 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 9, No. 3, December, 2005, pp. 27-40 Factors Contributing to Maternal Mortality in North-Central Nigeria: A Seventeen-year Review Facteurs qui contribuent à la mortalité maternelle au Nord-Central du Nigéria: Bilan couvrant dix-sept ans. Le rapport de la mortalite maternelle au Nigéria compte p;armi les plus hauts du monde. IAO Ujah1, OA Aisien2, JT Mutihir1, DJ Vanderjagt3, RH Glew3 and VE Uguru1 1Department of Obstetrics and Gynaecology, Faculty of Medical Sciences, University
of Jos, Jos, Nigeria. 2Department of
Obstetrics and Gynaecology, University of Benin, Benin City, Nigeria. 3Department
of Biochemistry and Molecular
Biology, University of New Mexico Medical School, Albuquerque, New Mexico,
USA. Code Number: rh05037 ABSTRACT Maternal mortality ratio in Nigeria is one of the highest in the world. This paper reports a facility based study in north-central Nigeria to determine the magnitude, trends, causes and characteristics of maternal deaths before and after the launch of the Safe Motherhood Initiative in Nigeria, with a view to suggesting strategic interventions to reduce these deaths. The records of all deliveries and case files of all women who died during pregnancy and childbirth between January 1, 1985 and December 31, 2001, in the maternity unit of Jos University Teaching Hospital, Jos, Nigeria, were reviewed. Data collected were analysed for socio-biological variables including age, booking status, educational level, parity, ethnic group, marital status, mode of delivery, duration of hospital stay before death occurred, cause (s) of maternal deaths. There were 38,768 deliveries and 267 maternal deaths during the period under review, giving a maternal mortality ratio (MMR) of 740/100,000 total deliveries. The trend fluctuated between 450 in 1990 and 1,010/100.000 deliveries in 1994. The mean age of maternal death was 26.4 (SD 8.1) years. The greatest risk of MMR was among young teenagers (>15 years) and older women (< 40 years). Parity-specific maternal mortality ratio was highest in the grand multiparous women. Unbooked as well as illiterate women were associated with very high maternal mortality ratio. The Hausa - Fulani ethnic group contributed the largest number (44%) by tribe to maternal mortality in our study. The major direct causes of deaths were haemorrhage (34.6%), sepsis (28.3%), eclampsia (23.6%) and unsafe abortion (9.6%). The most common indirect causes of death were hepatitis (18.6%), anaesthetic death (14.6%), anaemia in pregnancy (14.6%), meningitis (12.0%), HIV/AIDS (10.6%) and acute renal failure (8.0%). Seventy- nine percent of the maternal deaths occurred within 24 hours of admission. Most of the deaths were preventable. A regional-specific programme should be planned to reduce the deplorably high maternal mortality in north-central Nigeria. (Afr J Reprod Health 2005; 9[3]:27-40) RÉSUMÉ Cet article fait un rapport d’une étude basée sur des é tablissements au nord-central du Nigéria afin de déterminer l’ampleur, les tendances, les causes et les caractéristiques des décès maternels avant et après le lancement de "Safe Motherhood Initiative" au Nigéria, en vue de proposer des interventions stratégiques pour réduire ces décès. Nous avons étudié les dossiers de toutes les femmes qui sont mortes pendant la grossesse et l’accouchement entre le 1er janvier 1985 et le 31 décembre 2001 auprès du service de maternité du Centre Hospitalier Universitaire de Jos, Nigéria. Les données recueillies ont été analysées pour déterminer les variables socio-biologiques y compris l’âge, l’état de réservation, le niveau dinstruction, la parité, le groupe ethnique, l’état civil, la manière d’accouchement, la durée du séjour à l’hôptial avant le décès, la cause ou les causes des décès materrnels. Il y avait 38,768 accouchements et 267 décès maternels pendant la periode en cours de révision, ce qui donne un rapport de mortalité maternelle (RMM) de 740/100,000 de tous les accouchements. Cette tendance variait entre 450 en 1990 et 1,010/100 accouchements en 1994. L’âge moyen du