 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 9, No. 3, December, 2005, pp. 128-136 Socioeconomic and Reproductive Factors Associated with Condom Use Within and Outside of Marriage Among Urban Pregnant Women in Zambia Facteurs de reproduction et socio-économiques liés à l'usage du condom dans le mariage et hors de mariage chez les femmes urbaines enceintes en Zambie. Chipepo Kankasa, MD, PhD1, Margaret Siwale, MD, PhD1, Francis Kasolo, MD, PhD2, Ayako Nishiyama, MD, MHSc3, Hiroshi Terunuma, MD, PhD4 and Naomi Wakasugi, MD, PhD3 1Department of Pediatrics, University Teaching Hospital, Lusaka,
Zambia. 2Virology & Immunology Laboratory, University Teaching
Hospital, Lusaka, Zambia. 3Graduate School of Political Science,
Waseda University, 1-6 Nishiwaseda, Shinjuku-ku. 4Department of
Microbiology, Yamanashi University School of Medicine, Yamanashi, Japan Correspondence: Naomi Wakasugi, MD, PhD, Professor, Graduate School of Political Science, Waseda University, 1-6 Nishiwaseda, Shinjuku-ku, Tokyo, 169-8050, Japan. E-mail: nwakasu@ri.imcj.go.jp Tel: 81-3-3202-7181,ext.2857; Fax: 81-3-3202-7364; Code Number: rh05047 Abstract A cross-sectional questionnaire survey was conducted on 470 pregnant women in Lusaka, Zambia. Multivariate analysis revealed school attendance and child deaths as independently significant variables positively associated with HIV seropositivity. Among women with fidelity, HIV prevalence was not significantly lower, and condom use was much lower than among women who were having extramarital affairs. Factors significantly associated with condom use within and outside of marriage differed-age and number of live births within, and sexual transmission knowledge outside of marriage. School attendance was not effective for gaining knowledge on sexual transmission or condom use. Regular own earning was significantly effective for condom use in both groups, irrespective of school attendance. The following should be implemented intensively: effective education on HIV and sex in and out of school before early sexual debut, further implementation of family planning with emphasis on condom use, and empowering women by assisting with their economic independence. (Afr J Reprod Health 2005; 9[3]:128-136) Résumé Une enquête transversale basée sur un questionnaire a été menée auprès de 470 femmes enceints à Lusaka en Zambie. Les analyses multivariables ont montré que la fréquentation à l'école et la mortalité infantile sont des variables importants liés à la séropositivité du VIH. Parmi les femmes fidèles, le niveau de fréquence n'était pas inferieur de manière significative et le taux de l'usage du condon était moins élevé chez elles que chez les femmes qui trompaient leurs maris. Il y avait une différence à l'egard de l'âge et nombre de naissance vivantes dans le mariage et la connaissance de la transmission sexuelle hors de mariage ou l'usage du condom. La fréquentation à l'école n'était pas effective quant à l'acquisition de la connaissance sur la transmission sexuelle ou l'usage du condom. Un salaire personnel et régulier bien efficace pour l'utilisation du condom pour les deux groupes, que l'on fréquente l'école ou non. Il faut une mise en oeuvre rigoureuse des propositions suivantes: une éducation efficace du VIH et de la sexuelité dans l'école et hors de l'école avant le commencement précose de la vie sexuelle, une réalisation davantage de la planification familiale en mettant l'accent sur l'utilisation du condom et la capabilisation de la femme en l'aidant à accéder à l'independance économique. (Rev Afr Santé Reprod 2005; 9[3]:128-136) Key Words: Zambia, HIV, Condoms, Extramarital relationships, Income Introduction The global burden of HIV infection is increasingly