 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 9, No. 3, December, 2005, pp. 100-111 Are Process Indicators Adequate to Assess Essential Obstetric Care at District Level? — A Case Study from Rufiji District, Tanzania Les indicateurs du processus sont-ils adéquats pour évaluer le soin obstétrique essential au niveau du district? Une étude de cas du district de Rufiji, Tanzaniae David P Urassa1,2, Anders Carlstedt2, Lennarth Nyström3, Siriel N Massawe1 , Gunilla Lindmark2 1Departments of Community Health/Obstetrics and Gynaecology,
Muhimbili University College of Health Sciences, Dar es Salaam, Tanzania. 2Department
of Women's and Children's Health, International Maternal and Child Health,
Uppsala University, Uppsala, Sweden. 3Department of Public Health
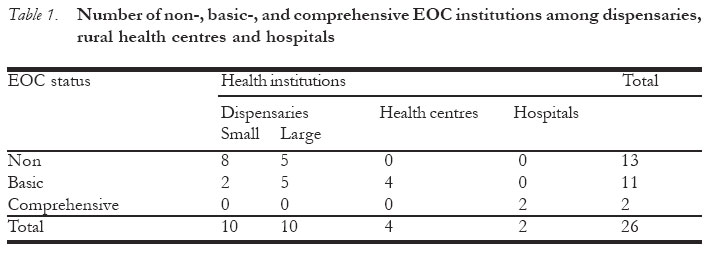
and Clinical Medicine, Epidemiology, Umeå University, Umeå, Sweden Correspondence: David P. Urassa, E-mail: durassa@muchs.ac.tz Code Number: rh05044 Abstract To assess coverage and quality of essential obstetric care (EOC) and the appropriateness of using process indicators, a 3-month follow-up study was done in Rufiji district, Tanzania, involving 2 hospitals, 4 health centres, 10 large dispensaries and 10 randomly selected small dispensaries. Data collection was done on process indicators as suggested by UNICEF/WHO/UNFPA (UN) and `unmet obstetric need (UON) for major obstetric intervention (MOI)'. With standard values in (brackets), the district had two comprehensive EOC facilities, births in EOC amounted to 62% (15%), met need for EOC was 76% (100%), caesarean section (C/S) rate 4.1% (>5%), hospital case fatality rate (CFR) 1.0% (<1%) and successful obstetric referrals 46% (100%). MOI for absolute maternal indication in the district was 2.6% (1-2%). All four maternal deaths occurred due to transport failures. The process indicators gave contradictory impressions on the coverage and quality of care and failed to link to the outcome of delivery complications in the study. (Afr J Reprod Health 2005; 9[3]:100-111 ) Résumé Afin d'évaluer l'étendue et la qualité du soin obstétrique essentiel (SOE) et le caractère approprié de l'emploi des indicateurs de processus, une étude d'une durée de trois mois qui est basée sur des suivis médicaux, a été menée dans le district de Rufiji, Tanzanie, auprès de deux hôpitaux, quatre centres médicaux, diz grandes pharmacies et dix petites pharmacies selectionnées au hasard. Les données ont été recueillies à l'aide des indicateurs du processus comme l'ont préconisé l'UNICEF/OMS/UNFPA(ONU) et "le besoin obstétrique non-satisfait (BON) à propos des interventions obstétriques principales (IOP)". Avec les valeurs normales (entre guillemets) le district disposait de deux structures de SOE, le taux de naissance par rapport au SOE s'est élevé à 62%(15%), le taux du besoin non-satisfait par rapport au SOE était de 76%(100%), le taux d'opération césarienne (OC) était de 4,1%(<5%), le taux du dècès des patients à l'hôpital (TDH) 1,0% (<1%) et les orientations vers les services spécialisés étaient de 46% (100%). L'IOP par rapport à l'indication maternelle absolue dans le district était de 2,6% (1-2%). Tous les quartre dècès maternels se sont produits à cause du manque de transport. Les indicateurs du processus ont signalé des impressions contradictoires en ce qui concerne la coverture et la qualité de soin et ils n'ont pas pu se lier au résultat des complications liées à l'accouchement dans l'étude. (Rev Afr Santé Reprod 2005; 9[3]:100-111) Key Words: Quality of obstetric care, met needs, process indicators, program evaluation, Africa. Introduction Monitoring of progress towards the reduction of maternal mortality will require reliable and internationally comparable data. Process indicators can provide useful information especially in countries with weak vital statistics 1. The conventional maternal and child health services have been criticised for emphasis more on the child than on maternal care 2. Maternal mortality ratio (MMR) in Tanzania is reported to be between 529 and 1500 per 100,000 live births 3-5. The main causes of maternal mortality are haemorrhage, abortion, hypertension, anaemia and sepsis 4, 6. Most maternal deaths occur as unpredictable obstetric emergencies, thus a strategy to achieve a substantial decline of maternal mortality must prioritise improvement in medical treatment of obstetric emergencies4. Reduction of maternal and perinatal mortality depends to a great extent on improved accessibility to quality obstetric services such as surgery and blood transfusion that can only be provided in hospital settings7, 8, but also on technically simple medical interventions for sepsis and bleeding. Maternal health has been monitored using outcome