 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 9, No. 3, December, 2005, pp. 148-158 Women's Perceptions of Pain and Discomfort after Childbirth in Angola La perception de la douleur et la gêne chez les femmes après l'accouchement en Angola. Elisabeth Jangsten1,2, Roland Strand3, Engrácia da Glória Gomez de Freitas4, Anna-Lena Hellström2, Annika Johansson3 and Staffan Bergström3 1Department of Obstetrics and Gynaecology, Sahlgrenska University
Hospital, Gothenburg, Sweden. 2Institute of Nursing, The Sahlgrenska
Academy at Göteborg University, Gothenburg, Sweden. 3Division
of International Health (IHCAR), Department of Public Health Sciences, Karolinska
Institutet, Stockholm, Sweden. 4Curso de Espezializacão
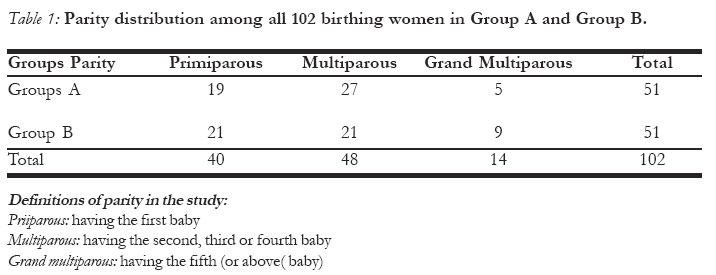
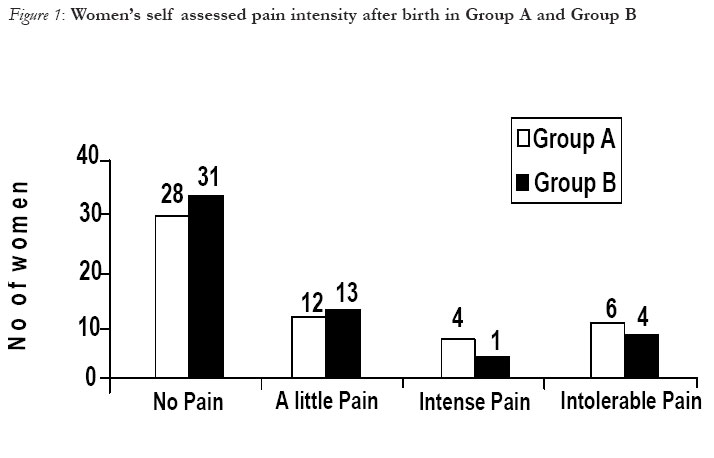
de Parterias, Ministerio de Saúde, Luanda, Angola Correspondence: Elisabeth Jangsten E-mail: elisabeth.jangsten@vgregion. Code Number: rh05049 Abstract Prophylactic treatment against postpartum haemorrhage is a widely investigated area and injection of Oxytocics has been considered as the best choice. The occurrence of postpartum pain and discomfort was studied in a population of birthing women in an overcrowded labour ward in Angola where the oxytocin-filled device Uniject TM was used. This study indicates that birthing women's perceived postpartum pain increases with parity and during breastfeeding, but does not confirm that injection of oxytocin increases pain and discomfort. This is an important finding, since it might facilitate the introduction of a management practice, likely to reduce haemorrhage-related maternal morbidity and mortality after delivery in underprivileged populations. The birthing women were, by and large, satisfied with the care and treatment provided, but the encounters with midwives seem to vary in quality. Further investigation is needed to elucidate parturient women's experience of postpartum pain and their perceptions of the quality of care and treatment. (Afr J Reprod Health 2005; 9[3]:148-158) Résumé Le traitement prophylactique contre l'hémorragie est un domaine qui a été bien étudié et l'injection des oxytoxiques est considérée comme la meilleure option. La survenue de la douleur et de la gêne postpartum à été étudiée chez une population de femmes en train d'accoucher dans une sale d'accouchement en Angola où un instrument plein d'oxytocine, UnijectTM, a été utilisé. L'étude montre que la douleur postpartum perçue chez les femmes en train d'accoucher augmente avec la parité et pendant l'allaitement, mais ne confirme pas que l'injection de l'oxytocine augmente la douleur et la gêne. Ce résultat est important puisqu'il peut faciliter l'introduction d'une pratique de suivi qui probablement réduira la mortalité et la morbidité maternelles liées à l'hémorragie après l'accouchement auprès des populations démunies. Les femmes en train d'accoucher étaient plus ou moins satisfaites des soins et des traitements offerts, mais leurs expériences auprè des sages-femmes semblaient varier en qualité. Il faut advantage études pour élucider l'expérience de la douleur postpartum chez les femmes parturientes ainsi que leur perceptions de la qualité de soin et de traitement. (Rev Afr Santé Reprod 2005; 9[3]:148-158) Key Words: Postpartum haemorrhage, third stage of labour, labour pain, satisfaction with care Introduction Among complications during pregnancy and childbirth, postpartum haemorrhage (PPH) is the single most important cause of maternal mortality1. PPH is defined as `blood loss of ³ 500 ml during the first 24 hours postpartum'. This level is arbitrary and for some women even less can be life threatening, particularly among those who suffer from severe anaemia. The prevalence of PPH is between 10 and 20% of all deliveries and the most common cause is uterine atony 2, 3. Several studies have shown that active management during the third stage of labour, AML, especially administration of uterotonic drugs, reduces the incidence of PPH by up to 40% 1,4,5. The steps in AML are in the following order: (1) early cord clamping, (2) injection of oxytocin, (3) traction of the umbilical cord during expulsion of the placenta6. WHO recommends that AML should be actively promoted in low-income countries where anaemia is widespread and treatment of blood loss may imply significant problems7. However, some women complain about oxytocin-induced postpartum pain, so-called "after pains". Hitherto there have been no studies on the acceptability of oxytocin injection for birthing women, or of the degree of pain caused by the injection as perceived by