 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
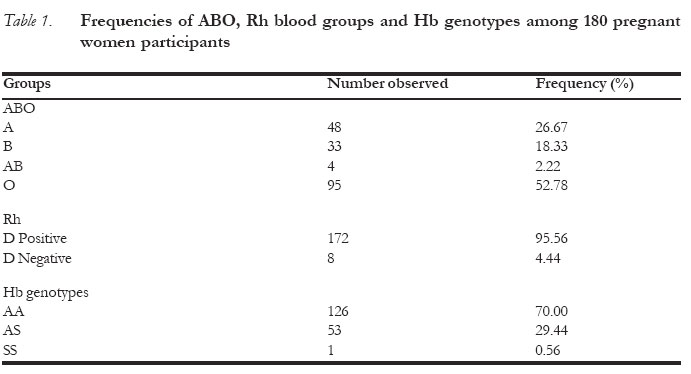
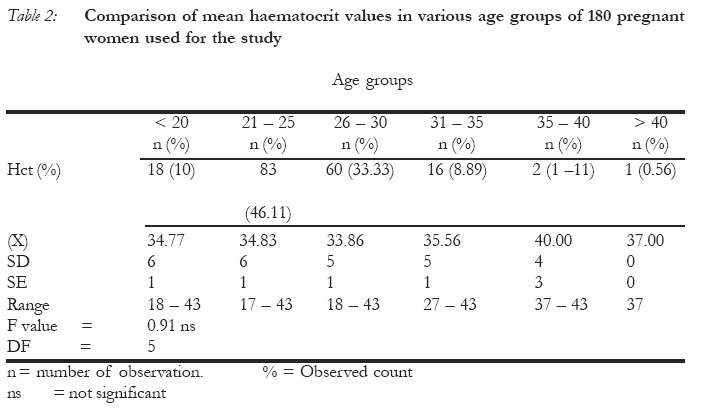
African Journal of Reproductive Health, Vol. 9, No. 3, December, 2005, pp. 112-117 An Assessment of the Clinical Utility of Routine Antenatal Screening of Pregnant Women at First Clinic Attendance for Haemoglobin Genotypes, Haematocrit, ABO and Rh Blood Groups in Port Harcourt, Nigeria Evaluation de l'utilité clinique du test de dépistage prénatal de routine auprès des femmes enceintes pendant la première consultation pour les génotypes d'hémoglobin, hématocrite, les groupes ABO et les groupes sanguins RH à Port Harcourt. Zaccheaus Awortu Jeremiah Correspondence: Z. A. Jeremiah, MSc. AMLSCN. P. O. Box 1437, Diobu, Port Harcourt. Rivers State, Nigeria. Phone: +234 - 803 - 4045636. E-mail: zacjerry@yahoo.com. Code Number: rh05045 Abstract This prospective study was designed to provide the frequencies of the haemoglobin genotypes, ABO and Rh blood groups and their effects on the haematocrit values among pregnant women in Port Harcourt. One hundred and eighty (180) pregnant women at their first clinic attendance and in their first pregnancy (parity - 0) participated in this study. The overall frequencies obtained for ABO and Rh blood groups were: 26.67% for group A, 18.33% for B, 2.22% for AB and 52.78% for O. Rh D positive was 95.56% while Rh D negative was 4.44%. The frequencies of haemoglobin genotypes were 70.00% for HbAA, 29.44% for HbAS and 0.56% for HbSS. HbAC and SC did not occur in this study population. The mean haematocrit value was 34.64%. This was found to be independent of the ABO and Rh blood groups (P>0.05). On the other hand, haemoglobin genotypes were found to exert significant effects on the haematocrit values (F = 8.01, P = 0.0005). No significant relationship was found to exist between age and the haematocrit values. (F = 0.91, P > 0.05). Since pregnancy in sickle cell disease is associated with morbidity, proper antenatal monitoring and counselling will be necessary to prevent fatal outcomes. (Afr J Reprod Health 2005; 9[3]:112-117) Résumé Cette étude perspective a été conçue afin de fournir les fréquences des génotypes d'hémoglobin, les ABO et les groupes sanguins Rh et leurs effets sur les valeurs hématocrites chez les femmes enceintes à Port Harcourt. Cent quatre-vingt (180) femmes enceintes au cours de leur première consultation prénatale et pendant leur première grossesse (parité-0) ont fait partie de l'étude. La fréquence totale obtenue à l'égard d'ABO et les groupes sanguins Rh étaient de 26,67% pour le groupe A, 18,33% pour le groupe B, 2,22% pour AB et 52,78% pour O. le Rh D positif était de 95,56% alors que Rh D négatif était de 4,44%. Les fréquences des génotypes d'hémoglobin étaient de 70,00% pour HbAA, 29,44% pour HbAS et 0,56% pour HbSS. Le HbAC et SC ne s'étaient pas produits au sein de cette population étudiée. La valeur hématocrite moyenne était de 34,64%. On a trouvé que celui-ci était indépendant des groupes sanguins ABO et Rh (p>0,05). Par ailleurs, on a trouvé que les génotypes d'hémoglobin exercent des effets importants sur les valeurs hématocrites (F=8,01, P = 0,0005). Aucun rapport important n'existe entre l'âge et les valeurs hématocrites. (F= 0,91, P = 0,05). Puisque la grossesse chez les femmes souffrant de l'anémie drépanocytaire est liée à la morbidité, il faut une bonne surveillance et une bonne consultation pour éviter les conséquences fatales. (Rev Afr Santé Reprod 2005; 9[3]:112-117) Key Words: Antenatal, pregnant women, Haemoglobin genotypes, ABO, Rb, blood groups, Heamatocrit Introduction The first antenatal clinics which were introduced between 1910 and 1915 in Australia, Scotland and the United States, represented a new concept of care for pregnant women vis-a-vis the monitoring of apparently healthy women for signs of illness in order to reduce maternal deaths (1). To achieve this noble objective, mandatory tests were introduced on antenatal mothers at first attendance to clinics. Some of these mandatory tests as they relate to the haematology laboratory are ABO and Rh blood groups, haemoglobin genotypes and packed cell volume (haematocrit). Available data has it that one in every 150 African-American couples in the United States is at risk of giving birth to a child with sickle cell disease (SCD) (2), which hitherto has been a major contributor to the highest mortality rate among children from one to ten years in high prevalence areas. (3) Geographic distribution of sickle cell disease revealed 1 – 10% HbSS, 15 – 30.5% HbAS and < 1% SC for Africa. West Africa and Nigeria recorded a higher prevalence of 40.5% for HbAS which appears to be the highest in the world (4). The clinical importance of the ABO and Rh blood group systems in haematology relates to the capacity of