 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
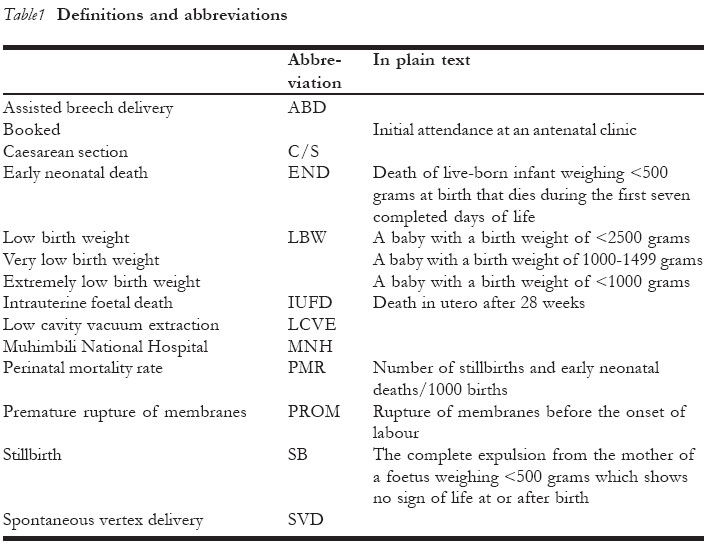
African Journal of Reproductive Health, Vol. 10, No. 2, August, 2006, pp. 72-80 Analysis of Perinatal mortality at a teaching hospital in Dar es Salaam, Tanzania, 1999-2003 Hussein L Kidanto1, Siriel N Massawe1 , Lennarth Nystrom2, Gunilla Lindmark3 Address for correspondence: Hussein L. Kidanto, PO Box 65439, Dar es Salaam, Tanzania. Tel: +255 22 748462478 Email: hkidanto@muchs.ac.tz 1.Department of Obstetrics and Gynaecology, Muhimbili National Hospital, Dar es Salaam, Tanzania Code Number: rh06028 Abstract We conducted a retrospective analysis of perinatal mortality at Muhimbili National Hospital (MNH), Dar es Salaam, Tanzania 1999-2003 in order to categorise/classify perinatal deaths as well as to identify key factors in perinatal care that could be improved. Key Words: Perinatal mortality, Tanzania, low-birth weight, stillbirth, and neonatal deaths
Résumé Mortalité périnatale dans un Centre Hospitalier Universitaire à Dar-Es-Salam, Tanzanie (1999 - 2003). Nous avons mené une analyse retrospective de la mortalité périnatale dans l'Hôpital National de Muhimbi (HNM) à Dar Es Salam, Tanzanie (1999 - 2003) afin de catégoriser/classifier les décès périnatals ainsi que pour identifier les facteurs clé dans le soin périnatal qui peuvent être améliorés. Nous avons collecté les données à partir de base de données obstétriques de HNM et causes du décès précose néonatal ont été tracés à partir de registre de la salle d'hôpital néonatal. L'étude comprenait tous les foetus qui pesaient = 500kg. Une classification des décès périnatals a été réalisé à l'aide d'une Nordic Baltic modifié. Au cours d'une période de cinq ans 77,815 enfants ont été nés avec un taux de mortalité périnatale de 124 pour 1000 naissances dont 78% étaient des naissances mortes liées au travail. Le TMP était 913/1000 pour les accouchements simples et 723/1000 pour les accouchements multiples pour les bébés qui pesaient moins de 1500 grammes et 65/1000 pour les accouchements simples et 116/1000 pour les accouchements multiples pour les bébés qui pesaient 2,500 grammes ou plus. Les bébés qui pesaient moins de 1500 grammes ont contribué 26% du TMP alors que 41% se sont produits chez les bébés qui pesaient 2500 grammes ou plus. La majorité (79%) des décès néonatals avaient l'indice d'Apgar < 7 à 5 minutes et les causes les plus communes de la mortalité néonatale étaient les mort apparante du nouveau - né (37%) et la prématurité (29%). Les décès liés au travail étaient plus communs dans les grossesses multiples. La majorité des décès périnatals doivent être essentiellement évitables grâce à une qualité améliorée de soin intrapartum. L'établissement d'un audit périnatal à HNM pourra aider à identifier le actions clé pour les soins améliorés. (Rev Afr Santé Reprod 2006; 10[2]:72-80) Introduction The perinatal mortality rate (PMR) is not only related to maternal health status but also a sensitive indicator of quality of maternal and neonatal health-care.1,2 PMR in developing countries is more than 10 times higher than in developed countries. The proportion of potentially avoidable perinatal deaths is also higher in resource poor countries with higher PMR and it is likely that a significant reduction can be achieved by minor improvements in the organisation and quality of health care.3,4 Mortality rates among under-5-year-old children have decreased substantially over the past 20 years in developing countries, but PMR has