the women. The International Association for the Study of Pain defines pain as "an individual sensorial and emotional experience correlated with actual or potential tissue damage, or describes it in terms of damage"8. The word "pain" is from the Latin "poena", which means "punishment". Labour pain has always been considered a normal phenomenon, though a unique pain experience, because it is intense and expected. Many women describe it as the most severe pain they have experienced. Pain during this circumstance is an important signal indicating that labour has started and the perception of pain increases as labour progresses8. Several variables correlate with labour pain. The major determinant of labour pain is parity, primiparous women having more pain than multiparous women 9. One of the most important tasks for a midwife, except providing obstetric care, is to support women during pregnancy and childbirth. It has been demonstrated that empathetic and physical support during labour has many benefits, including shorter labour and less medication. It also reduces anxiety and helps mothers to cope with labour pain and thus improves the childbirth experience6. The literature describes different methods to assess labour pain. The visual analogue scale (VAS) is the most frequently used self-assessment scale of pain intensity. It is a plastic instrument that can easily be held in the hand, utilising a line from zero to ten with a moveable marker, where zero means no pain and ten means intolerable pain. The woman assesses her pain and puts the mark on the line8. Another method is the McGill Pain Questionnaire, which is a long list of words intended to describe the pain, and implies a multidimensional assessment 9. It provides three types of measurements: pain-rating index, number of words chosen to express pain, and assessment of pain intensity. The Pain-O-Meter, POM, is partly based on a simplified version of the McGill Pain Questionnaire and VAS developed for clinical use10. On one side there are descriptive words (e.g., cutting, burning, aching, fearful, torturing, and horrible). Each word has a ranking value unknown to the patient. The Pain-O-Meter provides an assessment of the sensory and affective dimensions of pain experience. The verbal rating scale, VRS, is another self-assessment scale, including 3 to 5 expressions such as weak, medium or strong. The advantage of these scales is that they are easy to use and give immediate information8. While pain during the first and second stage of labour is given extensive scientific atten- tion,8, 9, 11 this is not the case for postpartum pain. This was demonstrated in a study in England of 100 primiparous and 100 multiparous women, who were interviewed after 48 hours. Fifty of the primiparous and 86 of the multiparous women complained of lower abdominal pain during the third stage of labour12. The study did not explore what kind of management was used during the third stage of labour. Angola has been ravaged by a civil war for more than 40 years, causing extreme hardship for the population. Less than one-third of the population has access to health services and one of three children dies before the age of five. Life expectancy is 42 years and 70% of the women are illiterate. The institutional maternal mortality ratio, MMR, in 2003 in the national capital, Luanda, was 1,320 per 100,000 live births. Postpartum haemorrhage is one of the main causes of death, making it important to reduce critical blood loss during the third stage of labour 13. UnijectTM is a disposable injection device consisting of a pre-filled, plastic tube with 10 IU of oxytocin and a sterile needle attached for intramuscular injection. It has been tested in third-stage labour in Indonesia, where midwives preferred it to the standard use of needles and syringes14. In 1999 WHO initiated the UnijectTM project at Maternidade Lucrécia Paím (MLP) in Luanda, in collaboration with the Division of International Health (IHCAR) Karolinska Institutet in Stockholm. The UnijectTM project studied the postpartum blood loss before and after introduction of AML with UnijectTM and a drastic reduction of blood loss was demonstrated after the introduction of this method15. The purpose of this study was to investigate the perceptions of pain and discomfort among birthing women in Angola in connection with the use of UnijectTM given as a part of AML, compared to women not receiving the treatment. Materials and methods Of a total population of around 13 million in Angola, approximately one-third lives in Luanda. Health statistics are scarce and unreliable, but