 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 9, No. 2, August, 2005, pp. 107-117 Province of Residence and Active Syphilis Infection among Zambian Men and Women: New Evidence from Population-Based Data AM Powell, G Seage and U Larsen Department of Population and International Health, Harvard
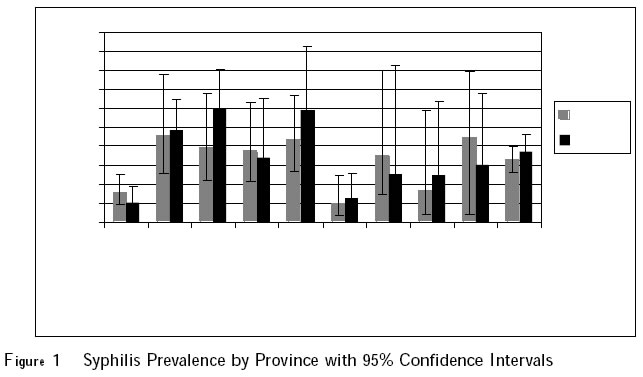
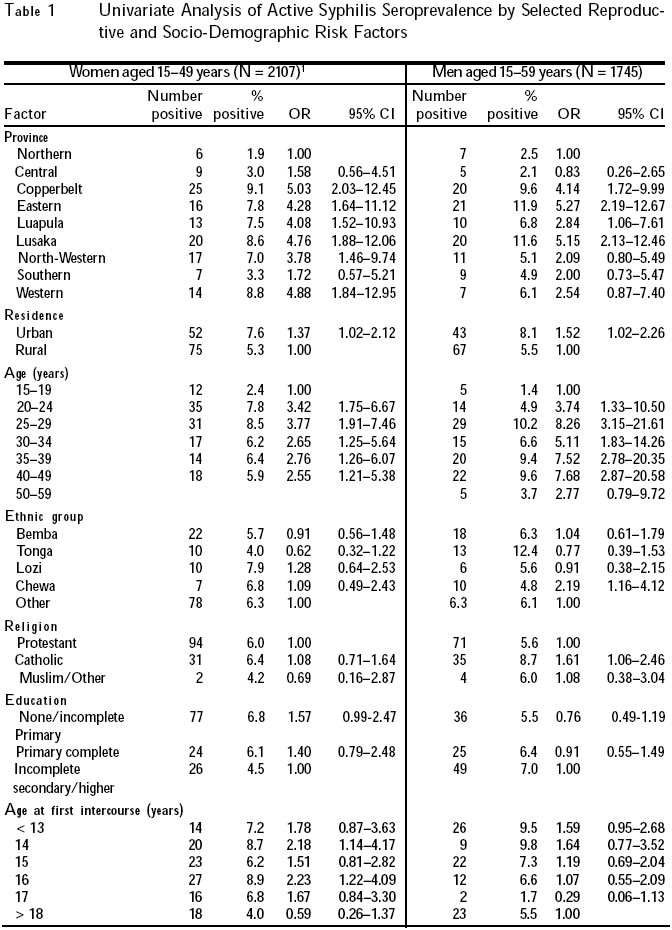
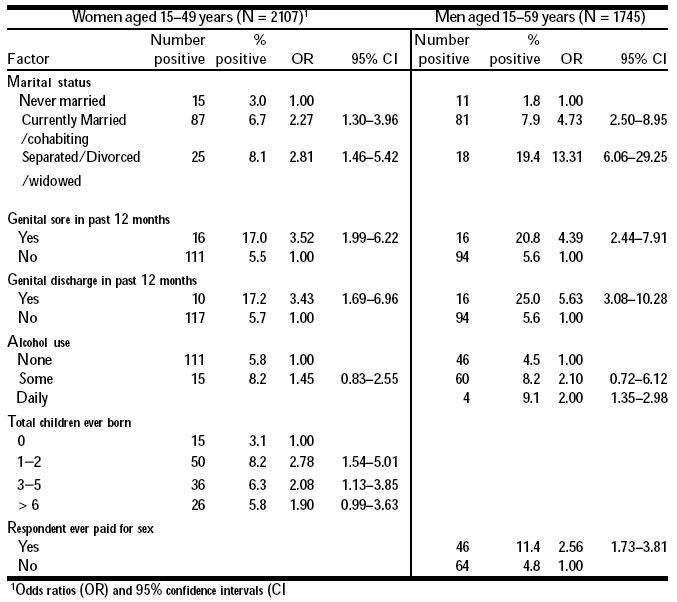
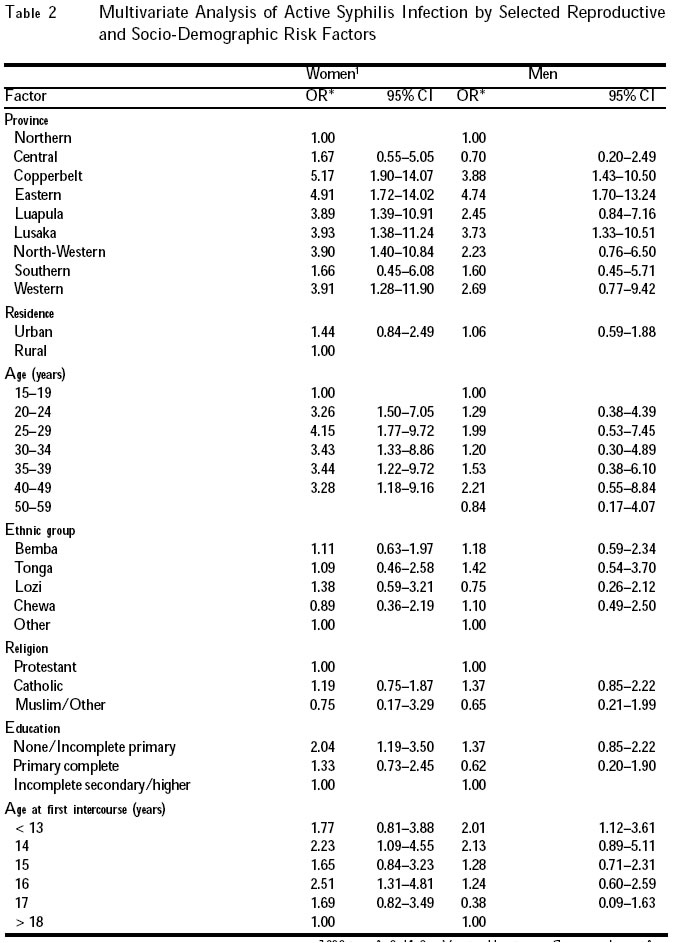
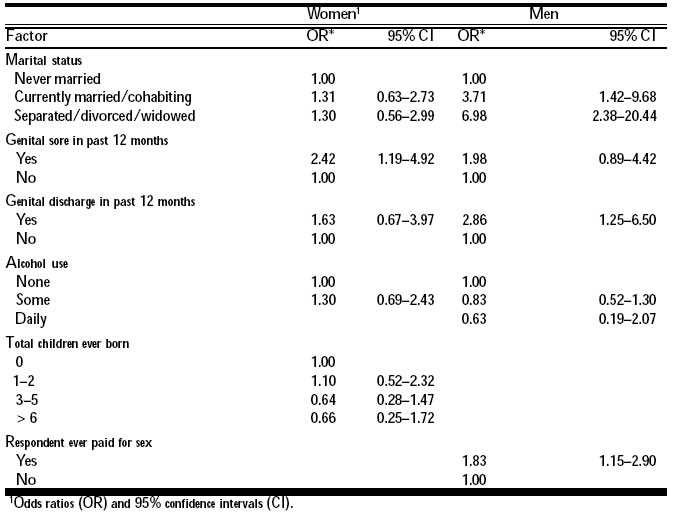
School of Public Health. Code Number: rh05030 Abstract This study examined the risk factors for active syphilis infection in a subset of nationally - representative population-based survey of Zambian men and women. Syphilis prevalence was 6.5% for women (N = 2107) and 7.4% for men (N = 1745). In the multivariate model, province was a strong risk factor for active syphilis infection, with Copperbelt, Eastern, Luapula, Lusaka, North-Western and Western Provinces presenting significantly higher risk for women, and Copperbelt, Eastern and Lusaka Provinces presenting significantly higher risk for men compared to the Northern Province. In addition to province, age, education, age at first intercourse, marital status, history of genital sore or discharge, and having ever paid for sex were independent predictors of syphilis infection. Given the ongoing HIV-1 epidemic in Zambia, more aggressive diagnosis and treatment of active syphilis infections, particularly in high-risk provinces, are important strategies to reduce reproductive morbidity and curb HIV-1 transmission. (Afr J Reprod Health 2005; 9[2]: 107-117) Résumé L'étude a examiné les facteurs de risque de l'infection de la syphilis active dans un sous-ensemble d'une enquête basée sur la population représentative du pays entier, auprès des hommes et des femmes zambiens. La fréquence de la syphilis était de 6,5% pour les femmes (N=2107) et de 7,4% pour les hommes (N=1745). D'après le modèle multifactoriel, la province constituait un facteur important pour l'infection de la syphilis active. Les provinces comme Copperbelt, Eastren, Luapula, Lusaka, Nort-Western et Western représentent les provinces à plus haut risque pour les femmes alors que les provinces de Copperbelt, Eastern et Lusaka constituent des provinces à plus haut risque pour les hommes comparées aux provinces du Nord. En plus de la province, l'âge, l'instruction, l'âge au moment du premier acte sexuel, l'état civil, les antécédents de la plaie génitale ou de l'écoulement génital et si l'on a jamais payé pour l'acte sexuel, étaient des indices indépendants de l'infection de la syphilis. Etant donné l'épidémie du VIH-1 en cours en Zambie, il faut des diagnostics et des traitements plus agressifs des infections de la syphilis active, surtout dans les provinces à haut risque qui serviront d'importantes stratégies pour réduire la morbidité de la reproduction et pour freiner la transmission du VIH-1. (Rev Afr Santé Reprod 2005; 9[2]: 107-117) Key Words: STI, HIV, risk, diagnosis, Africa Introduction Despite the ready availability of antibiotic medications in most parts of the world, syphilis remains a major preventable cause of reproductive morbidity and poor pregnancy outcomes worldwide.1 Syphilis, a bacterial infection caused by Treponema pallidum, is generally transmitted via sexual contact (including anal and oral intercourse) as well as vertically. Untreated syphilis has multiple stages including incubation, primary, secondary and tertiary infections.2 Patients in the primary or secondary stages of disease are considered to have active syphilis, defined as a reactive rapid plasma reagin (RPR) test, as well as a positive treponemal specific test, such as the