not followed the same trend and continues to represent a huge burden.5 In 1995, WHO estimated the number of perinatal deaths worldwide to be greater than 7.6 million, with 98% of these deaths occurring in developing countries.6 The highest levels of PMR are reported from sub-Saharan Africa (about 80 per 1000 births). Tanzania, like other countries in the region has a high PMR ranging from 90 to100 per 1000 births.7-10 Since 1999 routine data on perinatal outcome are recorded at Muhimbili National Hospital (MNH), Dar es Salaam. Perinatal morbidity and mortality statistics, despite their inherent limitations, provide an important base for audit.10,11 Analysis and monitoring of data collected on a regular basis in audit meetings avails both the neonatal and obstetric staff the opportunity to examine and critically evaluate patient management and to take appropriate action wherever possible.12 At a higher level, such data help to shape policy and change resource allocation. At MNH regular maternal and perinatal audit meetings are held since 2005, whereby data analysed from the data base are the basis for the discussion. We have analysed the perinatal mortality in MNH to document the magnitude of the problem and the relative contribution to perinatal mortality of major factors such as birth weight and labour complications in order to identify areas of perinatal care that merit priority for resource allocation and improved provision of care. Subsequent papers will report on the experiences with the clinical audit.
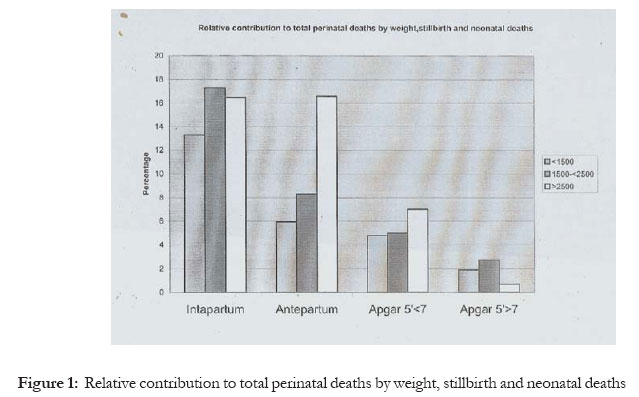
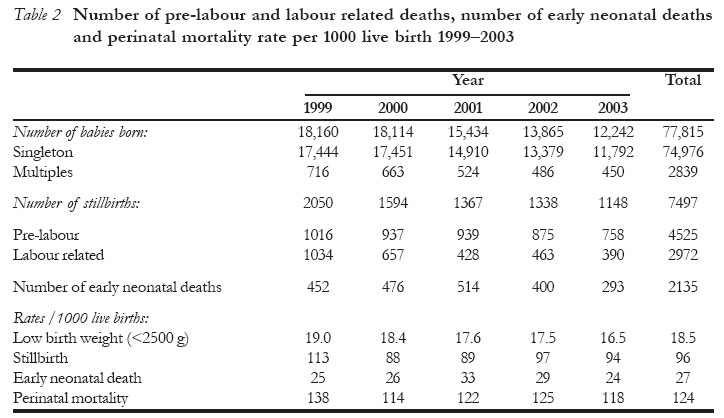
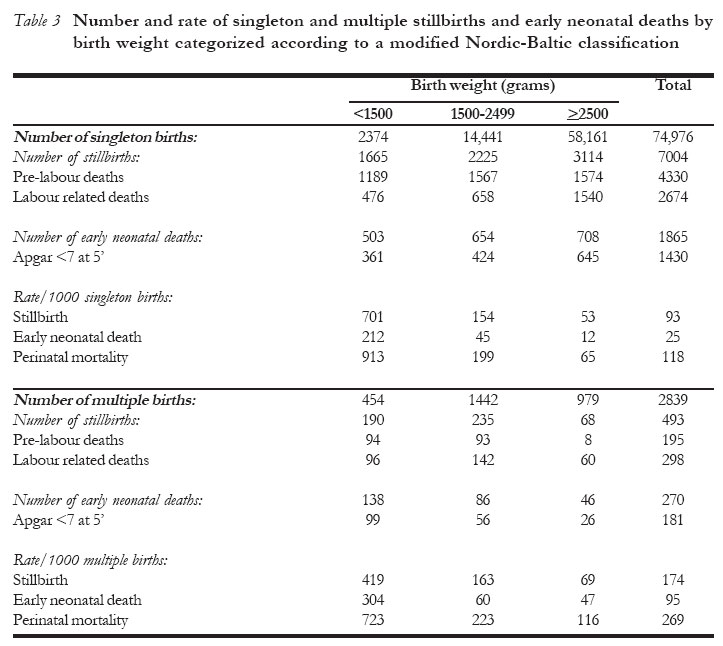
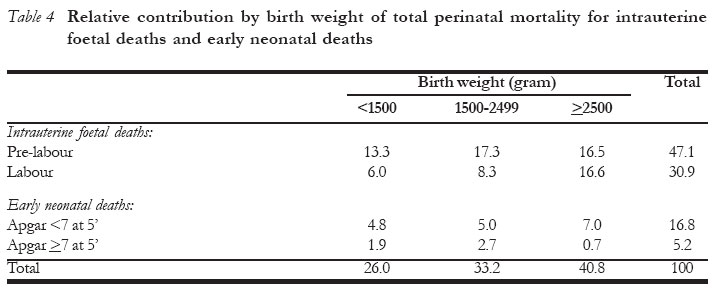
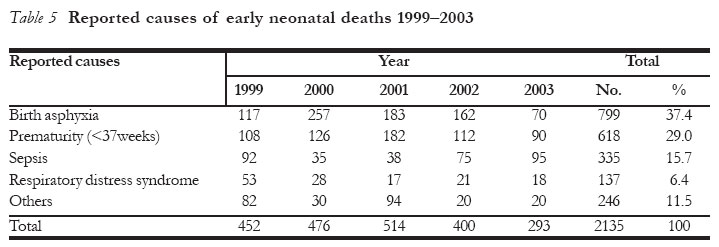
Methods The study was conducted at Muhimbili National Hospital (MNH), Dar es Salaam, Tanzania, a tertiary care hospital. The hospital provides primary and secondary care mainly for Dar es Salaam and the coastal region, but occasionally receives patients from upcountry. In addition, it serves as a referral centre for surrounding districts and primary health-care clinics and as a teaching hospital for the Muhimbili University College of Health Sciences of the University of Dar es Salaam. The MNH labour ward is meant for high risk and complicated deliveries, however, due to poor function of the referral system, 80% of patients come directly from home and often have an essentially normal pregnancy. This leads to overcrowding, an imbalanced staff patient ratio, especially the midwives and overuse, of the scarce supplies available. There are three shifts for nurses, each with six midwives. One specialist obstetrician, one consultant obstetrician and one resident (house officer) are on call every day. There is only one obstetric theatre for both emergency and elective surgeries, so there is often waiting time even for emergencies. The caesarean section (C/S) rate has increased from 12% in 1999 to 29% in 2003, while only 2% of deliveries are vacuum extraction. After a normal uneventful vaginal delivery patients are often only observed in hospital for 6-10 hours before being discharged. Babies delivered by C/S and those with low Apgar score (<7) are admitted to the neonatal ward, which is just one floor up from the labour ward. The unit also admits sick babies from other hospitals as well. The MNH obstetric database was established in 1998 and since that time data have been prospectively entered. The main source of data is the midwifery book in the labour ward. All