it is estimated that 100,000-125,000 deliveries occur per year in Luanda, assuming a crude birth rate of 40-50 per thousand13. Approximately 50% of all births take place at maternity wards or peripheral birth clinics. MLP is the largest maternity hospital in Luanda and is also a referral hospital. In 1998 nearly 100,000 women sought for care and treatment and 16,000-17,000 deliveries occur yearly. About 20% of maternal mortality at MLP is due to PPH13. The obstetric care unit staff consists of four to five midwives per shift and during one day midwives may assist 40-50 deliveries. The wards are crowded and the number of beds are insufficient. A woman in labour often has to share a bed with another woman and there is almost no privacy. Family members are not permitted to support a woman during labour at the maternity unit. During visiting hours families are allowed to bring food to birthing women. In case of an emergency, where blood transfusion is necessary, there is often insufficient blood available. Staff members have to call the family, which must then arrange a blood donor and buy the necessary equipment for blood transfusion. For the UnijectTM project, 12 midwives and 4 doctors were trained and defined as the project staff. At the obstetric care unit birthing women were included in the study by the project staff when they arrived at the maternity in labour between 08 am - 02 pm. The high workload did not permit all women to be included in the project. Women not included were treated routinely, which means that no treatment was given during the third stage of labour. All women were transferred after two hours to the post-natal ward to stay for a period between 6 and 24 hours and it was during this period that this study was carried out. A semi-structured questionnaire was developed and translated into Portuguese. The verbal rating scale (VRS) was chosen as the best alternative in this study setting and a four-grade scale about pain was used to distinguish "no pain", "a little pain", "intense pain", and "intolerable pain". It also included questions about the localisation of pain, breastfeeding, satisfaction of care and empathy shown to the women by staff. The questions about satisfaction with care and degree of empathy were divided into "good", "average", and "bad". The last question was open-ended and labelled "own comments". Information about age, gestation, parity, birth weight, time of birth and time of expulsion of the placenta was retrieved from the patients´ records. The women's comments in the open-ended question are described in themes by quotations according to the contents16. It was not possible for the women to fill in the questionnaire by themselves because of the significant proportion of illiterate women, some of whom did not understand Portuguese. One of the authors (EGGF), having both cultural and professional competence, served as an inter-viewer. She did not wear a uniform, she was unknown by the mothers and they were not dependent on her as a care provider. It was not possible to do the interviews within the same time after delivery for all of the women. Some women had given birth early in the morning and some had just recently arrived to the post-natal ward. The sampling of parturients was carried out during two weeks at the post-natal ward. Women were included in Group A if they were treated with AML and UnijectTM, or Group B if they were treated according to the routine at the obstetric care unit. The interviewer received information about whom she was going to interview when she arrived at the post-natal ward. She was not informed whether the parturients belonged to Group A or Group B. The interviews were performed in the afternoons 2-12 hours after the delivery and lasted for about 10 minutes per woman. The data were analysed from the two groups of women expressing postpartum pain and compared by use of the chi-square test with Yates´ correction17. Permission was obtained from the ethical committee at Karolinska Institute, Stockholm, Sweden and from the Agostinho Neto University, Luanda, Angola. Findings Informed verbal consent was received from all women who participated in the study. One hundred and two women were included and interviewed, of whom 51 belonged to group A and 51 belonged to group B. In group B, there is one record with no data about parity. There are also data missing about intensity of pain for one woman and about breastfeeding for another, both in group A. The average age was 24 years in group A and 23 years in group B. The parity distributions are presented in Table 1. A majority of the birthing