indicators such as the maternal mortality ratio (MMR). Where no comprehensive vital statistics exists, it is difficult and costly to get data for these indicators. Process indicators have been advocated since they are considered easier to measure and can give information on events that affect maternal mortality as well as activities needed to prevent it 1. An alternative approach is a system of process indicators expressed as Unmet Obstetric Need (UON)9. Several of these indicators are developed to compare the actual situation with estimated rates of complications and necessary interventions in the population. The main objective of this study was to assess the coverage and quality of essential obstetric care (EOC) in rural Tanzania and to discuss the appropriateness of these process indicators. Subjects and methods Study setting Rufiji district is one of the six districts of the Coastal region in Tanzania. In 1999 the district had an estimated population of 180,000, based on the 1988 Census and an annual population growth of 2.3%. Geographically the Rufiji River intersects the district from West to East, dividing it into flood plain, coastal-delta, and plateau (hill) zones. The roads in the district are not passable during the rainy season and the limited transport system makes people dependent on the available health services within the district. The district has 54 health institutions including private facilities that provide delivery services, out of which 48 are dispensaries, 4 rural health centres (RHC) and 2 hospitals. One of the hospitals is a government district hospital and the other is a voluntary hospital run by a religious organisation. Based on a birth rate of 4%, 7,200 births annually were estimated 10. Study design and study period This was a descriptive study of all institutional deliveries in Rufiji district during a 3-month period, from 15th November 1999 to 14th February 2000 i.e. during the dry season. Study participants and sampling All institutions were stratified by type of unit providing deliveries and number of deliveries, thus stratum I consists of all hospitals (n=2), stratum II of all RHCs (n=4), stratum III of all large dispensaries with more than five monthly deliveries (n=10), and stratum IV of 10 randomly selected out of 38 small dispensaries. The 26 units selected constitute 48% of all health institutions in the district. This fulfils the recommendations to cover at least 25-30% of the health institutions when assessing quality of care 1, 11. All women who attended the selected health facilities for delivery in the three-month duration were included in the study. Data collection Data collectors were the health workers at each selected health institution. An introductory meeting was held on the first day in each institution to familiarise the staff, explain the aim of the study and train them on data collection. It was emphasised that the research team was not representing the Ministry of Health and that the findings of this study would not be used against any of them. Standard diagnostic definitions for different complications were introduced in the training to be used uniformly by all the research assistants. Health workers were encouraged to record all the events occurring to patients reported with complications. The diagnoses were reviewed by a specialist obstetrician. If a woman had more than one complication the most immediately life-threatening was selected. We established a parallel data collection on information about complications since the routine data collection system reported delivery complications only as abnormal without specifying the type of abnormality. Information for quality assessment (i.e. structural, process and outcome variables) was collected. For structural quality, a standard checklist was developed and information on availability of the following items was collected monthly: number of qualified staff, functioning vacuum extractor, dilatation and curettage set, injectable antibiotics, oxytocics and anti-convulsant drugs, blood bottles, functioning operation theatre and blood transfusion facilities. Using UN process indicators 1 a form was filled for each woman with a delivery complication. Monthly visits by the investigator were made to all health institutions to collect data and to cross check and correct any discrepancy between the additional form and the routine data collection records of the institution. The forms of all women with complications were checked at all referral levels to avoid duplicates. Definitions and standards As trained staff were regarded as those who had at least two years of midwifery in their basic training, thus in this study a MCH aide (with two years of midwifery training) was the lowest cadre