patients admitted to the MNH labour ward bring their antenatal cards. Information from the cards is transferred to the midwifery book. Delivery data on the progress of labour, maternal and neonatal outcome are also recorded. Causes of early neonatal deaths were traced from the neonatal unit records based on clinical diagnosis. The neonatal register keeps summaries of the case notes of each neonate. A quality check program is run weekly to ensure the quality of the data. Maternal and neonatal diagnosis is based on doctor's records in the case notes. Data for this paper were retrieved from the MNH obstetric database 1999-2003 and counterchecked in the neonatal ward admission register. Neonatal deaths reflect only babies born at MNH and admitted to the neonatal unit. Deaths that occurred at home after discharge from the hospital could not be included. All perinatal deaths among women delivered at MNH labour ward between January 1999 and December 2003 were included. The analysis included all foetuses weighing =500g and deaths of live born infants occurring in the first week in the hospital. Various methods of classifying perinatal deaths have been suggested, however, in this study a modified Nordic-Baltic classification12 has been applied for simplicity. Since it was difficult to ascertain the gestational age, birth weights were used instead. Congenital malformations could not be classified since they were not properly recorded. Thus the variables used for classification were time of death (pre-labour-, labour- or post- delivery), Apgar score at 5 minutes, singleton or multiple gestation, and birth weight. Statistical methods The software Epi Info and PEPI were used for data entry and statistical analysis. Chi-square test was used to test whether there was a trend in low birth weight. The 95% confidence intervals for the rate ratio were based on the Chi-square distribution. Results There were 7497 stillbirths (SB) and 2135 early neonatal deaths (END) making a total of 9632 perinatal deaths among 77,815 babies delivered during the 5-year period. Thus SB, END and perinatal mortality rates were 96, 27 and 124 respectively (Table 2). A large proportion of the intrauterine deaths occurred during labour after arrival to the labour ward. The majority of the neonatal deaths were asphyxiated at delivery. There was a significant decrease in the LBW rate during the study period from 19.0% in 1999 to 16.5% in 2003 (p<0.001), but that was not followed by a similar trend in PMR. The PMR for multiples and singletons were 269 and 118 respectively resulting in a rate ratio of 2.3 (95% CI: 2.1-2.4) (Table 3). The corresponding figures for labour related deaths were 105 and 35.7 respectively resulting in a rate ratio of 2.9 (95% CI: 2.6-3.3). The PMR was 913/1000 for singleton births and 723/1000 for multiple births for babies weighing less than 1500 grams and 65/1000 for singleton births and 116/1000 for multiple births for babies weighing 2500 grams or more. About 41% of all perinatal deaths weighed 2500 grams or more with almost equal numbers of pre-labour and labour-related intrauterine deaths (Table 4). The majority (1611/2135) of the neonatal deaths had Apgar score <7 at 5 minutes. Among the multiple births there were 60 labour-related deaths in babies weighing >2500 grams. There were 1668 breech deliveries during the study period, out of which 485 (28%) and 125 (7.5%) were stillbirths and early neonatal deaths respectively. Breech deliveries were 2.1% of the total deliveries but their