to gain even more weight after one year of use.6 Weight gain occurs more in association with use of injectable hormonal contraceptives as compared to oral contraceptives.5 Although weight changes are usually classified as minor side effects, excessive weight gain may increase the risk of cardiovascular and metabolic side effects of hormonal contraceptives.8,17 Both weight gain and weight loss are associated with poorer physical and psychological well being18,19 particularly in adolescents and young adults who are usually pre-occupied with body image.4,20 Weight loss may be associated with increased incidence of minor side effects of oral contraceptives such as menstrual cramps and menstrual irregularities, nausea, and breast discomfort, which have been reported to occur more frequently in underweight women.3,21 The incidence of amenorrhoea has been found to be higher in overweight than in underweight women or those of normal weight.10 The weight gain associated with these contraceptives may be responsible for the increasing incidence of amenorrhoea with continued usage.10 The aim of this study was to determine the effect of hormonal contraceptives on the body weight of clients at Ahmadu Bello University Teaching Hospital, Zaria, and factors associated with these weight changes, with a view to providing accurate information during contraceptive counselling. It would also help in reducing the misconceptions that exist in this environment about these methods and in reducing the discontinuation rates due to weight changes, as clients would be better informed. Methods The setting was the reproductive health centre at Ahmadu Bello University Teaching Hospital, Zaria. The study was a retrospective analysis of data that were obtained from the case notes of all new clients who registered at the family planning clinic between January 1, 1993 and December 31, 1995, to allow for a follow-up period of up to five years for each client. Those who used hormonal contraceptives (combined oral contraceptives, depo medroxyprogesterone acetate, norethisterone enanthate and Norplant) and were followed-up for at least one year made up the subjects. Clients who use barrier methods do not have any regular follow-up schedule, they usually return to the clinic when their supply has run out or when they have other problems. Those who have bilateral tubal ligation are seen one week after the procedure and then four weeks later, and discharged if they have no problems. The follow-up schedule meant that only clients who used intrauterine devices could be included as controls. The controls were, therefore, clients who used intrauterine contraceptive devices and were followed-up for at least one year. Clients who were followed-up for less than one year and those who did not select any method were excluded from the analysis. Information were obtained from the case notes on age; parity; method of contraception used by the client; date of commencement; duration of use; history of illness between follow-up visits; weight before commencement of the contraceptive; weight changes after three months, one year and three years of use; and weight at the time of discontinuation of the method. Height was recorded in the case notes for less than 30% of clients, making it difficult for meaningful analysis of body mass index. Statistical analyses, including rates and comparative analyses, were carried out on the data obtained using the appropriate computer statistical software including MINITAB, SPSS and Microsoft EXCEL. Results A total of 1,131 new clients registered during the study period, out of which 516 met the selection criteria and were included in the analyses. Of the 516, 136 used the intra-uterine contraceptive device and these made up the controls. Clients using hormonal methods of contraception included 38 who used the combined oral contraceptives, 188 who used the Norplant subdermal implants and 154 who used injectable contraceptives (depo medroxyprogesterone acetate and norethisterone enanthate). The remaining 615 clients were excluded from the study due to follow-up periods of less than one year. Of these, 216 used the intra-uterine contraceptive device, 106 used the combined oral contraceptives, 151 used Norplant and 142 used the injectable contraceptives. A summary of the characteristics of clients on the different methods of contraception is shown in Table 1. None of the clients included in the study had any medical disorder and none reported any illness, apart from malaria and upper respiratory tract infections, between follow-up visits. The weight changes per 100 woman-years for clients using the various contraceptive methods are shown in Table 2. The difference in weight changes per 100 woman-years among clients using hormonal methods and intrauterine contraceptive device was not statistically significant as evidenced by the 95% confidence intervals. There was a significant association between contraceptive method and weight change at three months, one year, three years and end of use. After three months of use, weight loss was more common among clients using the intrauterine contraceptive device than in those using hormonal methods, while those using hormonal contraceptives were more likely to gain weight than those using the intrauterine contraceptive devices. After one year, and at the end of use, weight gain was less common among clients who used combined oral contraceptive pills as com-pared to other