of trained staff. They are specifically trained for immunisation and growth monitoring of under fives and antenatal care at MCH clinics, as well as to conduct low risk deliveries and to immediately refer women with complications. Met obstetric need The UN indicators define as obstetric complications antepartum (APH) and postpartum (PPH) haemorrhage, prolonged/obstructed labour, postpartum sepsis, complications due to abortions, pre-eclampsia/eclampsia, ectopic pregnancy and ruptured uterus. Basic EOC functions include providing injectable antibiotics, injectable oxytocics, injectable anti-convulsants, manual removal of placenta, removal of retained products, and assisted vaginal delivery. Comprehensive EOC functions include all six basic functions and also C/S and blood transfusion. Minimal acceptable levels of EOC are:
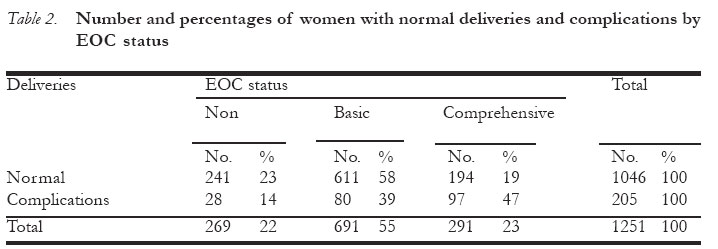
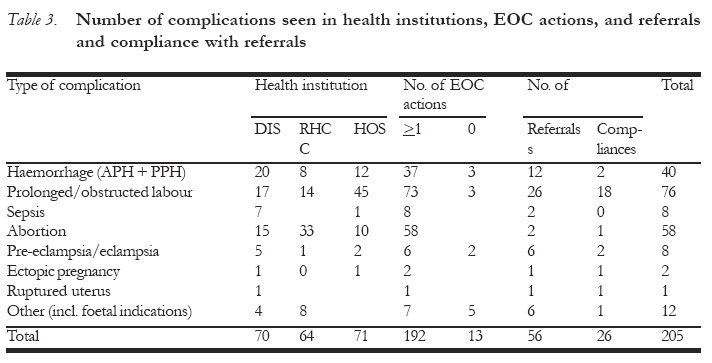
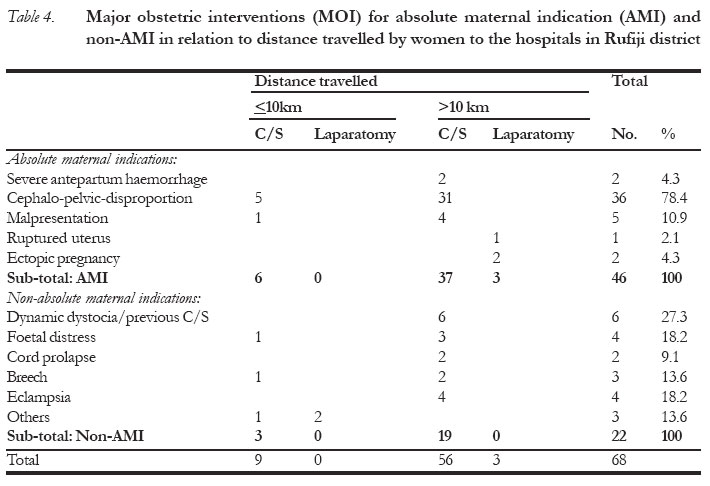
In the preliminary analysis we found that most institutions had not handled all types of complications in the study period and therefore had not performed all types of recommended interventions. We therefore combined structural and process indicators of quality to modify the UN definition of basic and comprehensive EOC based on the assumption that in the presence of standard drugs and the skills required to inject/deliver those drugs (antibiotics, oxytocics and anti-convulsants) the facility qualified for EOC. Thus, a basic EOC institution was defined as one that had the required injectables in stock and had performed parenteral administration of any one of the drugs, and in addition had performed either one of the following minor surgical procedures: removal of placenta, evacuation of retained products, or assisted vaginal delivery, i.e. vacuum extraction/forceps delivery. A comprehensive EOC institution was defined as an institution that, in addition to basic EOC requirements, had provided blood transfusions and surgery within the period of study. Unmet obstetric need (UON) The UON indicators define major obstetric interventions (MOI) in relation to absolute maternal indications (AMI), which can only be performed in hospitals to include: C/S, laparotomy, hysterectomy, internal version and craniotomy. Absolute maternal indications are severe APH, severe PPH, major Cephalo-pelvic disproportions (CPD), transverse position and brow presentation. The concept of reference ratio (RR) of 1-2% deaths of all deliveries has been used to mean the maximum expected maternal mortality ratio (MMR)in areas with no maternal care9 and therefore need a corresponding MOI for AMI to avert maternal deaths. The complications and interventions presented at hospital level were therefore re-categorized to fit into the UON classification. Only women residing in the study area were included and no MOI for AMI was performed on the study population outside of the district. Applying the RR on the number of expected births (EB) per catchment population, gives the expected number of women who should have had a MOI for the above-mentioned AMI. Unmet obstetric need was calculated using the formula: UON = (EB x RR) - (MOI for AMI). Ideally, the RR should be established locally. Since we did not have MOI for AMI, RR for Tanzania we used a benchmark of 1 -2% as suggested in studies from Morocco 12 and Mali (1.2%)13. NB: The Moroccan study was the first of its kind to utilize the UON concept and the established reference ratio from this study was recommended to be used in other areas of similar characteristic where local reference ratio was not yet established. Results Coverage The study population covered by the catchment population of the selected 26 health facilities was 155,000, and that is 86% of the 180,000 estimated district population. Figure 1 highlights a diagrammatic presentation of delivery or pregnancy complication information in the study area during a 3-month period of data collection. In that period, there were 1,427 women of whom 176 had normal home deliveries and 1,046 uncomplicated institutional deliveries. Two hundred and five women were managed by the health-care system due to delivery or pregnancy complication. The complications included 58 abortions and two ectopic pregnancies (total 60) and therefore total number of deliveries was 1,367 (1,427 minus 60). Adjusting for the coverage of 86% of the population, the total number of deliveries in the district was estimated at 1,587. Whereas two dispensaries had a shortage of the three essential EOC drugs, all RHC and hospitals had these drugs. Unlike all health centres and hospitals, where all the required interventions were performed, more than half of the dispensaries performed neither parenteral administration