 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 9, No. 3, December, 2005, pp. 51-58 What is Youth-Friendly? Adolescents' Preferences for Reproductive Health Services in Kenya and Zimbabwe Que signifie ’favorable à la jeunesse?’ Préférence des adolescents pour les services de santé de reproduction au Kenya et au Zimbabwe Annabel S Erulkar1, Charles J Onoka2 and Alford Phiri3 1Program Associate, Population Council, Accra, Ghana. 2Programme Officer for Research and Evaluation, Family Planning Association of Kenya, Nairobi, Kenya. 3Assistant Director, Evaluation and Research Unit, Zimbabwe National Family Planning Council, Harare, Zimbabwe. Correspondence: Dr Annabel Erulkar, Email: aerulkar@pcaccra.org Code Number: rh05039 ABSTRACT While there has been increased attention to youth-friendly reproductive health services, little research has been conducted among adolescents in developing countries to assess what characteristics of reproductive health services are most important to them. Large scale population-based surveys were carried out among youth in Kenya and Zimbabwe. A list of characteristics that programmers often think of as youth-friendly was read to respondents, after which they were asked to assess the importance of those characteristics in choosing their reproductive health services. Adolescents rated confidentiality, short waiting time, low cost and friendly staff as the most important characteristics. The least important characteristics included youth-only service, youth involvement and young staff, suggesting that adolescents do not prioritise stand-alone youth services such as youth centres, or necessarily need arrangements particular to youth such as youth involvement. The findings imply that most existing clinical services, even in the most resource-poor settings, are in a position to improve their level of youth friendliness. (Afr J Reprod Health 2005; 9[3]:51-58) RÉSUMÉ Alors qu’il y a eu une augmentation par rapport à l’attention faite aux services de santé de reproduction favorables à la jeunesse, peu de recherche a été menée au sein des adolescents dans les pays en développement pour évaluer les caractéristiques de santé de reproduction qui leur soient les plus importantes. Nous avons mené des enquêtes à grande échelle basée sur la population au sein des jeunes gens au Kenya et au Zimbabwe. Une liste des caractéristiques que les programmeurs considèrent souvent comme étant favorables aux jeunes a été lu aux interrogés. Ensuite, ils ont été demandés d’evaluer l’importance de ces caractéristiques-là dans le choix de leurs services de santé de reproduction. Les adolescents ont signalé que la confidentialité, une attente de courte durée, le coût bas et le personnel accueillant, étaient les caractéristiques les plus importantes. Les caractéristiques les moins importantes comprenaient le service reservé à seuls les jeunes, la participation des jeunes et le personnel jeune. Ce qui montre que les jeunes ne prioritisent pas les services de jeunes isolés tels les centres de jeunes, ou bien qu’ils n’ont pas forcément besoin d’arrangements qui concernent en particulier les jeunes comme la participation de jeunes. L’étude laisse entendre que la plupart des services cliniques, même dans les milieux de maigre ressource, sont en mesure d’améliorer leur niveau de gentillesse envers les jeunes. (Rev Afr Santé Reprod 2005; 9[3]:51-58) KEY WORDS: Adolescence, Youth friendliness, Kenya, Zimbabwe Introduction Reproductive health (RH) programmes targeted at adolescents are a relatively new phenomenon in sub-Saharan Africa, with the first programmes having been established in the late 1970s. In response to the understanding that many young people are ill-informed on matters concerning sexuality and RH, most of the early programmes focused on giving RH information to young people or on increasing parents' and teachers' capacities to convey such information. Programmes focusing on improving adolescents' access to reproductive health services, however, are comparatively less developed on the continent.1 This is possibly because of the political sensitivity and socio-cultural biases surrounding provision of family planning methods to unmarried young people.2,3 Numerous studies have revealed that adolescents are neither well-received nor comfortable in mainstream family planning clinics, which are mostly government-owned maternal and child health/ family planning (MCH/FP) facilities. Many of the existing studies regarding young people's reception at clinics have focused on providers' reactions to them. Young people often feel that they are unwelcome in such facilities, encountering providers who are judgmental, who treat them rudely, or who deny them services.4-7 Studies in several African countries revealed that providers impose age restrictions on providing family planning methods, including condoms, even when such restrictions are neither medically justifiable nor officially sanctioned.8,9In a