alloantibodies (directed against antigens not possessed by the individual) to cause destruction of transfused red cells or to cross the placenta and give rise to haemolytic disease of the new born. (HDN)(5). In Nigeria, most published reports on pregnancy and haemoglobinopathies are centred on the outcome of pregnancies associated with these inherited conditions of which anaemia is paramount, and most of these studies were carried out among the Yoruba in the Western part of Nigeria (6 - 9). There is scarcity of information on this subject in Port Harcourt, South - South of Nigeria, hence the prevalence of sickle cell haemoglobinopathies, ABO and Rh blood groups in pregnancy could not be fully ascertained. It is also thought that some of these independent variables tested during antenatal visitsmay have an overall effect on the haematocrit values of these pregnant women. The extent to which these factors interact to influence the dependent variable (haematocrit) is not fully known. This study therefore attempts to provide the frequencies of ABO and Rh blood groups and haemoglobin genotypes in this obstetric population and also to study the effect of these factors on the haematocrit values of the pregnant women. Materials and Methods Setting and design This study was carried out in a primary health demonstration centre, College of Health Science and Technology in Rumueme Community, Port Harcourt, South-South, Nigeria. Due to its strategic position, the health centre, serves both students and the community, thus the pregnant women who participated in this study were all from the host community and its environs in the Port Harcourt metropolis. It was a prospective study with completely randomised design. Only 180 pregnant women at their first clinic attendance and first pregnancy (parity - O) were selected for the study. Their age ranged from 17 - 44 years. Methods Two millilitres of venous blood were collected into potassium ethylene diamine tetracetic acid (EDTA) salt and used for all the parameters tested. Haematocrit values were estimated with the microhaematocrit centrifuge (Hettich, Germany). The well-mixed venous anticoagulated blood was allowed to fill two plain capillary tubes for each sample to 2/3 length. One end of the capillary tube was sealed with plasticine, placed in the micro haematocrit centrifuge and spun at 10,000 rpm for 5 minutes. At the end of 5 minutes, the spun tubes were removed and values read with microhaematocrit reader. Results were expressed as percentage (%).(10) Haemoglobin electrophoresis was performed on each sample with cellulose acetate paper at pH 8.9. The procedures were followed as described by Brown (1980) (10). ABO and Rh blood groups of the antenatal mothers were determined by haemagglutination method (tube) with anti-A, anti-B, anti-A+B and anti-D monoclonal antibodies (Biotec, Suffolk, UK) bought from the Nigerian market. Red cells were phenotyped according to standard procedures as described by Judd (11) and Brecher (12) Statistics Data were analysed using the statistical analytical software (SAS). Frequency procedure of SAS was employed for frequency distribution of blood groups and haemoglobin genotypes. General linear model (GLM) procedure of ANOVA was used for the separation of means and for assessing the effect of other parameters, ABO, Rh, haemo-globin genotype and age on the haematocrit values. Significant level was set at alpha 0.05 (P < 0.05). Results: The overall frequencies of the haemoglobin genotypes, ABO and Rh blood groups in the 180 participants are shown on Table 1. Frequencies obtained were as follows: 26.67% for blood group A, 18.33% for B, 2.22% for AB and 52.78% for O. Rh D positive accounted for 95.56%, while Rh D negative was 4.44%. The frequencies of haemoglobin genotypes were 70.00% for HbAA, 29.44% for HbAS and 0.56% for HbSS. HbAC and SC did not occur in this study population. Table 2 shows the comparison of mean haematocrit values in the various age groups of the participants. There was no statistically significant relationship existing between age and haematocrit values (F = 0.91, P> 0.05). Also, pregnant women 83 (46.11%) of the age group 21 - 25 years constituted the majority in the study population. Discussion This study was designed to evaluate a typical African obstetric population for the frequency of the most clinically relevant and routinely tested blood groups, haemoglobin genotypes and haematocrit values. It was also designed to study the effects of these independent variables on the haematocrit values. The frequencies of the ABO blood group in the study population were: 26.67% for group A, 18.33% for B, 2.22% for AB and 52.78% for group O. These values were found to vary significantly when compared with values from other races. For instance, in Western Europe, 42% have group A, 9% group B, 