of one of the drugs nor any minor surgical intervention within the 3-month study period. Both hospitals qualified for comprehensive EOC, whereas all RHCs but only five out of 10 large and two out of 10 small dispensaries qualified for basic EOC (Table 1). Met obstetric need using UN indicators In the three-month period, 72% ((691 plus 291)/1,367) of all observed births or 62% (982/1,587) of the expected number of births took place in EOC institutions being far in excess of the 15% reference given for the UN indicators (Table 2). Out of women with recorded complications 86% (177/205) were managed at EOC institutions, which is 74% (177/238) of the expected number for the whole district (met need). Among the complications 71 were self-referred to hospital and 134 attended a RHC or a dispensary, of which 78 were managed there and 56 were referred to hospital (Figure 1). The most common complication managed at dispensaries was postpartum haemorrhage, whereas abortions were most prevalent at the health centres. Prolonged/obstructed labour was the most common obstetric complication among women who were primarily seen at hospital level, and this complication was also the predominant cause of referral (Table 3). Our analysis of the case management of complications indicates that treatment was adequate even in small dispensaries that did not qualify as basic EOC units. No maternal death can be attributed to mismanagement at dispensary or health centre level. The four women with complications who died during transport or shortly after arrival in hospital (see below) were all referred as emergencies from basic EOC facilities. The referral diagnoses were postpartum sepsis (1), imminent rupture of the uterus in "grand multipara"(1) and Cephalo pelvic disproportion (2). Fifty-six patients were referred to hospital; however 30 did not arrive at either of the two hospitals. Twenty-two of these women were traced and interviewed for their outcome in the community. Three died on the way to the hospital, whereas 19 had delivered at home or on the way to hospital. The only hospital death occurred in a woman arriving at the government hospital with a ruptured uterus, after waiting more than three days for transport. Thus, all maternal deaths in this study can be attributed to lack of transport and/or inability to pay for hospital care. This was confirmed by interviews with women who did not adhere to the referral advice (see below). Considering the 3 women who died during transport and 4 who delivered on the way to the referral point, the referral compliance rate was 59% (that is 26 who arrived at hospital plus 7 who either delivered or died on the way to hospital divide by 56) (Figure 1). The reasons given for not complying with the referral advice among the 19 were: "No money for the hospital" (9), "No money for transport" (2), "No money" unspecified (4), "Delivered on the way" (2), and "No reason" (2). Unmet obstetric need by UON indicator Ninety-seven women, including 26 referrals, were treated in the two hospitals due to complications. Sixty-eight of these women underwent major obstetric interventions (MOI) i.e. C/S or laparatomy. The majority of absolute maternal indications were cephalo-pelvic disproportion (CPD). Non-absolute maternal indications (Non-AMI) included all dynamic dystocia, e.g. prolonged labour without documentation of obstruction (Table 4). Table 5 presents the unmet need of MOI for AMI in Rufiji by distance travelled by women to the hospitals. The MOI/AMI rate per 100 expected births (EB) was 2.5% for mothers residing more than 10 km from the nearest hospital and 3.0% for women living closer to hospitals however the difference was not significantly (p = 0.65). These rates were all above the UON reference of 1%. Caesarean rate The C/S rate in the whole district was 4.1% (65/1,587) which is lower than the minimum recommended of 5%. Accessibility The distance travelled by a patient who attended hospital was estimated from the centre of the administrative subdivision in which the patient's village was located to the respective hospitals. The median distance between the patient's village and the hospital was 20 km (Range 1-150) and the median time to access a comprehensive EOC institution was 45 minutes (Range 15-540). This, however, did not include the waiting time for finding means of transport. Case fatality rate (CFR) There was one death in hospital in 97 complicated cases, i.e. the hospital-based CFR was 1.0%. However, there were 3 reported maternal deaths of women who had been seen at the lower level of care during the three-month period and referred to hospital level but died before arrival. Thus, the overall CFR was 2.0% (4/205). Discussion More than 85% of the deliveries in