study in Tanzania, more than one-third of providers placed restrictions on condom provision based on age. This is surprising, given that condoms are very suitable to the sporadic nature of adolescent sexual behaviour as well as to reducing the risk of HIV infection.8 In separate studies in Ghana and Nigeria, using mystery clients, young clients were neither treated with the same level of respect as older clients, nor were they given detailed information as their older counterparts. Authors speculate that differences in treatment by providers were due to providers' negative attitudes regarding young unmarried women who are sexually active.5,7 In addition to provider negativity, young people said that cost of services represents a barrier to service, fear that services are not confidential, as well as fear of meeting their parents or other adults they know at the facility.10-12 A number of these studies speculate that adolescents' reproductive health needs would be better served in service environments specifically for them, such as youth-only clinics or youth centres. Several organisations such as the World Health Organization and Focus on Young Adults have compiled what they see as fundamental characteristics of youth-friendly services.13,14 These include provider characteristics, facility characteristics and aspects of programme design. Characteristics that were often mentioned as necessities include:
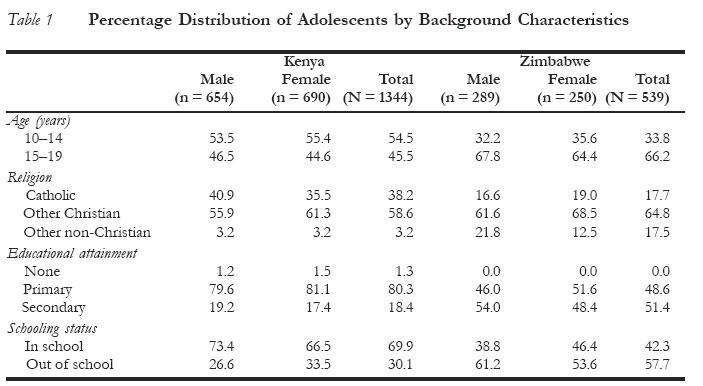
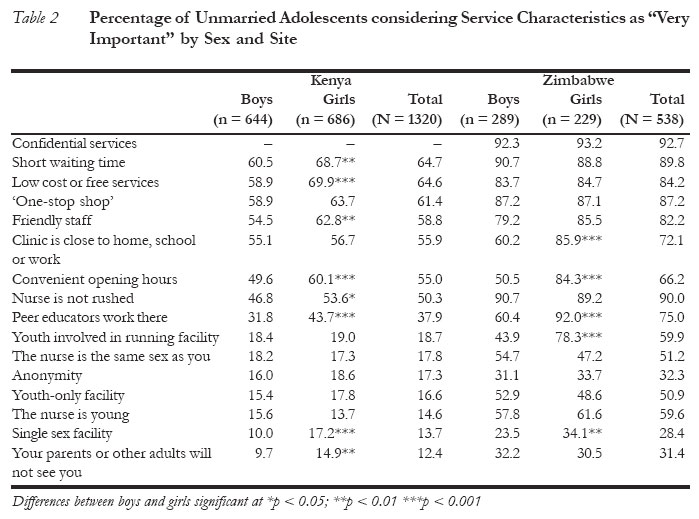
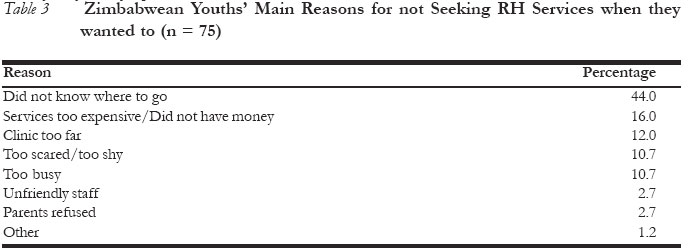
Some studies from the developed countries have quantified young people's preferences for reproductive health services. In two studies, one from the US and the other from Iceland, young people rated non-judgmental providers, short waiting time, a provider that does not rush but takes time with the client, and low-cost or free services, as the most important aspects of youth-friendly clinical RH services.15,16 Most of the remaining evidence concerning what young people consider youth friendly, especially for young people in developing countries, comes from qualitative data or, at times, evidence that is anecdotal. One study conducted in South Africa reflected young people's strong preference for youth only services and for providers that were friendly and judgment-free. However, this qualitative study was conducted among attendees of youth centres, which would likely result in respondents' biasness toward this model.4 A qualitative study in Zimbabwe found that youth preferred stand-alone, youth-only facilities,17 while another in Uganda found that they preferred upgrading existing services and facilities and retraining personnel, rather than establishing separate facilities for young people.11 Conversations with adolescents in West Africa suggested that they would prefer not to meet older people at the clinic, that they often get an unfriendly reception, and that they could afford the cost of services that are offered.10 Qualitative research in Kenya has suggested that young people's preferences vary widely and are often contradictory, with some preferring services at a distance from their communities, while others prefer services closer to their home. Youth in the urban areas preferred education from peers, while those in the rural areas preferred to get information from people older than themselves.18 Beyond scattered qualitative studies and anecdotes, little quantitative research has been devoted to understanding the relative importance of aspects of youth-friendliness to developing country young people, as well as to testing some of the assumptions about what programmers consider to be youth-friendly. Drawing on recognised aspects of youthfriendliness, this paper explores the relative importance of various aspects of services in the choice of facilities among young people in Kenya and Zimbabwe. Methods Data for this paper were obtained from largescale studies undertaken in Kenya and Zimbabwe. Initiated in 1997 in Zimbabwe and 1995 in Kenya, the studies tested the impact of community-based interventions aimed at reaching unmarried youth aged 10 to 24 years. In the context of these studies, baseline and endline surveys were carried out before and after youth activities were implemented. The current study utilises data collected from the endline surveys only. At endline, additional modules were added to the original questionnaire, including sections on preferences for reproductive health services. In Kenya, all households in the project site were listed in a house-to-house survey. Following this, households with eligible youth were selected for interview using a random number generator. In Zimbabwe, systematic random sampling was used where a sampling interval was calculated based on the number of households in the project site and the required sample size. In order to control for potential intra-household correlation, only one eligible youth was interviewed per household in both