shifting to women and children.1 This trend is a real and serious threat, particularly in Africa where infected females outnumber infected males1, 2, and the fertility rate is very high3. Zambia is no exception, since the estimated HIV prevalence rates among young people (15-24 years of age) are 16.8% - 25.2% for women and 6.5% - 9.7% for men4. Furthermore, 20% - 27% of the approximately 400,000 women who deliver every year in Zambia5 are estimated to be HIV-positive. Consequently, around 30,000 to 40,000 Zambian infants are thought to contract HIV by vertical transmission every year. Among the foremost reasons cited for the increased vulnerability of women to HIV infection is the higher efficiency of male-to-female HIV transmission than the reverse that has been shown in developed countries6, 7. In addition to this universal reason, many other factors seem to play a role in African countries. The high rate of undiagnosed and untreated STI (sexually transmitted infection)8 and the high frequency of transfusion of contaminated blood during high-risk deliveries under the insufficient safe blood policy9 are increasing the biologic risk of HIV infection among African women. The socioeconomic and cultural conditions faced by women, such as poverty, economic dependence, socio-sexual subordination, and power inequity, are also considered to contribute to their increased vulnerability to HIV infection10,11. Male resistance to condom use and women's inability to negotiate safer sex12 are considered to be major obstacles to the reduction of non-protective sex. The promotion of condom use within marriage might be the most difficult challenge in this society, where child bearing is of great value. However, it should be more targeted, in order to reduce the advancing deadly threat of a generalized HIV epidemic in women and children. Confronted with a very high prevalence of HIV infection among pregnant women in Zambia, we decided to investigate the factors related to women that facilitate condom use to help women protect themselves against contracting HIV infection. Methods The present study was performed at a primary-level health clinic offering antenatal services, located in an urban area of Lusaka city. The clinic covered a population of 120,000 people living in a compound named Chipata, with an estimated 6,400 annual pregnancies. The clinic is one of six antenatal clinics at which the national PMTCT (Prevention of Mother to Child Transmission) programme was conducted between 2000 and 2002, with the support of UNICEF/UNAIDS. The pregnant women on their first attendance at antenatal care were invited to individual pre-test counselling after a brief explanation of the VCT Voluntary Counselling and Testing and PMTCT programme. Our cross-sectional questionnaire survey was given before the start of individual pre-test counselling. Zambian female staff trained for this study interviewed the women individually, using a structured questionnaire. After counselling, the consent of each woman for serologic testing of HIV was sought. Each woman was assigned a serial number in addition to the number on her clinical record sheet. HIV status was checked thereafter using the serial number, and the confidentiality of each individual was strictly respected. The questionnaire included items aimed at defining the women's socioeconomic characteristics (age, recognition of own and husband's HIV sero-status before this VCT, years of school attendance, own earning, condom use) and reproductive profile (number of pregnancies, live births, abortions, and child deaths). The women were also asked which body fluid could transmit HIV among blood, breast milk, semen, and vaginal secretion. As for condom use, respondents