the study area took place in institutions, which is an unusually high figure for a developing country and much higher than the 55% reported from northern Tanzania 14. There may be several reasons for this finding, including a community health project in this area since 1997 and that may have had positive effects on the community perceptions of the quality of maternal care in institutions 15. In any case, the high rate of institutional deliveries makes the Rufiji district suitable for studies on quality of obstetric care. It also shows that accessibility was good during the study period. A study during one year would be needed to study seasonal variations in accessibility due to the rainy seasons. Women with delivery complications, especially those with a previous history of a C/S, tended to bypass lower levels as "self-referrals" to the nearest hospital. About 40% of women with complications were referred to hospitals from peripheral units but less than half of them arrived, indicating a poor compliance with referrals. In spite of a high proportion of institutional deliveries and good access to well-functioning hospitals, four maternal deaths occurred. This indicates that the whole health-care system does not function well. Our study reveals that the referral system must be improved to lower maternal mortality. Other studies16, 17 have shown that training traditional birth attendants (TBAs) and integrating them into the health-care system could reduce perinatal and maternal mortalities and reduce unnecessary obstetric interventions. However, given the existing situation in this study, very little could have been achieved by trained TBAs without a transport. Assessment of quality of care should be based on the inter-relationship between structure, process and outcome components of a health intervention and no single dimension alone is sufficient to measure quality of care.18 Both hospitals in the district qualified as comprehensive EOC institutions, which is sufficient according to UN indicators. If UN indicators were strictly adopted, however, no institution below hospital level would have qualified as a basic EOC institution and only one of the hospitals as a comprehensive EOC unit. This illustrates that these indicators are less applicable in small units and limited observation periods, and was the rationale for the structural-process quality modification adopted in this study. We developed a parallel data collection, since the routinely collected data, especially below hospital level, were not appropriate for the study. Furthermore, our findings indicate that routine data may not be sufficient for assessing quality of care using UN or UON indicators. The proportion of all deliveries in EOC institutions in our study was above the minimum level of 15% recommended by the UN guidelines. It may be questioned whether this indicator is realistic 19. This would require that all complications and complications only are delivered in EOC institutions, which is an unrealistic assumption. In our study, by using this definition, the met need for obstetric care of 62% was considerably higher than reported from Mozambique, Nepal, Senegal 20 and Eritrea 21. Under-reporting of obstetric emergencies and over-reporting due to double counting have been observed in a system developed to monitor obstetric services in Malawi 22. A comprehensive parallel data collection, as the one instituted in this study may be more reliable. The problem of definition of obstetric complications is another reason for variations in the met need indicator. In the study area, the cut-off point for diagnosis of haemorrhage was blood loss in excess of 500ml. The amount of bleeding was based on the perception of health workers and patient's since measurement tools were not used. Inconsistencies in the definition of blood loss have also been reported by Goodburn, et. al. in Malawi 22. Complications of abortion included infection or persistent haemorrhage, requiring evacuation of retained products. In settings where cases of abortions are common, this could contribute to an inflation of the met need indicator since only few abortions really need any intervention 23. In countries like Tanzania, where induced abortion is illegal these cases may be labelled as complications of spontaneous abortion to cover for the legal aspect. The diagnostic difficulty to separate cephalo-pelvic disproportion from other causes of prolonged labour is another notorious problem, especially when partograms are not used. The rate of C/S (4.1%) in our study is slightly lower than 4.6% reported from six districts in northern Tanzania 14. Also to the recommended minimum of 5%. The assumption that when the C/S rate is low, the majority of operations