relative contribution to the total perinatal mortality was only 6.3% The major causes of neonatal mortality were birth asphyxia (37%), preterm deliveries (29%), sepsis (16%) and respiratory distress syndrome (6.4%) (Table 5). Discussion The motive for this study was to identify areas of priority for improved quality of care in the largest and tertiary delivery ward in Tanzania with extremely high perinatal mortality. We used a modified Nordic Baltic classification12,13 to classify perinatal mortality as according to the relative contribution from different birth weight categories and the relation to labour and delivery, in order to guide on possible actions to be taken. In most statistics from developing countries not all stillbirths are included in official statistics due to logistical difficulties. In Tanzania only 44% of deliveries occur at health facilities and therefore stillbirths and early neonatal deaths occurring outside the health system are not included in health statistics. Further, some severely asphyxiated babies, especially with very low birth weight or with malformations, are often misclassified as stillbirths, since resuscitation is considered as not meaningful and the babies never leave the labour ward. The high PMR reported here is still an underestimation due to the short observation time for babies without initial problems. Mothers delivered normally are only observed for six to twelve hours before discharge, and thus some early neonatal deaths are missing, however, in term babies without initial problems, only a small part of the neonatal mortality occurs after the first 24 hours. During the study period the number of deliveries at the tertiary hospital declined, due to the upgrading of the delivery facilities at the three district hospitals in Dar es Salaam in 2001 (Mwananyamala, Amana, Temeke). However these hospitals are small, understaffed and do not provide 24 hours theatre services, and therefore most complications are referred to MNH, hence increasing the relative proportion of complicated deliveries. These referrals sometimes are made late and therefore they will not always increase the possibilities to save the baby. The PMR was estimated to be 124 per 1000 births, which is higher than the national average (99 per 1000).8 Some smaller community-based studies have reported lower figures (73/1000).9,10 In this study infants weighing 2500 or more contributed about 41% of the total perinatal deaths with labour related asphyxia accounting for 17% of all perinatal deaths The high risk of labour related perinatal death in multiple pregnancies found in this study raises questions on the competence and skills of delivery care providers to conduct these deliveries. There is also an increased risk of perinatal death in babies born in breech presentation, but 80% of them also were low birth weight, with associated higher mortality. Regular in-service training on the management of multiple as well as breech deliveries, especially among midwives and junior doctors might reduce these labour-related deaths as well as the risk of asphyxia and neonatal death. Birth asphyxia and pre-term delivery were the leading cause of neonatal deaths. To meet the millennium goal number four that calls for reduction of mortality in children under five by two thirds, a more rapid reduction is required particularly in the risk of early neonatal deaths, the group that has shown the least decline globally.15 Sepsis seemed to contribute less to neonatal mortality in this