Treponema pallidum hemagglutination assay (TPHA). For women of reproductive age, active syphilis infection carries increased risk of fetal loss and adverse pregnancy outcomes.3 Among women in the primary stage of syphilis infection, mother to child transmission during pregnancy is about 100%.4 Up to 40% of untreated maternal syphilis cases resulted in spontaneous abortion, stillbirth, or perinatal death.5 Surviving infants with congenital syphilis suffer multiple long-term morbidities.6,7 Active syphilis infection is associated with a three to five fold increased risk of HIV-1 acquisition.8 This increased risk is due to increased HIV-1 shedding, increased concentration of inflammatory cells in the genital tract and disruption of membrane integrity.10,11 Previous studies in sub-Saharan Africa have examined the risk factors associated with active syphilis infection.11-16 Among women and men, multiple sexual partners, concurrent infection with another sexually transmitted disease (STD), and being separated, divorced or widowed have been associated with increased risk of active syphilis infection. Risk factors unique to women include low education, early age at first sexual intercourse, engaging in transactional sex, high parity, a history of perinatal death, and an independent source of income. Risk factors unique to men include lack of circumcision and practicing a traditional religion. In addition to regional studies of syphilis infection, several Zambia-specific studies have been undertaken. Risk factor analyses in these studies found few variations according to marital status, educational level, economic state, or parity. Authors concluded that a widespread lack of awareness and generalised infection contributed to Zambia's continuing high rates of syphilis, as opposed to any particular sub-group or behaviour. 17,18 Data from the 1998 and 2002 antenatal clinic (ANC) sentinel surveillance of syphilis trends in Zambia show multiple risk factors for active syphilis infection according to RPR testing. The 1998 survey found urban residence; a history of marriage, separation, divorce or widowed status; a genital ulcer or discharge; and a sexually transmitted disease in the past 12 months to be significantly associated with active syphilis infection. Of these risk factors, a smaller subset remained significant in 2002, including separated, divorced, or widowed status; history of genital ulcer or discharge; or a sexually transmitted disease in the past 12 months. 19 This study focused on the risk factors for active syphilis infection among Zambian women aged 15-49 years and of Zambian men aged 15-59 years, with particular focus on province of residence. The recent release of the Zambia Demographic and Health Survey 2001-2002 presented a unique opportunity: for the first time nationally representative, population-based prevalence data became available for HIV-1 and syphilis. This survey found a high prevalence of syphilis and HIV-1: 6.5% of women and 7.4% of men had active syphilis infection, and 17.8% of women and 12.9% of men tested positive for HIV-1. 20 Given the generalised status of HIV-1 epidemic in Zambia, efforts to lower these high prevalence levels of syphilis and HIV-1 can be overwhelming and expensive. The aim of this study was to investigate the association of province of residence to active syphilis infection, enabling the development of more targeted campaigns to curb transmission among those populations at greatest risk. Methods Data Collection The Zambia Demographic and Health Survey 2001-2002 (ZDHS 2001/2) was the primary data source used for analysis.20 This survey was nationally representative, featuring population-based data and serologic testing of