were asked how often their husbands and/or their partners used condoms in the past. The term `partner' in this study was defined as sexual partner excluding husband. Each answer was classified into three categories, respectively: never use, sometimes use, and always use. Regarding sexual relationship, we classified the respondents into three groups according to their answers to two questions on condom use: `only husband' for those who answered only the question for condom use with husband, `husband and partner' for those who answered both questions for condom use with husband and with partner, and `only partner' for those who answered only the question for condom use with partner. The group `only husband' indicates, in its broad sense, women with fidelity, and the other group `husband and partner' indicates women who were having extramarital affairs. The sampling was conducted consecutively between November 2000 and May 2001. The HIV sero-status was determined at the laboratory attached to the clinic using an HIV-1&2 rapid test kit (ABBOTT), and confirmed using another test kit (BIONOR or GenieII). The results were announced to the women two days after, and then they received post-test counselling. Ethical approval for the study was obtained from The Zambian Government/University of Zambia Research Ethic Committee. Data analysis Associations between HIV sero-status and socio-economic/reproductive characteristics
were examined by the chi-square test and unpaired Student's t-test. School
attendance was divided into seven categories and subjected to the following
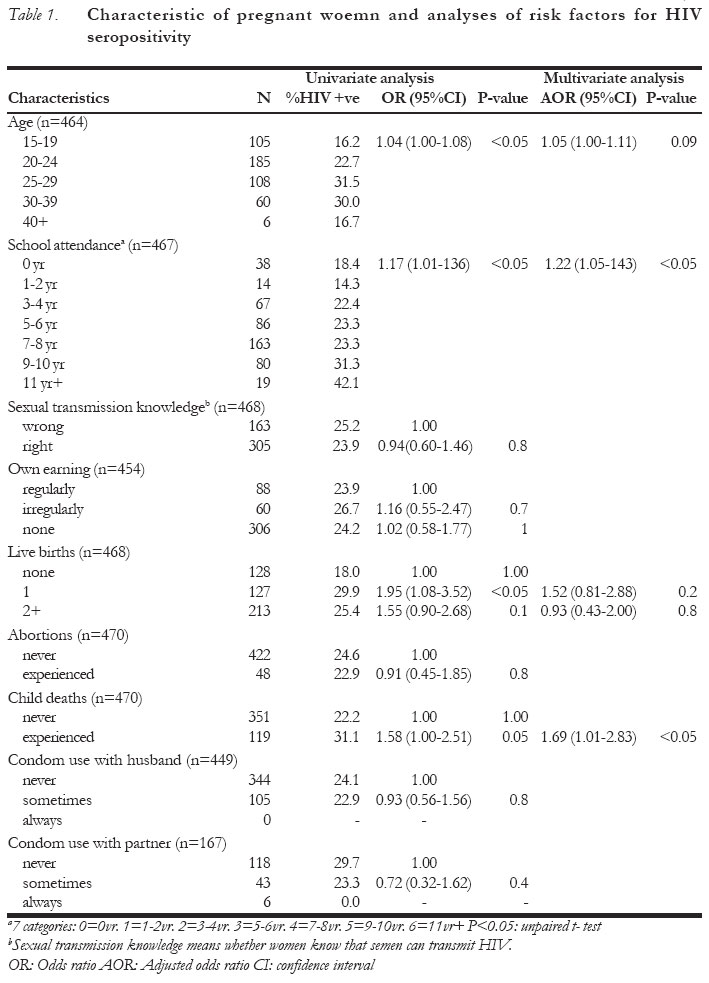
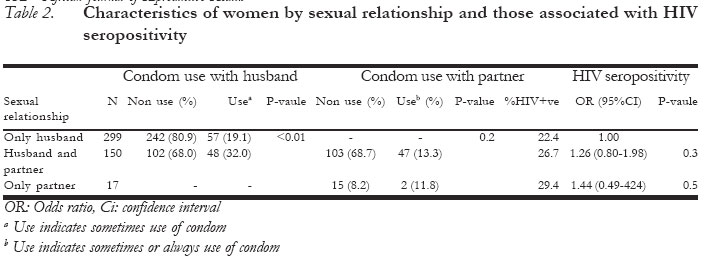
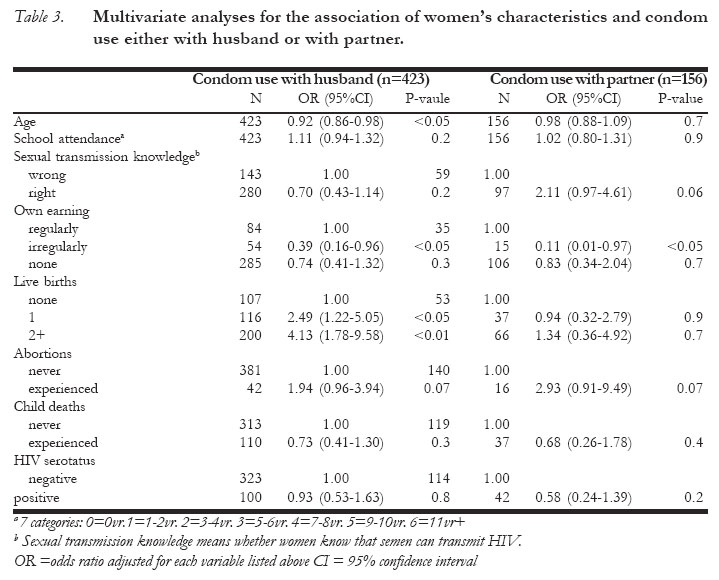
analys Results The general characteristics of the surveyed population, together with HIV seropositivity and its risk factors, are summarized in Table 1. A total of 490 pregnant women agreed to be tested for HIV. The rate of HIV test acceptance was 49.1%. Twenty cases were eliminated due to lack of serologic data (i.e., missing blood sample, one; rapid test declined, two; data not recorded, 17). Consequently, 470 pregnant women aged 15 to 44 were enrolled for analyses. The overall HIV prevalence was 24.5% (95% confidence interval [CI]=20.6-28.4). Only 6.2% were aware of their own HIV status before undergoing HIV testing, including two women who knew of their HIV infection and 27 who knew that they were HIV negative. Similarly, 5.7% of women were aware of their husband's HIV status (data not shown). A feature of age-specific prevalence of HIV infection was a slightly higher rate among women aged 15-19 years than that recorded in the sentinel surveillance study conducted in the same Lusaka city in 1998 (14.8% in 1998, 16.2% in the present study)13. The age of women was associated significantly with HIV seropositivity by univariate, but not by multivariate analysis. The prevalence of HIV infection increased significantly with increase in the years of school attendance by both univariate and multivariate analyses. The rate of correct answers on the routes of HIV transmission were 97.2% for blood, 80.8% for breast milk, 65.2% for semen, and 62.6% for vaginal secretion (data not shown). Thus, a gap existed in the extent of knowledge between the non-sexual (blood or breast milk) and the sexual (semen or vaginal secretion) routes of HIV transmission (P<0.01, chi-square test). Those who answered correctly on the non-sexual routes had a trend toward longer school attendance (blood, P<0.05; breast milk, P=0.09; unpaired t-test). However, no association was found regarding the sexual routes. Furthermore, knowledge of the routes of sexual transmission did not correlate significantly with HIV seronegativity in the present