methods. However, weight gain was still more common among those who used the other hormonal contraceptives, as compared to those who used the intrauterine contraceptive device. Details are shown in Table 3. Weight change was significantly associated with duration of use; weight gain being more likely in clients who had used the contraceptive for longer periods. The difference in mean duration of use between clients who gained weight and those who did not was 9.8 months, 95% confidence interval = 5.8, 13.9, and p < 0.0001. Of the 516 clients, weight gain occurred in 306 (59.3%) after three months of contraceptive use, 340 (65.9%) after one year, and 384 (74.4%) at the end of use/last visit. Only 236 clients were followed-up for up to three years after commen-cement of contraceptive use, and of these, 200 (84.8%) gained weight. Of those who gained weight after the various durations of contraceptive use, weight gain was less than 10% of initial weight in 278 clients (90.8%) after three months of contraceptive use, 296 (87.1%) after one year, 124 (62%) after three years, and 224 (58.3%) at the end of use/last visit. On the other hand, weight gain was 10% or more of initial weight in 28 clients (9.2%) after three months of use, 44 (12.9%) after one year, 76 (38%) after three years, and 60 (41.7%) at the end of use/last visit. Weight loss occurred in 186 clients (36.1%) after three months of contraceptive use, 164 (31.8%) after one year, and 114 (22.1%) at the end of use/last visit. Of the 236 patients followed-up for three years, 30 (12.7%) had lost weight. Of those who lost weight, weight loss was less than 10% of initial weight in 178 clients (95.7%) after three months, 152 (92.7%) after one year, 30 (100%) after three years, and 104 (91.2%) at the end of use/last visit. Weight loss was 10% or more of initial weight in eight clients (4.3%) after three months of contraceptive use, 12 (7.3%) after one year, and 10 (8.8%) at the end of use/last visit. No weight change occurred in 24 clients (4.7%) after three months of contraceptive use, 12 (2.3%) after one year, 6 (2.5%) after three years, and 18 (3.5%) at the end of use/ last visit. Of clients who did not have any weight changes after three months of contraceptive use, 16 (66.7%) were intrauterine contraceptive device users, while 8 (33.3%) were Norplant users. After one year of use, those who did not experience any weight changes consisted of six injectable contraceptive users (50%), four intrauetrine contraceptive device users (33.3%), and two Norplant users (16.7%). After three years of use, no weight change occurred in six clients, four intrauterine contraceptive device users (66.7%) and two Norplant users (33.3%). At the end of use/last visit 18 clients including eight intrauterine contraceptive users (44.4%), eight injectable contraceptive users (44.4%), and two Norplant users (11.1%) experienced no weight changes. Mean weight changes for each of the methods are shown in Table 4. Table 5 shows the association between the degree of weight change (< 10% and = 10% of the initial weight) and variables of interest in clients using the hormonal methods of contraception. The mean initial weight was significantly higher (60.7kg) among clients who gained less than 10% of their initial weight after three months of use, compared to the initial weight (52.2kg) in clients who gained 10% or more of their initial weight. Similarly, the mean initial weight was significantly higher after one year of use (62.6kg compared to 58.9kg), after three years of use (63.1kg compared to 58.3kg), and at the end of use/last visit (61.7kg compared to 58.2kg), in clients who gained less than 10% of their initial weight. Significant weight gain after three months, one year and three years of contraceptive use was significantly associated with weight gain of 10% or more of initial weight subsequently. Weight loss of 10% or more of initial weight after one year of contraceptive use and at the end/last visit was significantly associated with greater weight loss after three months of use, as compared to weight loss of less than 10% of initial weight. Weight loss of 10% or more of initial weight at the end of use/last visit was also significantly associated with greater weight loss after one year of use. Weight gain of 10% or more of their initial weight was most common among clients using Norplant after three months (48.5%), one year (64.3%), three years (57.9%), and at the end of use/last visit (45%). Among clients using injectable contraceptives, 30.4%, 28.6%, 29% and 36.3% had gained 10% or more of their initial weight after three months, one year, three years and at end of use/last visit. Among intrauterine contraceptive device users, 16.4%, 7.1%, 13.2% and 15% gained 10% or more of their initial weight after three months, one year, three years and at end of use/last visit. Weight gain of 10% or more of initial weight occurred only after three months of use (4.7%) and at the end of use/last visit (3.8%) among clients using the combined oral contraceptive pills. These differences in weight changes among clients using the different contraceptive methods were statistically significant as shown in Table 5. Discussion The mean age and parity of family planning clients in this study were similar to what has been reported by other researchers.2,7,22 The lowest mean age and parity occurred among clients using the combined oral contraceptives, and these factors probably accounted for