women and men for HIV-1 and active syphilis infection. Of the 7,658 women and 2,145 men in the general survey population, final serologic syphilis testing results were available for 2,107 women and 1,745 men. Refusal rates were not clearly specified. Initial screening tests were performed using RPR testing, thus detecting active syphilis infections.21 Those with reactive results underwent additional testing using treponemal-specific confirmation TPHA testing to decrease false positive results.21 Statistical Analysis SAS statistical software version 8.2 (SAS Institute Inc., Cary, North Carolina, USA) and STATA version 8 (Stata Corporatoin, College Station, Texas, USA) were used for analysis. A two-stage cluster sample design stratified by residence and province was used. Prevalence estimates took the sampling design into account. Associations between active syphilis infection and predictor variables were summarised with unadjusted odds ratios (OR) and 95% confidence intervals (CI), stratified by sex. Variables were entered into the multivariate model for men and women according to the level of significance in the univariate analysis (p = 0.1) for either sex. Multivariate analyses were performed using logistic regression. Covariates found to modify fully adjusted effect estimates by 20% or more were considered confounders and retained in the final model. Effect modification was considered with respect to alcohol and province of residence as well as domestic violence and province of residence; none of these interactions was significant. Missing data were analysed using the missing variable indicator.22 Ethical Approval The analysis was based on secondary data (Demographic and Health Survey data), thus no IRB approval was required. Results Any person with a missing syphilis diagnosis result was excluded from the analysis, leaving a total of 2,107 women and 1,745 men included in the multivariate analysis, among whom there were 127 and 110 confirmed cases respectively. National prevalence of active syphilis was 6.5% (95% CI 5.0-8.0) for women and 7.4% (95% CI 6.0-9.0) for men, with substantial variation across provinces (Figure 1). The active syphilis prevalence rate ranged from 9.1% in Copperbelt to 1.9% in Northern Province for women, and for men from 11.9% in Eastern to 2.1% in Central Province. There was evidence of some misreporting among survey respondents, including active syphilis cases among those respondents reporting never having had sexual intercourse. Given the difficulty in discerning the exact nature of the misreporting, women who reported never having had sexual intercourse were included in the analysis. There was little evidence of systematic difference among those testing for syphilis and those in the general survey sample who were not tested for syphilis. Women differed with respect to province, recent history of a genital sore, and whether they had experienced domestic violence. Men differed by urban versus rural residence, province, ethnic group, and whether they had ever been tested for HIV-1 (data not shown). In the univariate analysis for women, there were multiple significant predictors (p = 0.10) of active syphilis infection, including urban residence, residence in certain provinces, age, educational level, age at first intercourse, current marital status, genital sore, genital discharge, and parity (Table 1a, b). Number of sexual partners, condom use at last sex, age at first marriage, age at first birth, literacy, history of rape, having experienced domestic violence, media exposure (newspaper, radio or television), knowledge of safe sex methods, length of time at present residence, and an older male partner, were not found to be significantly