study. One-third of the women had their own earnings, whether or not the earning was regular. As for the factors comprising the reproductive profile, child deaths were associated significantly with HIV seropositivity in the multivariate analysis. None of the women answered that they always use condoms, and only one-fourth reported sometimes use of condoms with their husbands. Condom use both with husband and partner tended to decrease HIV prevalence, but a significant association was not revealed. Table 2 shows the distribution of women by sexual relationship, condom use, and HIV seropositivity in each group. Of the 466 pregnant women, 32% had extramarital sexual relationships. The HIV prevalence among women with fidelity was not significantly lower than that among women without fidelity. With respect to condom use with the husband, it was much lower among the fidelity group than among extramarital affair group (P<0.01, chi-square test). Women involved in extramarital sexual relationships seemed to have increased condom use either with the husband or with the partner. Table 3 shows the results of the multivariate analyses for the association of women's characteristics with condom use either with husband or with partner. Condom use with husband showed a significant association with age and number of live births (for age, odds ratio [OR]=0.92, 95% CI=0.86-0.98); for the number of live births, 1, OR=2.49, 95% CI=1.22-5.05; 2+, OR=4.13, 95% CI=1.78-9.58). On the other hand, condom use with partner was not associated with these factors. Sexual transmission knowledge tended to associate with condom use with the partner but not with the husband. Women with irregular earnings had significantly lower condom use with both husband and partner than those with regular earnings (with husband, OR=0.39, 95% CI=0.16-0.96; with partner, OR=0.11, 95% CI=0.01-0.97). Discussion The present study indicates the tendency of and the factors associated with the HIV epidemic among urban pregnant women in Zambia in 2001. The overall prevalence of HIV infection in the study population was slightly lower than that in the report of sentinel surveillance performed in 1998 (median 27.3%, min. 25.9%, max. 29.1% in antenatal care clinics-major urban areas)13,14. However, it may be noted that the prevalence in women 15-19 years of age was slightly higher than in that report. We observed a contradictory effect of the length of education on the prevention of women contracting HIV infection. This result was not unexpected, since previous reports have found that a woman's educational attainment was linked positively with a high prevalence of HIV infection15,16. School attendance did not, in fact, increase condom use with husband or extramarital sexual partner. Furthermore, school attendance was not effective for these women to gain knowledge on sexual transmission of HIV, although it was effective for knowledge of non-sexual transmission routes, such as blood and breast milk. This suggests to us a lack of effective and consistent education regarding HIV transmission and sexual behaviour, at least within the school system. Actually, we had several cases of infected teenagers who had a correct knowledge of the sexual transmission routes. It may be possible that the knowledge was not gained before a risky event or the knowledge was the result of a risky event that led them to become infected with HIV. This again indicates insufficient or lacking education on HIV and sex both in and out of school, and that educational efforts should be implemented before the very early age of sexual debut among Zambian women17,18. Another reason for non-linkage between sexual transmission knowledge and HIV protection might be the power