countries. Where there was more than one eligible youth in a household, the Kish grid was used to randomly select one of the youth for interview. In both countries, experienced interviewers were recruited and where possible interviewers who participated in the baseline survey were again used during the endline survey. For both countries, the interviewers spoke the local languages; some of them were residents in the study regions. The criteria used to select interviewers were, that they were young enough so that the respondents felt comfortable with them, and sufficiently open-minded so as not to be judgmental during the interviewing, especially on sensitive topics. Female interviewers interviewed female respondents while males interviewed male respondents. The surveys sought to assess the perceptions of young people on the importance of different aspects of RH services often considered youth-friendly. Respondents were asked: "I want you to think about a situation where you need services related to family planning, sexually transmitted diseases, or HIV/AIDS. I will read a list of characteristics of clinics. I want you to tell me if it is 'very important' that the clinic has this characteristic, 'important ' that the clinic has this characteristic, or 'not so important' that this clinic has this characteristic". The characteristics of clinics that programmers often consider youth-friendly were read to the respondents, after which they were asked to rate them according to level of importance. In Zimbabwe, confidentiality was included in the questionnaire as one of the characteristics, while in Kenya it was not. While the surveys in Kenya and Zimbabwe included respondents above the age of 20 years, analysis for this paper was restricted to unmarried adolescents aged 10-19 years. This was based on the fact that most prior work on youth-friendliness has focused on this group. Differences in preferences between boys and girls were examined, focusing on characteristics that were rated "very important" by respondents. Results A total of 1,344 never-married adolescents aged 10-19 years were interviewed in Kenya, while 539 adolescents were interviewed in Zimbabwe (Table 1). The Kenya sample was roughly evenly divided between younger adolescents aged 10- 14 years and older adolescents aged 15-19 years, while the Zimbabwe sample had twice as many older adolescents as the younger. Adolescents interviewed in Kenya were more likely to be Catholic (38%) than those in Zimbabwe (18%). At the same time, a considerable proportion of Zimbabwean youth were neither Catholic nor Christian, with most of them reporting that they had no religion (17%). Adolescents in both samples were highly educated, with none of the Zimbabwean adolescents reporting no education and only 18 respondents from Kenya reporting that they had never been to school. More Zimbabwean adolescents had reached secondary level education, which may be a reflection that the Zimbabwean sample is slightly older than the Kenyan sample. Overall, Zimbabwean adolescents were more likely to rate various service characteristics as 'very important', compared to Kenyan adolescents. Zimbabwean youth rated an average of 9.6 characteristics as 'very important' to them, compared to Kenya's 6.0. In both countries, of the 15 youth-friendly characteristics mentioned, girls were significantly more likely than boys to rate characteristics as 'very important'. On average, Kenyan girls rated 6.4 characteristics as 'very important' in their decision to choose one clinic in preference to another, compared to the boys who rated 5.5 characteristics as 'very important', a difference that was statistically significant. Among Zimbabwean youth, girls rated an average of 10.2 characteristics as 'very important', compared to boys, 8.9. The difference was also statistically significant. The fact that girls were more likely to rate service characteristics as 'very important' in their choice to visit a clinic could reflect that girls were more particular about clinical reproductive health services than boys. Given that premarital sex for girls is highly stigmatised in most parts of Africa, it would not be surprising if girls are more sensitive to where they get reproductive health services than boys. At the same time, it is possible that providers tend to be more judgmental and moralistic when girls present themselves for services, further contributing to girls' sensitivities. The rating of youth-friendly characteristics was similar for Kenyan and Zimbabwean adolescents. Staff attitudes, cost, short waiting time and the ability to obtain all services at one site (the 'one-stop shop' approach), emerged as the most important issues for youth. The most important characteristics for Kenyans were short waiting time, low cost or free services, the 'onestop shop' approach, and friendly staff. Among Zimbabwean adolescents, having confidential services, a nurse that takes her time, short waiting