associated with active syphilis infection (data not shown). Men were also found to have multiple factors associated with active syphilis infection in the univariate analysis (p = 0.10) including urban residence, residence in certain provinces, age, Chewa ethnic group affiliation, religion, current marital status, genital sore, genital discharge, daily alcohol consumption, and having paid for sex (Table 1). Number of sexual partners in the last 12 months, condom use at last sex, age at first marriage, literacy, media exposure (newspaper, radio or television), knowledge of safe sex methods, number of unions, and length of time at present residence were not found to be significantly associated with active syphilis infection (data not shown). In the multivariate logistic regression model, province of residence, age, educational level, age at first intercourse, and a history of genital sore in the past 12 months remained significant risk factors for active syphilis infection in women (Table 2a, b). Residence in Copperbelt, Eastern, Luapula, Lusaka, North-Western and Western Providences conferred significantly higher risk of active syphilis compared to Northern Province. Among age groups, each five-year age group over age 20 exhibited higher risk relative to the 15-19-year-old reference group. Women with no education or incomplete primary education had twice the risk of syphilis as compared to women with incomplete secondary education or higher education (OR 2.04, 95% CI 1.19-3.50). Women who reported having had a genital sore within the last 12 months had an increased risk of active syphilis infection (OR 2.42, 95% 1.19-4.92). For men, province of residence, age at first intercourse, current marital status, genital discharge, and having ever paid for sex remained significant risk factors for active syphilis infection in the multivariate logistic regression. Copperbelt, Eastern and Lusaka Provinces conferred significantly higher risk for syphilis infection among men, again compared to Northern Province. Those separated, divorced or widowed were at nearly seven times the risk of having active syphilis when compared to men who had never been married (OR 6.98, 95% CI 2.38-20.44), and currently married or cohabiting men had almost four times higher risk (OR 3.71, 95% CI 1.42-9.68) Whereas genital sore but not discharge was important for women, among men, genital discharge appeared to be more important, conferring a relative risk of almost three times that of men with no history of genital discharge in the past year (OR 2.86, 95% CI 1.25-6.50). Having paid for sex remained significant in the multivariate regression model for men (OR 1.83, 95% CI 1.15-2.90). Discussion As hypothesised, province of residence remained a very strong risk factor for active syphilis infection, even after adjustment for background characteristics and sexual risk behaviours. This finding has clear implications for public health programming particularly in Copperbelt, Eastern and Lusaka Provinces, where both men and women are at significantly elevated risk for active syphilis infection as compared to Northern Province. While Copperbelt and Lusaka Provinces have major urban cities (Ndola and Lusaka), urbanity did not prove to be a significant risk factor in the multivariate analysis and, thus, cannot solely explain the increased risk observed in these provinces. Transport routes alone also fail to explain these findings. Main trucking routes from Zimbabwe to Tanzania cross Southern, Central, Lusaka and Copperbelt Provinces, and one would expect to see increased risk throughout all of these provinces if migration were a main risk factor driving the association seen in provinces. Further