 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 9, No. 2, August, 2005, pp. 101-106 Concurrent Use of Multiple Antenatal Care Providers by Women Utilising Free Antenatal Care at Ebonyi State University Teaching Hospital, Abakaliki Sunday Adeoye1, LU Ogbonnaya2, OUJ Umeorah1 and O Asiegbu1 Departments of 1Obstetrics & Gynaecology, and 2Community
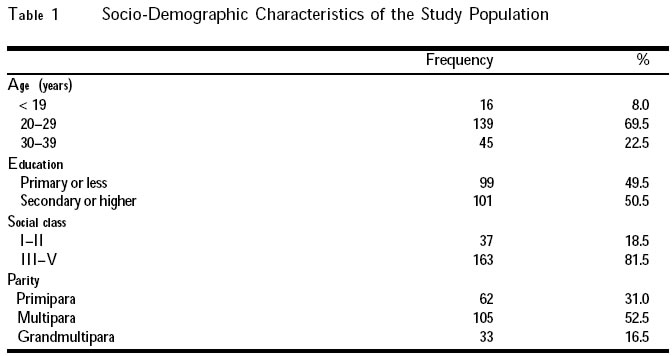
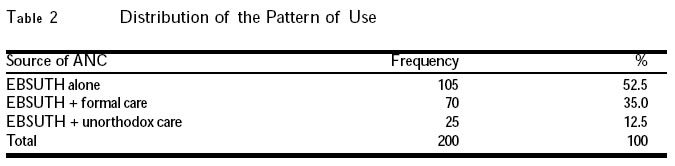
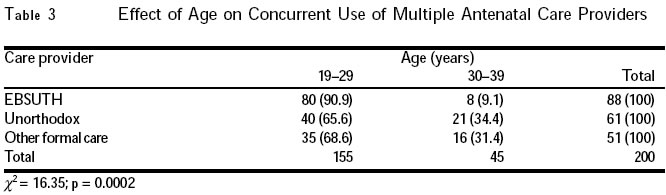
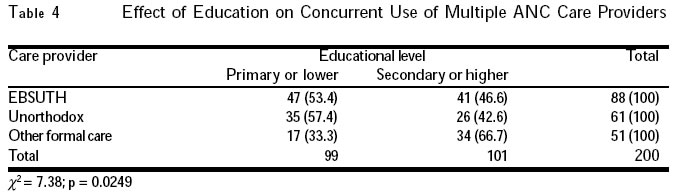
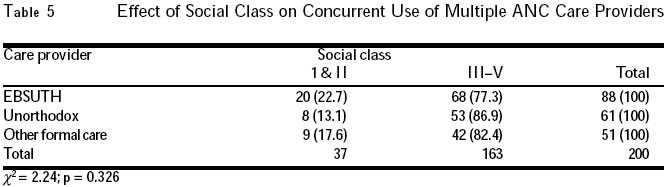
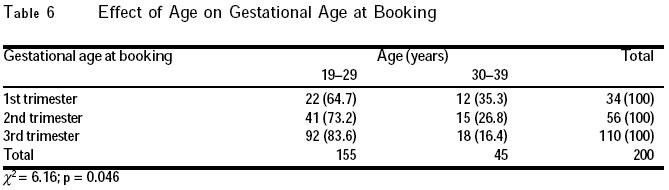
Medicine, Ebonyi State University Teaching Hospital, Abakaliki Code Number: rh05029 Abstract Observation has revealed that women who book at Ebonyi State University Teaching Hospital, Abakaliki, concurrently use multiple antenatal care givers (formal and non-formal). This study was therefore conducted to identify the other sources of antenatal care for the women and to examine them in relation to their socio-demographic characteristics. A total of 200 antenatal women chosen from two randomly selected booking clinics were interviewed using a structured questionnaire. The results show that 25% and 30.5% respectively from the two clinics were concurrently using formal and unorthodox ANC givers. Age and education were significantly related to the practice (p < 0.0002 and p < 0.02 respectively). These findings suggest that free services alone may not be enough to make women attend ANC in the hospital. A larger study, especially investigating patient's perspective of the quality of care, is recommended. (Afr J Reprod Health 2005; 9[2]: 101-106) Résumé L'observation a révélé que les femmes qui s'inscrivent auprès du Centre Hospitalier Universitaire de l'état d'Ebonyi à Abakaliki se servent en même temps des fournisseurs des services prénatals multiples (officiels ou non-officiels). Cette étude a été menée donc pour identifier les autres sources de soin prénatal pour les femmes et de les examiner par rapport à leurs caractéristiques socio-démographiques. Au total, 200 femmes prénatales selectionnées de deux cliniques d'inscription selectionnées au hasard, ont ont été interviewées à l'aide d'un questionnaire structuré. Les résultats ont montré que 25% et 30,5% respectivement de deux cliniques se servaient en même temps des fournisseurs officiels de soins prénatals. L'âge et l'instruction ont été droitement liés à la pratique (p<0,0002 et p<0,02 respecitivement). Ces résultats montrent qu'il ne suffit pas que les services soient gratuits pour que les femmes aillent à la consultation prénatale qui se trouve à l'hôpital. Nous préconisons une étude plus élargie qui mettra l'accent sur la manière dont la patiente perçoit la qualité du soin. (Rev Afr Santé Reprod 2005; 9[2]: 101-106) Key Words: Antenatal, Care, Women, Clinic Introduction Antenatal care has evolved since its introduction at the turn of the century to become an essential part of standard obstetric care. It provides education, support and re-assurance for mothers with uncomplicated pregnancies.1 It has as one of its cardinal objectives, the identification of high risk patients for closer management. Regrettably the provision of antenatal services has not translated to an improvement in maternal and perinatal mortality rates in Nigeria. This has been related to several factors, including poor quality of care by service providers.2 In Nigeria, there is a problem of inadequate antenatal care facilities, and pregnant mothers have had to travel long distances to access the available centres. This factor has continued to encourage the utilisation of quacks and poorly trained traditional birth attendants who reside in the community and who enjoy the confidence of the people.3 Where antenatal facilities exist, utilisation is often far from optimal,4,5 and several reasons may account for this behaviour. These include poor socio-economic status of the patient, cultural beliefs, high cost of antenatal services and undue delay in the provision of services.4-6 Some studies have also shown that many of our pregnant mothers may receive antenatal care but would still choose to deliver at home with the traditional birth attendant and in spiritual churches.3,5,9,10 Data from the Ebonyi State University Teaching Hospital reveal that with the introduction of free antenatal and delivery services in 2001, there has been a steady rise in the utilisation of antenatal facilities from 599 women in 2000 to 1284 in 2001 and 3254 women by October 2002. The corresponding delivery rates for the periods