the observation that this group of clients had the shortest mean duration of contraceptive use, as such clients would be more likely to be desirous of further conception. Weight changes occurred in clients on both hormonal and non-hormonal contraceptives though weight gain occurred more commonly among clients on hormonal contraceptives, while weight loss was less common in this group of clients. Weight gain occurred in 65.2% of clients after one year of use of the hormonal methods. This is similar to figures reported in previous studies.8,10 There was no significant difference in the proportion of clients and controls that gained weight as reported previously.4,12,14 The injectable contraceptives were associated with greater likelihood of weight gain and lower likelihood of weight loss as compared to the intrauterine contraceptive device. This is in keeping with some reports that have found greater likelihood of weight gain in clients using the injectable contraceptives as compared to other methods,5,9 although other researchers have reported no association between the injectable contraceptives and weight gain, as compared to other methods.11,12 The combined oral contracep-tives were least likely, among the hormonal contraceptives, to lead to weight gain as has been reported previously.4,5 Clients using Norplant were more likely to gain weight than those using the combined oral contraceptives, but when compared to other methods of contraception, Norplant was not significantly associated with weight gain. Some previous reports also did not find any significant association between Norplant use and weight gain.13-15 The amount of weight gained was significantly associated with the method of contraception with clients using Norplant or the injectable contraceptives being more likely to gain 10% or more of their initial weight. An association between the degree of weight gain and the method of contraception has also been reported in previous studies.5,10 A similar association between weight loss and the method of contraception was absent. There was no association between weight change and age or parity in clients using the hormonal methods of contraception as has been reported previously.5,9,10 Higher initial weight (60kg or more) was significantly associated with lower weight gain in this study, in keeping with findings of other studies,3,8,16,21 although other researchers did not find such association.5 Weight loss was not significantly associated with mean initial weight. Weight changes were significantly more likely to occur with longer duration of hormonal contraceptive use probably due to a cumulative effect of the contraceptive on the system over time. However, some studies found no significant weight change even with long-term contraceptive use.12-15 The mean weight changes were not significantly different in clients using the hormonal methods and those using the intrauterine contraceptive device. The mean weight gain in clients using the hormonal methods of contraception was 2.5kg, 4.8kg, 6.1kg and 6.3kg after three months, one year, three years and at the end of use/last follow-up visit respectively. The mean weight loss in clients using the hormonal methods of contraception was 2.2kg, 2.6kg, 1.7kg and 2.2kg after three months, one year, three years and at the end of use/last follow-up visit respectively. These changes lie within the mean ranges of weight gain (0.2-9kg over three months to five years)8-10,15,21,23 and weight loss (0.6kg to 1.8kg over one to five years)10,15 that have been reported previously. Clients who gained weight after three months of contraceptive use were more likely to gain weight at one year, three years and at the last visit/end of use. A similar pattern was also observed for weight loss. This suggests that the pattern of weight change during hormonal contraceptive use is likely to continue with continued use. Previous studies have reported weight gain at three months as being a risk factor for further weight gain with continued use.5,16 Clients being counselled for contraception should be informed that hormonal methods do not cause significant weight changes when compared to other methods. However, they should also be informed that weight gain amounting to 10% or more of their initial weight is more likely with the injectable contraceptives and the Norplant subdermal implants. Clients should be informed of the greater likelihood of weight gain if their initial weight is less than 60kg, though this depends on their body frame and height. They should also be informed that whatever weight change they experience is likely to be maintained with continued use of the method. The importance of regular exercise and balanced diets in maintaining their desired weight should be emphasised. There is a need for prospective study of weight changes in clients on the various methods of contraception in this environment, using the body mass index to assess whether clients become obese or underweight due to weight changes, which was not possible in this retrospective analysis due to unavailability of height measure-ments for the majority of patients. A prospective study would also have improved follow-up rates and avoid bias that may arise as a result of poor follow-up rates. References
Copyright 2005 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh05028t4.jpg] [rh05028t3.jpg] [rh05028t5.jpg] [rh05028t1.jpg] [rh05028t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}