women had been visiting antenatal clinics. Twenty-nine of the women in group A had a calculated gestational age according to the first day of last menstrual period. In group B, there were 27 women who had a calculated gestational age. Among these women, there were five pre-term deliveries and three post-term deliveries in Group A, and in Group B there were four pre-term deliveries and three post-term deliveries. None of the multiparous or grand multi-parous women had a previous caesarean section or instrumental delivery. In Group A, there were 9 mothers (18%) who had lost one child and 3 mothers had lost 2 children. In Group, B 8 mothers (16%) had lost one child, 3 mothers who had lost 2 children, one mother had lost 3 children and one had lost 5 children. Seventy-five percent of the birthing women in both groups arrived at the maternity unit with a dilatation of the cervix between 6 and 10 cm and they delivered between 5 minutes and 3 hours after being admitted. The mean birth weight in group A was 3,100 g and in group B 3,200g. Expression of pain was assessed in two ways that tried to take into consideration the social and cultural dimensions of the women approached. The quantifying of pain is expressed in Figures 1 and 2 and examples of the individual pain expressions are presented in quotations. Postpartum pain was experienced by 45% of the women in group A, of that percentage 10 women said that they felt intense or intolerable pain. In group B, 37 % felt pain after delivery and 5 women classified the pain as intense or intolerable pain (Figure 1). However, a chi-square test did not confirm a significant difference between the two groups (p=0.55). Multiparous women experienced more postpartum pain than primiparous women, irrespective of whether they had received any treatment during third stage of labour. Among 40 primiparous women, only 6 experienced pain after delivery. Multiparous and grand multiparous women totalled 62 and among them 36 women experienced postpartum pain. The difference is statistically significant (p=0.002). The pain ranking value was also assessed higher among the multiparous and grand multiparous women. In both groups, there were 15 women who ranked the pain as intense or intolerable and only two of them were primi- parous women. The pain was mostly described by the parturients in both groups as localised in the lower abdomen (90%). Other localisations of pain were also described, such as lower back pain, upper back pain and epigastric pain. Multiparous women who belonged to group A explained their pain and discomfort with the following words:
The multiparous women from group B describe pain in these sentences:
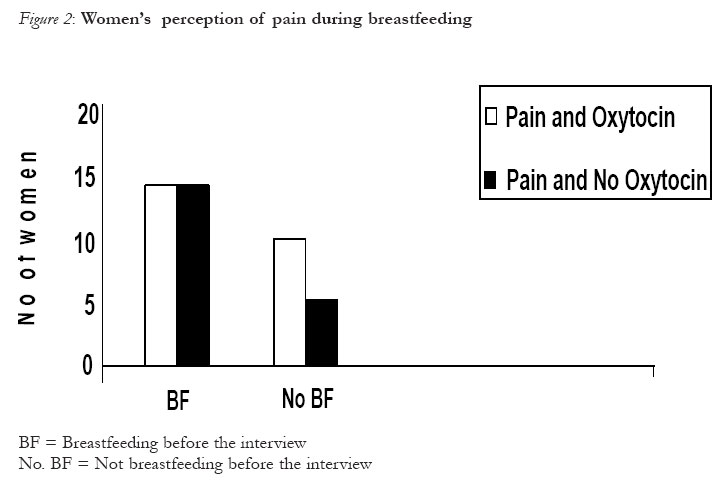
An analysis was made to see if time and memory could be a factor influencing the women's answers regarding intensity of pain. Most women were interviewed in the post-natal ward 4 to 8 hours after delivery. Approximately 20% of the women were interviewed between 2 and 4 hours after delivery and 9% were interviewed 8-12 hours after delivery. Thus the timefactor is not likely to have influenced the results in any significant way. We also found that breastfeeding mothers in both groups had similar degrees of postpartum pain (Figure 2). Altogether were 61 breastfeeding mothers and 40 mothers who had not breastfed their new-borns before the interview. Breastfeeding mothers had more pain after delivery than non-breastfeeding mothers by the time they were interviewed. Twenty-two mothers in group A complained of pain and 14 of them had breastfed. In Group B, 18 mothers experienced pain and 14 of them had breastfed. Only one primiparous woman from each group experienced intense or intolerable pain during breastfeeding. Comments from the birthing women indicate that breastfeeding exacerbates postpartum pain. The comments about breastfeeding and pain are all from multiparous and grand multiparous women:
Most of the women (75%) were satisfied with the care they received at the maternity ward. In both Groups A and B, 38 women expressed full satisfaction, while 10 women in Group A and 11 women in Group B was reasonable satisfied. Three women in Group A and two in Group B were not satisfied. On the question about empathy the result was similar. Thirty-two women in both groups found that the care providers' empathy was good, 13 women in Group A and 12 in Group B had the opinion that it was reasonable. Six women in Group A and 7 in Group B thought that the care providers' empathy was poor. The last question was an open question, labelled "own comments". More than half, 57 of 102 women made comments in response to this. The comments mostly concerned women's postpartum pain and their perceptions of care and treatment. The comments are divided into five themes according to the content and described by quotations. The following themes were discussed: (1) pain and discomfort, (2) breastfeeding, (3) satisfaction with care, (4) behaviour, and (5) economy. In Group A, 28 women gave their comments and in the Group B, 29 women did so. The comments were similar in both groups and included not only satisfaction, but also dissatisfaction with the care. It also elucidated the encounter with care providers. One woman from Group A seemed to be satisfied with the treatment and expressed it in these words:
A woman from Group B seemed to be pleased with the treatment by the care provider. ("Attention" could mean that she felt supported):
The next sentence describes that "good behaviour" is favourable and screaming is equated with scandalous behaviour and is punished by the care providers, expressed in these words:
Several comments were about the behaviour of the health staff:
The following describes a perception of reasons for bad treatment from care providers:
Some of the comments include advice to midwives about how to support and treat labouring women. One primiparous woman from Group A said:
A grand multiparous woman said:
Some of the comments indicate that economic conditions can play a role for the perception of care:
Discussion The principal finding in this study is that women receiving oxytocin in the third stage of labour by use of a disposable injection device did not report significantly more pain than women without administration of oxytocin. Hence, the introduction of AML, with the approach utilised, would presumably be acceptable in this population. Its advantages in terms of drastically reduced blood loss postpartum in the same population have already been demonstrated 15 and it can be extrapolated that haemorrhage-related maternal morbidity and mortality were significantly reduce by the introduction of AML in this population. The results in our study showed that women's postpartum pain tends to increase with parity and may not always be correlated with the administration of oxytocin. We also found that breastfeeding tended to exacerbate postpartum pain and that increased postpartum pain can influence the mothers to avoid breastfeeding immediately after birth. A study in England demonstrated that perceived pain during breastfeeding increases with parity due to stronger contractions 18. Pain is a multidimensional experience with physiological, psychological and social components, and the pain of childbirth is rated as one of the most intense of all pains, but it is also extremely variable 11. Birthing women's perception of pain and pain tolerance is influenced by various factors: the individual's previous experience, anxiety, cultural standards and education, etc. It was demonstrated in Israel that women with low educational levels, had higher ratings of pain during labour, assessed by a visual analogue scale (VAS), than highly educated women 19. It became obvious to the authors that both the simple recording of quantified pain and the qualitative approach utilised in the presentation of individual pain reactions are not easily translated in clear categories of responses. The social and cultural dimensions of the reality in which the studied women lived make interpretation of their reactions difficult. In the capital province of Luanda (still severely affected by the ongoing war at the time of the study), the extreme resource scarcity and the lack of security in combination with fear of and experience of rude staff behaviour certainly influenced both the perception and the expression of pain. Given all these negative circumstances, it appears that the introduction of yet another intervention (Uniject TM injection) might be expected to have aggravated the perception of pain still more. This did not appear to have been the case. The accuracy of memory and recalling labour pain is widely discussed. The literature is relatively limited and many studies demonstrate methodological problems. It is shown that women do not completely forget labour pain and recall is often vivid, but not always entirely accurate 11. In a study performed in Sweden, it was shown that the amount of pain and discomfort remembered was less than the amount of pain reported in labour by both primiparous and multiparous women 20. Another study in Israel did not find differences between labour pains recorded immediately after delivery and recalled 2 days after 21. Postpartum