were 354, 606 and 1536 respectively. This improvement in utilisation suggests that cost is an issue in the utilisation of antenatal facilities. Also, it indicates that several other factors are considered by the pregnant mother in deciding where to deliver rather than just the provision of free delivery services. Less than 50% of the women who sought antenatal care with the centre actually delivered there in spite of the free antenatal and delivery services provided. This curious obser-vation calls for an elaborate study in the centre. The unacceptably high maternal mortality figures in the country has been partly attributed to unbooked obstetric emergencies, and serious attempt to reduce maternal deaths should also address factors that create unbooked emergencies.11 This is in addition to the provision of accessible, affordable and effective antenatal facilities. Material and Methods This study was carried out at the Ebonyi State University Teaching Hospital, Abakaliki (EBSUTHAI). EBSUTHAI is a state-owned tertiary referral centre situated in Abakaliki, capital of Ebonyi State. It is a 300-bed hospital with a total of 188 doctors. The Obstetrics and Gynaecology Department, which houses the antenatal clinics, has a total of seven consultants and 14 resident doctors. There are 20 nurses and other supporting paramedical staff. Antenatal booking clinic is held once a week (every Wednesday) whereas antenatal care clinics run every working day of the week except on Wednesday. Available statistics show that with the introduction of free maternity care services in the state, antenatal booking rates increased from 559 in the year 2000 to 3254 by the end of October 2002. Correspondingly, the delivery rates increased from 354 in 2000 to 1536 by the end of October 2002. Maternal mortality rate for the hospital within the same period stands at 700/ 100,000 live births. The inhabitants of the state are mainly farmers, traders and civil servants. Sampling and Sample Size The sample size was limited because of the exploratory nature of the study. Two hundred women were selected from two randomly selected booking clinics in September and October 2003. The sample is, therefore, a total population of the booking clinics chosen. Informed consent was obtained from the patients. Data Collection Data were collected using interviewer-adminis-tered pre-tested structured questionnaire. Two independent health workers who were natives translated the questionnaire from English to vernacular and back to English. This was further pre-tested amongst few patients in another booking clinic. The result of the pre-test was used to prepare a final draft of the questionnaire. The interviewers who were doctors in the department were trained for one day. The training consisted of reading items on the questionnaire and finding out from each of them what the item sought to establish. After editing and coding, data were entered into an IBM compatible personal computer and analysed using the Epi-Info version 6.0 statistical package. Chi-square statistic was used to compare proportions. Significance level was set at p < 0.05. Results Socio-Demographic Characteristics of the Patients Sixteen (8%) of the mothers were teenagers aged less than 19 years, 139 (69.5%) were aged 20-29 years, while 45 (22.5%) were aged 30-39 years. Almost half (49.5%) of them had no formal or primary education, while 101 (50.5%) had secondary education or more. A preponderant proportion (81.5%) came from the lower social classes (social classes III-V) while 37 (18.5%) came from social classes I & II. Amongst the study population, 62 (31%) were primipara, 105 (52.5%) were multipara, while 33 (16.5%) were grandmultipara (Table 1). Concurrent Use of Multiple ANC Sources The result also shows that 105 (52.5%) of the subjects were utilising EBSUTH antenatal clinic only in their present pregnancy, 70 (35%) were utilising EBSUTH and another formal care establishment, while 25 (12.5%) were utilising EBSUTH and an unorthodox source (Table 2). Age and education significantly influenced concurrent use of multiple care centres (χ2 = 16.35; p = 0.0002 and χ2 = 7.38; p = 0.02 respectively) while social class did not (χ2 = 2.24; p = 0.326) (Tables 3, 4 and 5). Gestational Age at Booking Thirty four (17%) of the women booked during their first trimester, 56 (28%) booked in the second trimester, while 110 (55%) booked in the third trimester. Age was related to the gestational age at booking, as a significantly lower proportion of women aged 30-39 years booked in the late stages (second and