décès maternel était 26, 4 (SD 8,1) ans. Le plus grand risque du RMM se trouvait chez les plus jeunes adolescentes (> 15ans) et les femmes les plus âgées (< 40ans). Le rapport de mortalité maternelle particulier à la parité était le plus élevé chez les grandes femmes multipares. Le rapport de mortalité maternelle très élevée a été associée aux femmes illetrées. Le groupe ethnique Hausa/Fulani a contribué le plus (44%) par rapport aux autres groupes, à la mortalité maternelle dans notre étude. Les causes directes principales du décès étaient l’hémorragie (34,6%), la septicité (28,3%) l’éclampsie (23,6%) et l’avortement dangereux (9,6%). Les causes les plus indirectes de la mortalité étaient l’hépatite (18,6%), la mort anesthétique (14,6%), l’anémie dans la grossesse (14,6%), la méningite (12,0%), le VIH/SIDA (10,6%), et l’insuffisance rénale aiguë (8,0%). Soixante-dix-neuf pour cent des décès maternels se sont produits au cours de 24 heures après l’admission. La plupart des décès étaient évitables. Il faut prévoir un programme à caractère particulier à la région pour réduire la mortalité maternelle qui est déplorablement élevée au nord-central-central du Nigéria. (Rev Afr Santé Reprod 2005; 9[3]:27-40) KEY WORDS: MMR, age, parity, illiteracy, haemorrhage, eclampsia, abortion, Nigeria Introduction The estimated number of maternal deaths worldwide in 2000 was 529,000. These deaths were almost equally divided between Africa (251,000) and Asia (253,000), with about 4 % (22,000) occurring in Latin America and the Caribbean, and less than 1% (2500) in the more developed countries. 1 For every pregnant woman who dies, at least another 30 suffer serious injuries and often permanent disability.2 Maternal mortality ratio (deaths/100,000 live births) by region was highest in Africa (830), followed by Asia (330), Oceania (240), Latin America and the Caribbean (190), and the developed countries (20). India had the highest number of maternal deaths (136,000), followed by Nigeria (37,000). With the exception of Afghanistan, the countries with highest maternal mortality ratios (MMRs) were all in Africa.1 The average risk of dying from pregnancy-related causes in Africa is about one in 20, compared to one in 2000 in the more developed countries.3 During the past half century there was a marked reduction in maternal mortality rate, especially in developed countries, to such a level that the standards of obstetric care could no longer be assessed in terms of mortality rates alone. However, the picture is different in the developing world, and the disparity in deaths between developed and developing countries is greater for maternal mortality than for any other global health problem. Of all the health statistics compiled by the World Health Organization (WHO), the largest discrepancy between developed and developing countries occurred in maternal mortality.5 While 25% of females of reproductive age lived in developed countries, they contributed only 1% to maternal deaths. Females of reproductive age in developing countries account for 75% of all females of reproductive age worldwide and they account for 99% of all maternal deaths.4 Studies from various countries of sub-Saharan Africa indicate that maternal mortality is not only deplorably high but is indeed increasing even after the launch of the Safe Motherhood Initiative (SMI) in Kenya in 1987.6-15 Many believe that the most important common denominator that is central to the increasing maternal deaths in Africa is poverty. Nigeria, the most populous country in Africa, has one of the highest maternal mortality rates in the world.16 Like in most countries in the developing world, maternal mortality rate in Nigeria is on the increase.16 In most areas of sub- Saharan Africa restructuring has promoted dangerous inequality, social upset and disintegration of all forms of infrastructure that were built in the 60's and 70's. Attempt at debt recovery has collapsed: currently sub-Saharan Africa's total debt as a percentage of their GNP exceeds 110%, compared to around 30% in 1980. The result is misery all round