time, 'one-stop shop' approach, and low cost or free services were the most important charac-teristics (Table 2). The least important characteristics included facilities where adolescents are assured of anonymity or where their parents would not see them, having a youth-only facility, a nurse that is the same sex or young, a facility that is for youth only, and a single sex (girls only/boys only) facility. In the Zimbabwe survey, young people were also asked if there had ever been a time when they wanted to get RH services but could not do so. This question made possible the assessment of other environmental factors, outside of the clinic walls, that may keep young people from visiting clinics. Fourteen percent of the adolescents interviewed mentioned that they had not gone for services when they had wanted to, with most of them having interest in obtaining information or services on HIV/ AIDS. Majority (44%) of the adolescents did not obtain RH services because they did not know where to get such services (Table 3). The second most important reason for not seeking RH services was because services were too expensive, or they did not have the money to pay (16%). Twelve percent felt that the clinic was too far. Being too shy or scared was also a significant reason for not seeking services (11%), as well as being too busy (11%). Adolescents, therefore, face barriers to obtaining RH services that extend beyond the clinic walls. At the same time, cost-related reasons did keep them from accessing services. Being too busy or feeling the clinic was too far are related to the time spent in accessing services, which is also reflected in their desire for short waiting time while at the clinic. Discussion Increasingly, RH organisations are focusing their attention on youth, and considerable energy has been devoted to implementing youth-friendly services. However, little quantitative research has been conducted among adolescents in developing countries in assessing what is important to them in the context of clinical RH services. Such research is largely qualitative, which does not lend itself to prioritising the importance of service characteristics, or guiding the directions of programmes. At the same time, resources for adolescent programmes are limited, and in resource- poor settings, managers must make decisions about how best to appeal to adolescents with the limited funds available. This analysis revealed that many aspects of youth-friendliness are not as important to adolescents as commonly thought. Youth-only facilities, a hallmark of youth centres, do not rate highly in the service preferences of adolescents, yet considerable investment has gone into this model. Similarly, the involvement of peer educators or the involvement of youth in running programmes does not seem to be as high a priority as is commonly thought. What does seem to be important are service aspects that are important to adult clients also. Several studies of mainstream clinics have documented long waiting time, long distance to clinics, inadequate providerclient interactions, and insufficient time spent for consultation as problematic. Improving these aspects of clinical service does not require a considerable investment of external resources. Capacities readily available in the clinical setting can be harnessed to make facilities more attractive to young clients. These include staff commitment, ongoing self-assessment and internal reorganisation. These findings imply that in many developing country settings, existing facilities can be upgraded with minimal monetary investments to meet the RH service preferences of adolescents and make them youth-friendly. Such strategy is probably more feasible than establishing new, and often expensive, stand alone services for adolescents, such as youth centres. At the same time, clinic characteristics are not the only factors that prevent adolescents from seeking RH services, thus simply making facilities youth-friendly may not be sufficient to make youth visit them. Indeed, one study did find that community support for adolescent RH was a more important predictor of young people seeking RH services than was the quality of services.19 Not knowing where to go or being too scared to go can be important factors in preventing a young person from accessing the information and care they need. Such findings underscore the need for programmers to address other service barriers that may be more critical than facility characteristics such as environmental, community and psychosocial factors. Acknowledgements We wish to thank Ayo Ajayi and Placide Tapsoba for comments on earlier versions of this paper, as well as Lucy N'gan'ga for assistance with data processing. Funding for these studies was provided by the Rockefeller Foundation. REFERENCES
© Copyright 2005 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh05039t3.jpg] [rh05039t1.jpg] [rh05039t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}