3% group AB and 46% group O(13). Values obtained from South-Western Germany, 43.26% for group A, 10.71% for group B, 4.82%4.82% for group AB and 41.2% for group O, (14) also show a wide variation from the results obtained in this study. Generally, the frequency of O blood group in this study was found to be higher than all the Caucasian values, implying that the majority of the women in our obstetric population are of blood group O. On the other hand, the frequency of group A in this study appears to be lower than the Caucasians. However, results obtained in this study have been found to be consistent with values obtained from South-Eastern parts of Nigeria (15). Values obtained from other parts of Nigeria, however, showed little variations (16). Generally, group O red cells can be given to A, B, AB and O recipients and were formally inappropriately called `Universal donors' (17). The moderate frequency of group O in this obstetric population provides an advantage in terms of availability of blood for transfusion, especially in emergencies arising from obstetric complications. However, if the transfused units contain potent immune haemolytic antibodies (haemolysins), such neutralisation and dilution effect may be insufficient and may lead to marked destruction of A and B cells of the recipient(17). For this reason, the practice of transfusing group O blood to non-group O recipients is strongly discouraged. Routine haemolysin test as an additional test to complement routine ABO testing ought to be mandatory even though pregnant women are always recipients rather than donors. This will help to reduce the risk of transfusion reaction. The frequency of Rh D positive was 95.56% while that of Rh D negative was 4.44%, Rh negativity has been documented to be primarily a Caucasian trait (18). In most Caucasian population, the incidence of Rh negativity is 15 - 16% while that of Finland is 10 - 20%. In Chinese and Japanese populations, it is less than 1%. In blacks, the incidence ranges from 4 to 8%, being higher in North American than in African blacks(18). The result of this study is similar to an earlier study in Port Harcourt general population where 5% were tested to be Rh D negative(19). The 4.44% D - women in this study stand the risk of developing anti-D which can cause both moderate and severe form of haemolytic disease of the newborn. The frequency of haemoglobin genotypes in this study were HbAA (70.00%), HbAS (29.44%) and HbSS (0.56%). This observation is similar to that of Nwafor and Banigo(20) who recorded 73% for HbAA, and 22% for HbAS in Rivers State, Nigeria. HbSS of 4% recorded in their study is, however, at variance with the result of this study where only 0.56% was obtained for HbSS. It is of specific interest to note that the prevalence of HbSS in this obstetric population is quite low when compared to other studies where 4%(20) and 3%(21) have been recorded in Nigeria. Apart from the small sample size in this study, other factors like improved socio-economic conditions and educational awareness could possibly contribute to this low prevalence. A population based study for the prevalence of HbSS may be needed to confirm the low prevalence of HbSS recorded in this study. The mean haematocrit values obtained in this study was 34.64%. Analysis of data with general linear model (GLM) procedure of ANOVA revealed that age, ABO and Rh blood groups do not have any effect on haematocrit values. A significant effect of haemoglobin genotypes on haematocrit values was, however, observed. (F = 8.02, P= 0.0005). Sickle cell anaemia is an inherited blood disorder, characterised primarily by chronic anaemia and periodic episodes of pain. The underlying problem involves haemoglobin, a component of the red cells in the blood. In sickle cell anaemia, the haemoglobin is defective. After the haemoglobin molecules give up their oxygen, some of them may cluster together and form long rodlike substances. These structures cause the red blood cells to become stiff and to assume a sickle shape. Sickled red cells die after only about 10 - 20 days, because they cannot be replaced fast enough, the blood chronically become short of blood cells - a condition called anaemia(4). Since pregnancy in sickle cell disease is associated with increased morbidity and mortality,(22)-(24), proper antenatal monitoring of pregnant mothers at risk and counselling are necessary to prevent fatal outcomes. Acknowledgement The author is grateful to all the staff in the School of Medical Laboratory Sciences, College of Health Science and Technology for assisting in sample collection. The Community Health Staff in the Health Centre also gave me the needed help. References
© Copyright 2005 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh05045t2.jpg] [rh05045t1.jpg] |
| |||||||||

{kind=link}
{kind=link}