with the most telling effects on education and maternal and child health.16 The maternal mortality ratio of any nation reflects not only the adequacy of obstetric care but also the general level of social and economic development. Although a large number of publications have been made on maternal mortality in Nigeria, there are only few of these that report on the situation in north-central region of the country. The region is peculiar because it is inhabited largely by the ethnic minorities of the Middle Belt of Nigeria with their distinct culture and custom. The authors were therefore motivated to conduct a comprehensive study of maternal mortality in the tertiary health institution in the region. The objectives of the study were:
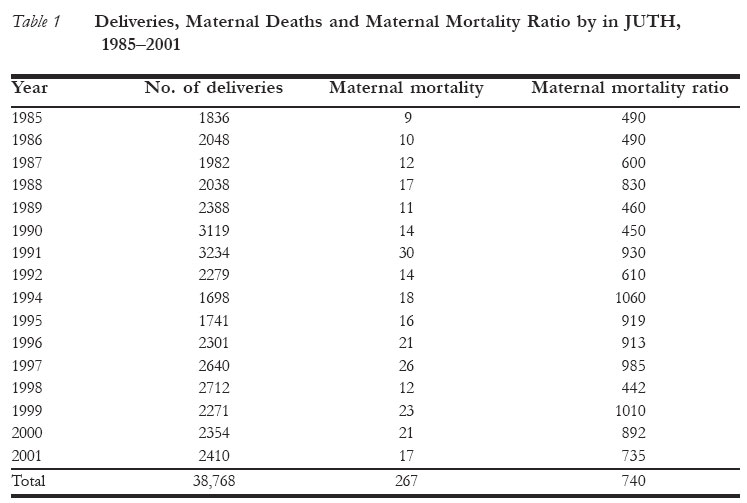
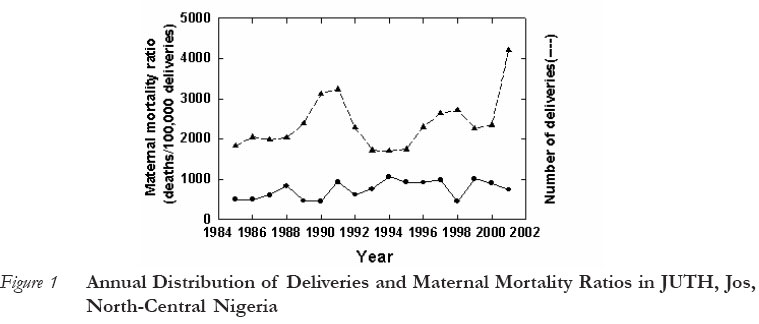
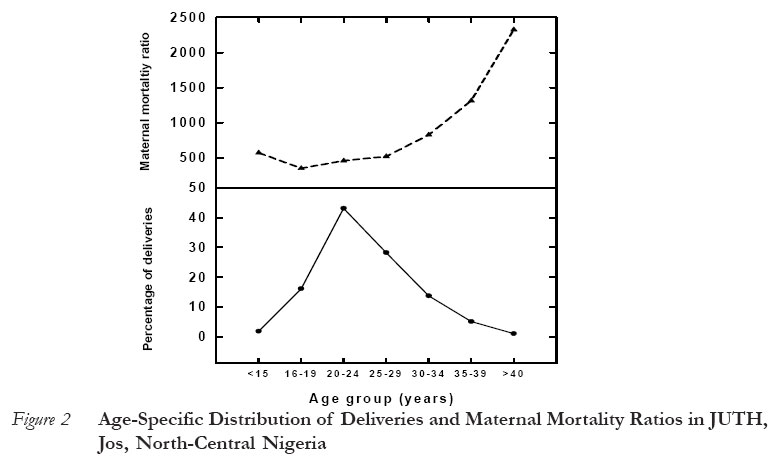
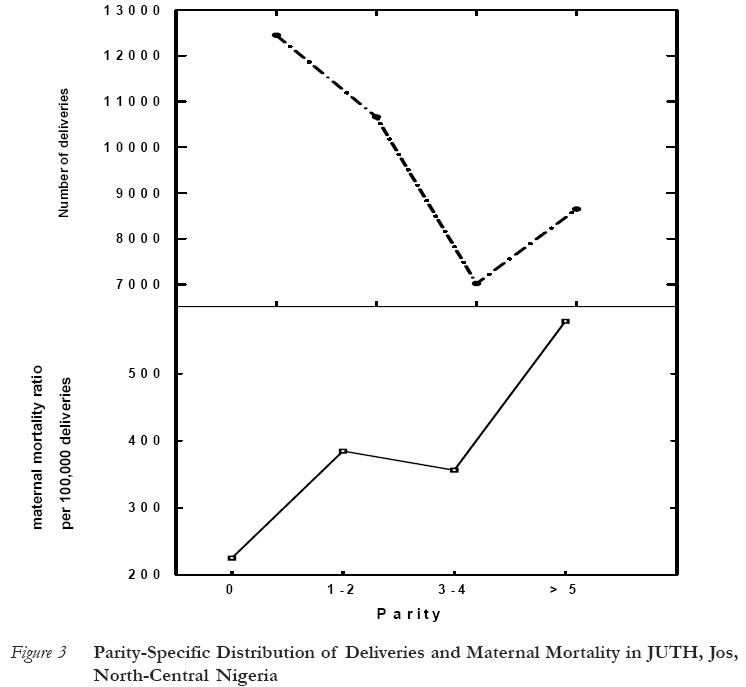
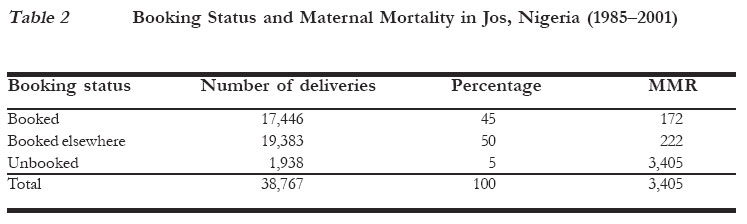
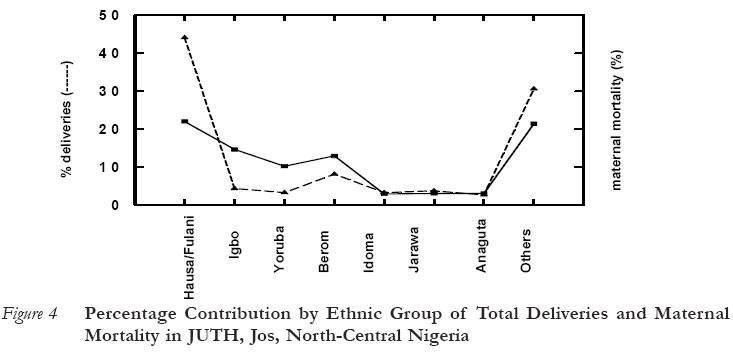
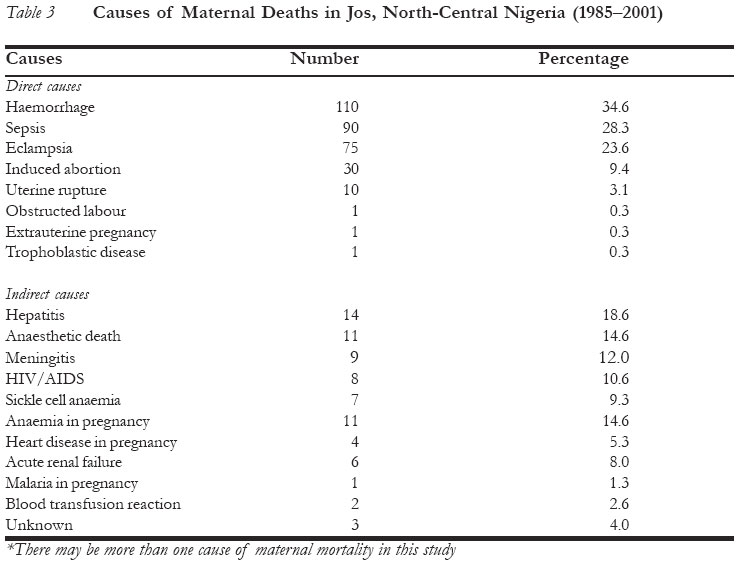
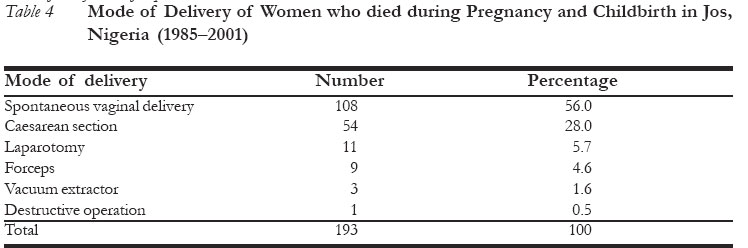
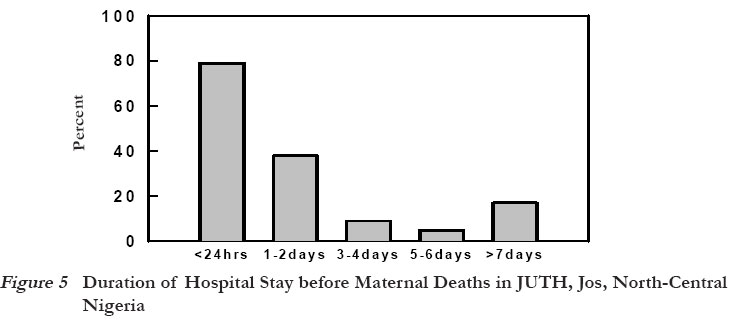
Patients and Methods Plateau State, situated in north-central region of Nigeria, is one of the 36 states of Nigeria. It has 3.3 million heterogeneous inhabitants with over 40 ethno-linguistic groups. None of the ethnic groups claims numerical dominance. The climatic conditions of Plateau State are greatly influenced by its high altitude, with the months of November through February recording as low as 1°EC. The Jos University Teaching Hospital (JUTH) is located in Jos, the state capital, and is the foremost tertiary health institution in north-central Nigeria. With a total of 520 beds, 70 of which are obstetric beds, the hospital provides primary and secondary health services in addition to its statutory tertiary functions. The hospital also provides specialised health services to the contiguous states of Bauchi, Benue, Kaduna, Nasarawa and the Federal Capital Territory, Abuja. The maternity unit of the hospital takes about 3000 deliveries per annum. A study conducted between 1978 and 1980 in the Obstetrics and Gynaecology Department of JUTH revealed that the maternal mortality ratio was 410/100,000 total births.17 Between January 1985 and December 2001 (17 years), the case files of all women dying in pregnancy and childbirth in the maternity unit of the hospital were promptly retrieved as soon as a death occurred. The study ensured that a detailed and comprehensive record-keeping of all deliveries, including complications and maternal deaths, was kept in the labour, antenatal, postnatal and caesarean section wards. To ensure compliance, two of the authors supervised record- keeping in the unit while another did the same in the delivery ward. The case file of every maternal death that occurred during the period under review was promptly sent to one of the authors. The files were then reviewed and any doubtful or incomplete information provided in the file was cross-checked with close relatives of the deceased. All relevant information was transferred into the proforma designed for the study. By so doing, the chances of losing the case file altogether due to poor record-keeping in our health facilities was apparently reduced. The following socio-biological variables were analysed: age, booking status as previously categorised,6 educational level, parity, ethnic group, marital status, mode of delivery, date and time of admission, and the cause(s) and contributing factors to maternal deaths. The date and time of death were recorded in order to determine the duration of hospital stay before death occurred. For religious and cultural reasons, post-mortem examinations are rarely permitted in this part of the country; therefore, the cause(s) of maternal death were based only on clinical assessment and diagnosis. Data analysis was done using NCSS 2001 and PASS 2002 software. Results Yearly Variation of MMR A total of 267 maternal deaths occurred among 38,768 deliveries over the 17-year period, making the maternal mortality ratio (MMR) 740/100,000 total