analyses, possibly including qualitative work, are needed to enhance the understanding of provincial variations in the prevalence of active syphilis. For instance, health care services and treatment for syphilis might play an important role, but we do not have any information about these factors. Age was strongly associated with risk for syphilis infection in women but not in men. This finding persisted even after controlling for background characteristics and sexual behaviour risk factors. As soon as Zambian women reach age 20, their risk for infection increases almost three-fold and stays elevated throughout their reproductive years. It may be that age is acting as a proxy for some characteristics in women that is not well captured by the available data due to misreporting, such as lifetime number of sexual partners. However, this finding should be viewed with caution, as women who had not yet undergone sexual debut were included in the reference group due to widespread misreporting of exposure. This may cause an artificially low prevalence in the reference group, thus inflating the risk of older age groups by comparison. Education was an important risk factor for syphilis infection for women, but not for men. Women with fewer than five years of education had an increased risk for syphilis infection when compared to those women with complete secondary school or higher education. Literacy, however, was not found to be a predictor of syphilis infection (data not shown). It is not simply the inability to read, then, that predisposes women of no or low education to syphilis infection, but perhaps some other skills, attitudes, or experiences acquired in the process of formal education. It is possible that women with the lowest educational attainment were also the most disadvantaged, and these women may resort to multiple sexual relationships as a means of livelihood. Interestingly, for men, educational attainment was not a significant predictor of syphilis risk. This finding suggests that while improvements in general primary education may reduce women's risk of syphilis, it is unlikely to change men's risk. Early age at first intercourse, often cited as a risk factor, was important for men and women. Men beginning sexual relations at age 13 or earlier had twice the risk of active syphilis infection compared to those delaying sexual debut until age 18. This is to be expected, particularly as early age at first sexual intercourse may be an indication of lifetime number of sexual partners. Among women, however, there was no clear trend with respect to early sexual debut and risk of active syphilis infection. Initiating sexual intercourse at a very young age (14 years or younger), at age 15, or at age 17 was not associated with an increased risk of active syphilis infection when compared with those delaying sexual relations until age 18 or older. Those women who underwent sexual debut at age 14 were at a marginally significant increased risk for active syphilis infection, and women undergoing sexual debut at age 16 had more than twice the risk of syphilis infection than those waiting until age 18 or older. While research is needed to clarify why risk might be elevated for certain age groups and not others, it is clear that delaying sexual relations until age 18 is beneficial for both men and women in terms of mitigating risk for active syphilis infection. Men's current marital status was an important factor in risk of active syphilis infection. As expected, men separated, divorced or widowed at the time of survey were at a very high risk for syphilis when compared to never-married men. Interestingly enough, men who reported being married or cohabitating at the time of survey