study, probably due to under recording. Previous studies have indicated high perinatal morbidity and mortality of neonates due to cord sepsis.13,14 This is again a preventable complication related to the standard of delivery care. The low birth weight rate in this material is 18%, and is similar to other countries in the region. Studies in Tanzania have showed a high incidence of LBW (10-16%).16 The mean birth weight in Tanzania is 2978 grams (UNICEF) and is low compared to developed countries (Denmark 3375g and France 3335 g respectively). PMR among LBW babies was extremely high. The high PMR reported in this study concurs with previous studies, which reported a fourfold increase in mortality16. This is partially explained by the inability to take care of very pre-term babies at the MNH neonatal unit. Previous studies done at MNH have indicated that factors significantly associated with increased neonatal morbidity and mortality were prematurity, birth asphyxia, sepsis, respiratory distress syndrome, hypothermia and hypoglycaemia and majority of the deaths (83%) occurred within the first week of life.16. Infections such as syphilis, HIV and chorioamnionitis and malaria have been associated with pre-term deliveries and therefore low birth weight.16-18 These infections may also contribute to pre-labour deaths.19, 20 Muhimbili National Hospital (MNH) is overwhelmed by a large number of patients. It is the only government owned referral hospital in the city. The population of Dar es Salaam is currently over 3 millions, but the health care structure has not changed since when the population was less than 1 million. This has created an imbalance between the numbers of health care providers, resources and patients. Quality of care in such situation is uncertain.21,22 About 80% of patients admitted for delivery at MNH are coming directly from home and most of them have essentially normal deliveries. The referral system must be streamlined, easy and quick. Only patients requiring tertiary level care should be accepted in the tertiary centre. However this can only be achieved if the existing district hospitals (three) are expanded to cater for more patients since they are small and overcrowded as well. Although the limitations of hospital based data for correct assessment of the magnitude of a problem in the general population is known, the absence of nationally collected vital statistics in most developing countries makes a community based survey impracticable. Hence most studies in developing countries are hospital based. Still, for the purpose of improving the quality of care in the health-care sector, subgroup analysis such as this study and further case-based in depth audit is an appropriate and useful method. Conclusions and recommendations A major part of the perinatal deaths should be essentially avoidable through improved quality of intrapartum care in a tertiary hospital such as MNH. Prelabour intrauterine death must be addressed through improved antenatal care, with special attention to common causes in this region such as syphilis and malaria. Establishment of perinatal audit at MNH can help identify key actions for improved care. Case-based audits of perinatal deaths should be a regular event for more detailed recommendations for a positive change. References
© Copyright 2006 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh06028t5.jpg] [rh06028t3.jpg] [rh06028f1.jpg] [rh06028t4.jpg] [rh06028t1.jpg] [rh06028t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}