deliveries. However, the maternal mortality ratio varied greatly from 490/100,000 deliveries in 1985 to 1010/100,000 deliveries in 1999 (Table 1). There was no consistent trend in MMR over the study period. It rather showed annual fluctuations in MMR. The MMR peaked in 1991, 1994, 1997 and 1999 with the highest ratios of 1060 and 1010 being recorded in 1994 and 1999 respectively. The lowest MMR of 442/100,000 deliveries was recorded in 1998. Annual deliveries at JUTH also fluctuated remarkably during the study period, with the lowest number of deliveries being recorded in between 1993 and 1995 (Figure 1). Characteristics of Women who Died during Childbirth The mean age of women who died during pregnancy and childbirth was 26.4 (SD 8.1, range 15-47) years. Figure 2 shows the bimodal pattern of maternal deaths that occurred in both extremes of the age range. The greatest risk of maternal death was among early teenagers and older women. For instance, while only 1.8% and 1.0% of all deliveries occurred among women aged ≤15 and ≥ 40 years respectively, these age groups had maternal mortality ratios of 573 and 2325/ 100,000 deliveries respectively. On the other hand, women aged 16-29 years, who accounted for 78.4% of all deliveries in Jos, appeared relatively protected from dying in pregnancy and/or childbirth. Parity distribution (Figure 3) (range 0-12) showed that maternal mortality increased with parity, and the highest maternal death was recorded in the grand multiparae (>5). The study also showed that a large number of deliveries occurred in primigravidae (32.1%) and grand multiparous women (22.3%), the parities that were associated with high risk of maternal deaths. Forty percent of all women who were delivered in JUTH received antenatal care (booked) and the maternal mortality ratio for this group of women was very low (172/100,000 deliveries) compared to the 5% of women who did not receive antenatal care (unbooked) and had maternal mortality ratio of 3405/100,000 deliveries (Table 2). Thus, the MMR among unbooked women was about 20 times greater than among women who had antenatal care (B) and 15 times worse than in women who booked for antenatal care elsewhere (BE) but were delivered at JUTH. The data show that women who had antenatal care and had their deliveries conducted in JUTH were relatively protected from death at pregnancy and childbirth. Another correlate of maternal death was the educational level of the women. About 70% of all maternal deaths occurred in women who were illiterate. Furthermore, the higher a woman's educational level, the less likely that she would die during childbirth. The ethnic group of the women was also an important risk factor for maternal mortality (Figure 4). The women who died during pregnancy and childbirth in JUTH during the period were from 38 ethnic groups. Although the Hausa - Fulani ethnic group accounted for 22% of all deliveries, they contributed a disproportionate 44% to maternal deaths. Other ethnic groups included Igbo (14.6%), Yoruba (10.2%), and Berom 12.9%, while their contributions to maternal deaths were 4.3%, 3.2% and 8.1% respectively. Berom is one of the major indigenous ethnic groups in Jos. The remaining 31 ethnic groups which contributed 30.6% to maternal deaths, accounted for 21.4% of all deliveries during the study period. These data show that the Hausa - Fulani ethnic group was at a higher risk of dying during pregnancy and childbirth in north-central Nigeria. Major Causes of Maternal Deaths The four most common direct causes of maternal deaths were haemorrhage 110 (34.6%), sepsis 90 (28.3%), eclampsia 75 (23.6%) and unsafe abortion 30 (9.4%). More than one factor may have contributed to maternal death in some cases (Table 3). Surprisingly, obstructed labour, a common cause of maternal death in many developing countries, was rare in this study. Ectopic pregnancy as a cause of maternal mortality was also uncommon. The leading indirect cause of maternal mortality (Table 3) was hepatitis, accounting for 18.6% of maternal deaths, followed by anaesthetic death (14.6%), meningitis (12%), HIV/AIDS (10.6%), sickle cell anaemia (19.3%), anaemia (14.6%) and acute renal failure (8.0%), which was a complication of eclampsia. It is noteworthy that hepatitis was the leading indirect cause of maternal deaths in north-central Nigeria. Of the 193 women who were delivered, majority (56%) had spontaneous vaginal delivery (SVD), followed by caesarean section (28%). Seven (3.7%) women had vaginal breach delivery, while 12 (6.2%) had assisted operative vaginal deliveries (vacuum and forceps) (Table 4). Eleven (5.7%) cases had laparotomy for ruptured uterus and extrauterine pregnancy. Destructive operation was not common, as only one case was reported in the study population. A large number of women 61 (21.3%) who died of maternal death were undelivered. Seventy-nine percent of all maternal deaths occurred within 24 hours of admission (Figure 5). The implication of this is that many of the women came to seek care when their condition had already become grave. Discussion This study revealed high maternal mortality ratio (MMR) of 740/100,000 deliveries in north-central Nigeria, similar to findings from previous studies in other parts of Nigeria.7-11 However, this ratio is much less than 2420/100,000 deliveries reported in Kano State,8 a predominantly Hausa- Fulani community in northern Nigeria. There was no consistent pattern or trend in MMR during the 17-year period. However, marked annual fluctuations of maternal mortality ratios were recorded (Figure 1). The "crescendo-descendo" pattern of maternal mortality ratios recorded in this study indicate that maternal mortality in Nigeria could exhibit "episodic outbreaks" and could be a "dynamic process" probably associated with certain trigger factors.8 Inconsistent and everchanging health policies, cost recovery and userfee policy introduced into the health system, coupled with unstable socio-political climate in Nigeria may have contributed significantly to the fluctuating maternal mortality ratios found in this study. Similar findings have been recorded in Kaduna13 and Kano States.8 The leading direct causes of maternal mortality we found in this study included haemorrhage, eclampsia, sepsis and unsafe abortion. This is similar to what has been reported from other parts of sub-Saharan Africa,7,8,12,14 although the order of frequency may vary. Obstructed labour, which was rare in this study, was found to be common (4.0%) with a maternal mortality ratio of 605/100,000 live births in a study in Gombe State.18 Another study among the Hausa-Fulani ethnic group of northern Nigeria estimated the prevalence of obstructed labour to be 1238/100,000 births.19 The study found that only 1.8% of all deliveries were among adolescent girls aged 10-15 years. This is in sharp contrast to the 6.7% recorded among early teenagers aged 15 years and below in Zaria where high incidence of early marriage and obstructed labour were also reported.20 Surprisingly, malaria as a cause of maternal mortality was not common in the present study. However, maternal deaths due to anaemia in pregnancy (14.6%) may have been associated with malaria. The strong association between hepatitis and maternal mortality that we noted in this study has been documented in previous studies from this hospital.6,17 It could be attributed to the high rate of consumption of locally brewed alcohol by women as well as men in this part of Nigeria. The alcohol is believed to contain impurities that are toxic to the liver. Anaesthetic death was responsible for as high as 14.6% of indirect causes of maternal deaths in the hospital. Specialist doctor anaesthetists are not widely available at JUTH or other hospitals in northern Nigeria. Therefore, nurse anaesthetists were trained to complement the anaesthetic services provided by the few doctors available. The recent recruitment of some inexperienced nurse anaesthetists may have been responsible for the high rate of maternal deaths due to improper administration of anaesthesia. Update courses should be provided to build the capacity of these nurses to reduce the incidence of avoidable