were also at an increased risk when compared to single men. This is somewhat counter-intuitive, as one would expect single men to have higher rates of partner exchange and thus be at higher risk for active syphilis infection. Given that condom use with a regular partner is quite low, this finding raises important concerns about whether men are monogamous when in union and the subsequent risk for their wives or partners. While several behavioural risk factors were significant for men, background characteristics were more predictive of risk of active syphilis infection in women. This raises important questions about the efficacy of behaviour change interventions to decrease women's risk of syphilis infection and the underlying factors causing their vulnerability. Until this is better understood, the best public health strategy may be more aggressive diagnosis and treatment of women based on background characteristics, while still focusing on behavioural risk factors in men. There are several important limitations to the analyses performed above. First, given the clear evidence of misreporting, men and women who reportedly never had intercourse were included in the analyses. This non-differential misclassi-fication may have caused a bias toward the null and, therefore, these findings may have been somewhat attenuated by the inclusion of women and men who have not yet had sexual intercourse. Second, some sub-categories had a relatively small sample size and were collapsed into broader categories to increase statistical power. In doing so, subtle gradations of risk may have been obscured. Finally, certain risk factors that may be important for active syphilis infection were not available for study in the Zambia Demographic and Health Survey data set. Perhaps chief among these was socio-economic status, which may have an important role in the transmission of infection, particularly as regards women's vulnerability and ability to negotiate condom use. With respect to generalisability, women and men tested for syphilis were generally comparable to those not tested for syphilis in the general survey population. The existing differences did not suggest that high risk individuals were consistently more or less likely to consent to and participate in testing. As such, the sample tested for syphilis was representative of the general survey sample. Given that this was a nationally representative, population-based survey, these results are, by extension, generalisable to Zambian men and women of reproductive age. Generalisability to other sub-Saharan African countries should be undertaken with caution. As past studies of syphilis risk factors in the region have shown, the factors influencing sexual behaviour are numerous and vary widely. In conclusion, the results of this analysis largely concur with many of the previous published findings. Unlike previous studies, however, these results underscore the importance of geographical variation in active syphilis infection. These findings suggest that in the case of Zambia, public health programming may benefit focusing less on certain risk behaviours and more on regions of highest risk including Copperbelt, Eastern and Lusaka Provinces for men and women, and additionally Luapula, North-Western and Western Provinces for women. Treating and preventing syphilis infection is essential to reduce reproductive morbidity and poor pregnancy outcomes; in the context of Zambia's continuing HIV-1 epidemic, this task is even more urgent. References
Copyright 2005 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh05030t1a.jpg] [rh05030t1b.jpg] [rh05030f1.jpg] [rh05030t2b.jpg] [rh05030t2a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}