pain has not been a focus of investigations, probably because it is less severe than the pain in first and second stages of labour. The method of Verbal Rating Scale (VRS) was considered appropriate when asking the mothers to assess their pain in this study setting. Studies about birthing women's postpartum pain had never been conducted before at the maternity unit used in the present study. The results demonstrate that the mothers had pain by the time when they were interviewed, but not immediately after birth; this can be explained by the fact that they were happy and relieved when the delivery had been uneventful. We found that about 75 % of the parturients in both groups were satisfied with the care and treatment they received and they were also pleased with the empathy shown by the midwives. This result might reflect that the women felt inhibited in expressing their opinions to an interviewer, instead of filling in a questionnaire on their own. Surveys of patient satisfaction as a measure of health-care are important and should be used systematically; it can facilitate choice between alternatives in organising and providing health- care 22. Client satisfaction can be considered an integral component of perceived service quality. Support for this statement has been found in studies indicating that satisfied patients are more likely to continue using medical services. However, reliable information may not always be easy to collect and, for example, dependence on the provider may mute criticism of the service 23. The respondent’s “own comments” enabled us to obtain opinions about the care received. It was obvious that this open question gave the women an opportunity to express their experiences and perceptions. Although the result of satisfaction and empathy gave positive assessment scores, many “own comments” gives another picture about care providers´ treatment. These comments also offer insight for care providers and decision-makers. There are studies that confirm the lack of communication between care providers and labouring women in overcrowded labour wards. During one study in Zambia, it was observed that communication during labour between the midwife and the labouring women was limited. The women were often left alone and had to call for the midwife when it was time to deliver 24. In a study in Rakai district in Uganda, it was demonstrated that only 32 % of the women chose public health units for delivery. Midwives were described as rude, proud, negligent and vulgar. They often tell mothers in labour demeaning words like “Do not disturb us!”, “ Who told you to become pregnant?” 25. In the perception of a positive delivery, the birthing women's encounter with the midwife plays a crucial role. In a Swedish study, women explained that being seen as individuals and receiving respect from the midwives gave them courage, and they did not have to be ashamed of their behaviour. They felt accepted and supported by the midwife, which gave them a positive experience and satisfaction 26. Birthing women with good support are also likely to have more tolerance of pain and need less pain alleviation 27. In many low-income countries, the healthcare and staff's situation in labour wards is difficult because of work overload, low salaries and job dissatisfaction. It is important to be aware of the environment and the study setting. Scarcity of material, equipment and medicine is frustrating. Conclusion AML with administration of 10 IU of oxytocin did not significantly add to the burden of postpartum pain in the population studied. This is an important finding, since it might facilitate the introduction of a management proven to reduce haemorrhage-related maternal morbidity and mortality after delivery in this underprivileged population. Taking into account that many women experience a great deal of pain not only during labour, but also after delivery, further investigations are required with the aim of strengthening midwives ‘consciousness of mothers’ need for support and pain alleviation after delivery and during breastfeeding. Acknowledgements This study was made possible through financial support from the World Health Organization, Family and Reproductive Health, Geneva. We gratefully acknowledge the Management board at Maternidade Lucrécia Paím. The Angolan women are acknowledged for sharing their experiences and perceptions when giving birth at Maternidade Lucrécia Paím. REFERENCES
© Copyright 2005 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh05049t1.jpg] [rh05049f1.jpg] [rh05049f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}