deaths. HIV/AIDS may influence maternal mortality in several ways. Women living with HIV/AIDS may be more susceptible to direct or obstetric causes of maternal mortality such as postpartum haemorrhage, puerperal sepsis and complications of caesarean section. AIDS-related deaths may be incidental to pregnancy (fortuitous) or may be true indirect causes of maternal mortality where the infection itself or opportunistic infections such as tuberculosis progress faster in pregnancy.21 The extent of the contribution of HIV/AIDS to maternal mortality is difficult to quantify, specifically since the HIV status of pregnant women is not always known.21 National confidential enquiries in South Africa revealed that AIDS-related maternal mortality increased from 13% in 1998 to 17% in 2001.22,23 The contribution of HIV/AIDS to indirect causes of maternal mortality in this study was 12.1%. As the HIV/ AIDS epidemic spreads in Nigeria, the contribution of the infection to maternal mortality will certainly increase. Therefore, programmes to prevent mother to child transmission (PMTCT) of HIV should be greatly expanded so as to allow women easy access to counselling, testing and treatment. The high maternal mortality ratios recorded in 1994 and 1995 could be attributed to the social and political crises that accompanied the annulment of the June 12, 1993 presidential election and the overthrow of the Interim National Government (ING) by a military coup. The number of deliveries was the lowest recorded during the same period, because hospital staff as well as patients and pregnant women stayed away from public health institutions as a result of the lingering crises. The apparent reduction in the incidence of maternal mortality ratio between 1995 and 1998 found in the Kano study8 could be attributed to the positive impact of the Petroleum Trust Fund (PTF) programme, which was credited for reducing service fees as well as making drugs available in public health institutions in Nigeria. The maternal mortality ratio of 442/ 100,000 deliveries in 1998 was remarkably low and could be attributed to the positive impact of the PTF programme. However, it is doubtful if such isolated reduction in MMR could be due to the PTF programme of the then military government. Therefore, the low MMR recorded in 1998 remains inexplicable to us. The continuing increase of MMR in Nigeria and other parts of sub-Saharan Africa indicates that the intervention strategy for reducing maternal mortality through the Safe Motherhood Initiative (SMI) has been so far unsuccessful in Jos, northcentral Nigeria. We suggest that a regional-specific intervention policy be formulated to reduce the high MMR due to such main causes as haemorrhage, eclampsia, sepsis and unsafe abortion, as no worldwide policy could be applicable to every country.24 The maternal mortality reduction strategies should include building the capacity of skilled attendants (doctors and midwives) at childbirth to provide quality care to pregnant women and women in labour. It shoud also include retraining of traditional birth attendants (TBAs) and community health extension workers (CHEWs) to recognise early signs of complications. This is to encourage early and appropriate referrals to health facilities. Health facilities should be stocked with sufficient equipment and supplies to receive and manage obstetric emergencies promptly. The high incidence of maternal mortality due to unsafe abortion reported in this study provides ominous and warning signals to the magnitude of reproductive morbidity and mortality of Nigerian women, particularly among adolescents in northern Nigeria. Family planning is known to reduce maternal mortality by preventing illegal abortion and reducing the number of unwanted pregnancies.24,25 Policymakers and health-care providers should take this information very seriously because abortion laws remain restrictive in Nigeria and the prevalence and use of family planning services remains disappointingly low (< 10%).26 Contraceptive prevalence is even less than 10% in north-central Nigeria and most of the other