inequity between men and women, which makes it exceedingly difficult for women even with sexual transmission knowledge to negotiate safer sex with their sexual partners19,20. Concerning whether a woman's fidelity protects her from HIV infection, our result was not affirmative. Among women with fidelity (the "only husband" group), the prevalence of HIV infection was not significantly lower, and condom use was much lower than among women who were having extramarital affairs (the "husband and partner" group). This finding suggests to us that the woman's fidelity only cannot prevent HIV transmission within marriage, given together with the high rate of polygamy in Zambia21. On the other hand, significantly higher use of condoms both with the husband and with other partners among women having extramarital relations, prompts us to consider that the meaning of condom use as an HIV protector is becoming accepted and is put into practice to some extent in Zambia. Interestingly, the factors significantly associated with condom use within and outside of marriage were very different from each other. Reproductive factors, such as the number of live births, promoted condom use with the husband, which is consistent with the previous report22. It would appear that the motivation for condom use comes after a sufficient number of childbirths. In other words, condom use within marriage can be promoted when family planning is more accepted and practiced. On the other hand, for condom use with the extramarital sexual partner, not the reproductive factors but the knowledge of the sexual transmission route of HIV was barely associated, which indicates that sexual transmission knowledge can push condom use as HIV protection in the context of which childbearing is not expected. Besides this, it is noteworthy, in comparison to the inefficacy of school attendance, that regular earning by a woman was significantly associated with condom use with both husband and partner. The possibility of sex work as the source of earnings was thought to be very low, since the percentage of women with fidelity among women with regular earnings was 59% compared with 37% for women without fidelity, and this ratio was similar in both the irregular earnings and no earnings groups (data not shown). Empowering women, or correcting the power imbalance between partners, has received much attention as critical to gaining the male partners' cooperation and acceptance of condom use1,19,23. However, it has not been clearly demonstrated what constitutes a woman's empowerment and how it can be acquired. Our results suggest that even relative but stable economic independence by their own earning, irrespective of their school attendance, might be indispensable, even though education has been believed to be a prerequisite for economic empowerment. It would appear that a woman's economic independence should receive proper attention to combat the spread of HIV infection through condom use. In conclusion, the following should be implemented intensively in the HIV/AIDS prevention programme in Zambia: effective HIV and sex education for young girls less than 15 years of age in and out of school, further implementation of family planning with emphasis on condom use, and empowering women by helping them to become economically independent. Acknowledgements The authors thank the Lusaka PMTCT Health staff for conducting this investigation and the interviews. This research was supported by grants from the Ministry of Education and the Ministry of Health, Labour and Welfare of Japan. References
© Copyright 2005 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh05047t1.jpg] [rh05047t3.jpg] [rh05047t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}