are done for maternal indication may not be valid. In our case, at least 12% of the C/S was done on foetal indications. A large variation in the proportion of sections performed for maternal indications has been reported in Senegal, where the rate of C/S is as low as 1.2, and from many countries a relatively low MMR has been reported with a C/S rate of less than 2.5% 19. A rise in the C/S rate does not necessarily indicate progress in reducing maternal mortality and fixing the arbitrary minimum rate of 5% may not be adequate if only maternal mortality is addressed. The CFR is an indicator of quality of emergency obstetric care at hospital level 1. In our study, only one death occurred shortly after arrival to hospital in 97 complicated cases, which is in accordance with UN indicators of acceptable quality. Maternal death or near-death audits, may help improving case management 20. The hospital CFR is of limited significance where a large proportion of complicated obstetric cases are, as in this study, delivered outside health institutions. Three maternal deaths during transport highlighted the importance of the referral system for maternal mortality and therefore should also be assessed in relation to quality of obstetric care. Unmet obstetric need Considering UON indicator and a reference ratio of 1-2% maternal mortality ratio for a population without access to any obstetric care 9,12 if major surgical interventions in a study area (usually C/S) are below 1.0%, this would be regarded as an "unmet obstetric need". Conversely, major interventions in excess of 2.0% would indicate that operative deliveries are made on other indications than to avert maternal mortality. Our finding of four maternal deaths in the study area, despite the MOI for AMI ratio of 2.5% for mothers residing more than 10km from the nearest hospital and 3.0% for women living closer to hospitals, may indicate limitation of this indicator for quality assessment as a management tool at district level. The method is further limited by the difficulties involved in a retrospective differential diagnosis between obstructed labour that is directly life-threatening to the mother and less severe disproportions that may cause considerable maternal morbidity. The indicators of Met need (UN) and Unmet Obstetric Need (UON) are designed to identify whether women who need obstetric care really receive it. Both indicators are based on the diagnosis of direct obstetric complications that may need a skilled provider. For the Unmet need indicator the reference ratio, usually 1-2%, is far below the 15% used for the Met need indicator. To transform one into the other is very difficult. The UON reflects near-death maternal complications, and is thus more closely related to the reduction of maternal mortality. However, it does not include non-surgical but life-saving, medical interventions, or such a common procedure such as removal of retained placenta. Furthermore, the reference rate estimated from an urban population with good access to hospital care makes it less valuable in a rural setting with restricted access to care and weak referral systems. Conclusion This study has demonstrated the inadequacy of UN and UON-network process indicators in monitoring the activities necessary to reduce maternal mortality in a low-resourced country setting. Using the UN and UON process indicators, we got contradicting results of met and unmet need for obstetric services observed in Rufiji district. The process indicators did not clearly identify areas for improvement and hence other sources of information, including community based data and individual case audits, will be necessary to complete the information from these indicators. The study shows that poor perfor-mance of the referral system may cause an unacceptably high maternal mortality, in spite of good access to well functioning institutions. The study calls for more research on factors influencing compliance with referral advise as well as to establish more well-defined indicators linked to activities for reducing maternal mortality. Acknowledgement We are grateful to the District Medical Officer of Rufiji district and all health workers/data collectors who supported and participated in this study. We thank Kerstin Carlstedt for her expert assistance in data entry and management. This study was funded by Swedish Agency for Research and Co-operation with Developing Countries (SAREC) under collaboration between MUCHS, Tanzania, and Uppsala and Umea Universities of Sweden. References
© Copyright 2005 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh05044t5.jpg] [rh05044t1.jpg] [rh05044t4.jpg] [rh05044t3.jpg] [rh05044t2.jpg] [rh05044f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}