regions of northern Nigeria, where conservative culture, custom and religious doctrine are serious barriers to modern family planning. Because of the overwhelming resistance to family planning by religious leaders and traditional rulers in Nigeria, particularly in the north, we suggest that well-directed and focused advocacy and sensitisation programmes targeted at policymakers, traditional rulers and religious leaders with appropriate and effective communication messages should be developed to improve family planning use. The overall goal of this is to reduce maternal mortality from unwanted and unplanned pregnancy. It is worrisome to know that as many as 21.3% of all maternal deaths in this study occurred among undelivered women and where 79% of all maternal deaths happened within 24 hours of admission. A similar figure of 28.3% had been reported from Ahmadu Bello University Teaching Hospital (ABUTH), Kaduna (northern Nigeria), where none of the women had received antenatal care.27 By far, a higher figure was reported in Ghana.27 The death of women who were undelivered was described as a double tragedy because the unborn babies died prematurely.27 Early recourse to post-mortem caesarean section will spare such babies. The issue of pregnant women dying undelivered is an indictment on the health system in Jos, because it is either that the quality of care is far below standard or that infrastructure is not in place to improve access to health-care by pregnant women. A report from south-west Nigeria documented some reasons for the "brought in dead" in Obafemi Awolowo University Teaching Hospital (OAUTH), Ile-Ife.28 The reasons included inability to obtain transportation in time, inability of the health-care staff to detect an obstetric emergency early enough, inability of the referring hospital to perform caesarean section and inability to pay for hospital costs,28 among others. We suggest that this group of women should be extensively studied in order to determine the risk factors for dying undelivered, to reduce the high incidence among women. Illiteracy was found to be closely associated with maternal mortality ratio, as 70% of all maternal deaths in this study occurred in women who had no formal education. This finding is in agreement with previous studies in Nigeria.7,8,13,20 Illiteracy is therefore an important risk factor for maternal mortality. This problem is further compounded by the fact that majority of these women were also not booked for antenatal care. Girl-child education, as stated in the Millennium Development Goal 2 (MDG 2), is an appropriate response to the high level of illiteracy in northern Nigeria. The Universal Basic Education (UBE) programme of the Federal Government of Nigeria is a long-term strategy for reducing maternal mortality. A particularly striking finding in this study was the high risk of the Hausa - Fulani ethnic group for maternal mortality. Of the 38 ethnic groups, the Hausa - Fulani ethnic group alone was responsible for 44% of deaths. The women in this ethnic group were mostly illiterate and unbooked for antenatal care. This is probably a reflection of the high prevalence of illiteracy among the women and low status accorded to women, including the practice of seclusion (purdah). A more detailed study should be conducted to determine if other factors also act as barriers to the utilisation of maternity service among women of this ethnic group, so that specific strategic programmes will be developed to reduce the unacceptably high incidence of maternal deaths. Maternal mortality is a symptom of poverty and the low status accorded to women. Women themselves contribute to their deaths through repeated pregnancies and causing significant socio-economic loss to society.24 Nigeria adopted the Structural Adjustment Programme (SAP) in 1986 as its economic policy. SAP was introduced to restore fiscal discipline but its doctrines were workers' retrenchment, removal of subsidies, currency devaluation, trade liberalisation and privatisation of public utilities.16 In most parts of sub-Saharan Africa, the