third trimesters) compared to the younger women (χ2 = 6.16; p = 0.046) (Table 6). Discussion Findings from this study show that in spite of the free antenatal and delivery services offered at EBSUTHAI, a high proportion (47.5%) of the study population were concurrently utilising multiple sources of care. About 37.5% of the study population utilised other sources that were fee-paying in addition to the free antenatal care at EBSUTHAI. This suggests that free services alone may not be the incentive for optimal utilisation of antenatal care. It would be necessary to probe the factors that make these patients to seek care at fee-paying centres outside the teaching hospital. The scope and design of the present study could not unravel these hidden factors. The findings suggest that the policy of free antenatal services for all patients may not be appropriate, as some women could afford a fee-paying service. Such policy could be beneficial and cost-effective if some discriminatory measures could be employed to identify those (mostly the rural and urban poor) who actually need the free service, thus sieving out those who do not need it. A significantly higher proportion of the women aged 19-29 years used EBSUTHAI alone compared to the older age group. This may be because the age group constituted the majority of the study population. Also, education significantly affected use of other forms of formal health care, as a significantly higher proportion of those with secondary education and above used other formal health care sources concurrently with EBSUTHAI, compared to EBSUTHAI alone or EBSUTHAI plus unorthodox care givers. Higher education is likely associated with higher paying jobs and, therefore, ability to afford the fees in these other places. However, paradoxically, social class did not affect concurrent use. Two thirds of women in the study were multiparous and grandmultiparous, a finding that is similar to that reported from Ethiopia.3 The low number of nulliparous patients booking suggests that these groups of women may be utilising non-formal forms of antenatal care. There seems to be a cultural aspect to this finding. Women, especially those in the rural parts of the country, are expected to prove their womanhood by delivering at home, thus making them to shun orthodox medical care during pregnancy. A large proportion of the patients booked in the third trimester, which is consistent with earlier reports.2,4 The women booked late for ANC probably because they were already receiving some formal and non-formal care elsewhere. The timing of booking was influenced by the age of the patient, as more women aged 20-29 years booked in the third trimester. Surprisingly, the level of education did not appear to influence the gestational age at booking. This unexpected finding may be due to the limited sample size. The finding of a larger proportion of women seeking antenatal care late in the establishment where services are free may be due to lack of adequate information about availability of free services. Some of them may also not believe in the usefulness of antenatal care in a tertiary centre, hence their presentation only for "insurance" booking — in case they develop complications while labouring elsewhere. A quarter of the study population was already receiving antenatal care from other formal sources before presentation at the centre for antenatal booking. This probably explains why they presented late for ANC booking at the tertiary centre. The practice of making multiple antenatal bookings may also be responsible for the vast difference between the number that booked for antenatal care in the hospital and the number that actually deliver there. We conclude that despite the free antenatal and delivery services rendered in EBSUTH, many women attending the antenatal booking clinic concurrently utilise other formal and non-formal sources of antenatal care, many of which are fee-paying. Free services may not, therefore, be the only factor affecting utilisation of antenatal care services at EBSUTH. We recommended that a larger and broader study that will include a probe of patients' perspective of the maternity services received at EBSUTH be conducted to validate this finding. This will have an important policy impact on the implementation of government's free antenatal and delivery services. References
Copyright 2005 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh05029t4.jpg] [rh05029t3.jpg] [rh05029t6.jpg] [rh05029t5.jpg] [rh05029t2.jpg] [rh05029t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}