restructuring promoted dangerous inequality, social upset and disintegration of all forms of infrastructure. In addition, the attempt at debt recovery collapsed and sub-Saharan Africa's total debt as a percentage of GNP exceeded 110% in 2003, compared to 30% in 1980.16 These policies have had negative impact on education, particularly of women, and on maternal and child health.16 The maternal mortality ratio of any nation reflects not only the adequacies of obstetric care but also the general level of social and economic development. This could also be related to the deteriorating living conditions and poverty that is prevalent in Nigeria. Following the introduction of SAP, maternal mortality ratios have continued to rise, as reported by Ekempu in Zaria, northern Nigeria.29 Although living conditions have seriously deteriorated in Nigeria, the situation may worsen as more Nigerians (70%) live below poverty line. The Federal Ministry of Health had set Year 2006 as the target year that maternal mortality and morbidity would have been reduced by 50%, neonatal morbidity by 30%, unwanted pregnancies by 50%, and sexually transmitted infections by 50%.26 We hope that these targets would be met in the face of the deteriorating health system. Nigeria had in the 1981-85 National Development Plan targeted particular health issues for special focus. These include the consideration for liberalisation of abortion laws; improvement in health-care delivery system to strengthen the downward trend in child, infant and maternal mortality and morbidity rates.30 Sadly, it is not only that these targets were not achieved but also that the health situation in Nigeria is much worse now than previously. Conclusion Maternal mortality ratio in north-central Nigeria has remained high and the trend is rising. The main direct causes of maternal mortality are haemorrhage, eclampsia, sepsis and unsafe abortion, while the indirect causes include hepatitis, anaesthetic complications, HIV/AIDS-related deaths and acute renal failure. Among the numerous ethnic groups in Nigeria, the Hausa - Fulani had the highest risk of dying during pregnancy and childbirth. Maternal age, illiteracy, grand multiparity and non-utilisation of antenatal services were risk factors for maternal mortality in this study. Seventy percent of the maternal deaths occurred within 24 hours of admission. The safe motherhood programme has so far been unsuccessful in Jos, north-central Nigeria. Recommendations A region-specific programme should be developed if the rising trend of maternal mortality is to be halted. These programmes should take into consideration the social, cultural and religious peculiarities of northern Nigeria. Intensive high level advocacy and sensitisation campaign programme targeted at policymakers, religious leaders and traditional rulers, with appropriate communication messages, should be developed to improve family planning services and use. In addition, abortion laws should be made less restrictive in Nigeria to reduce the high rate of maternal mortality resulting from unsafe abortion. A monitoring process using appropriate indicators should be developed to measure progress on maternal mortality reduction programmes. Finally, the economy must be improved to raise the living standards of Nigerians through the poverty alleviation programme of the Federal Government of Nigeria, which should ultimately contribute to the reduction of the deplorably high maternal mortality. Acknowledgements Our appreciation goes to the consultants of the department whose patients were included in the study. The Minority International Research Training (MIRT) programme of the University of New Mexico, Albuquerque, USA, awarded a four-week research fellowship to the first author. The visit facilitated the production of this research paper. REFERENCES
© Copyright 2005 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh05037f4.jpg] [rh05037t2.jpg] [rh05037f2.jpg] [rh05037t1.jpg] [rh05037f1.jpg] [rh05037f3.jpg] [rh05037t4.jpg] [rh05037t3.jpg] [rh05037f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}