 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
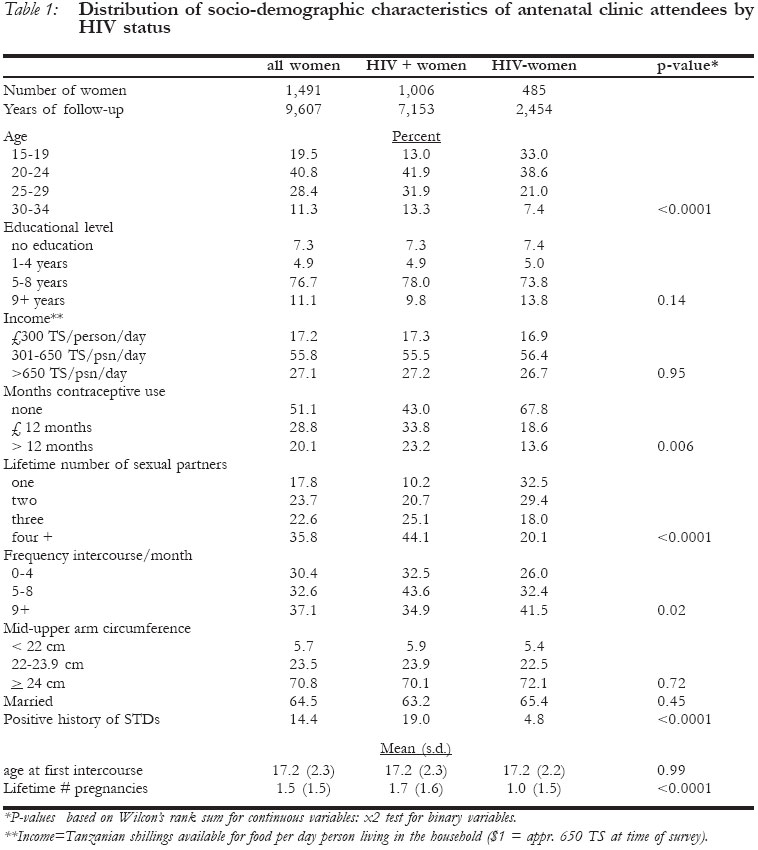
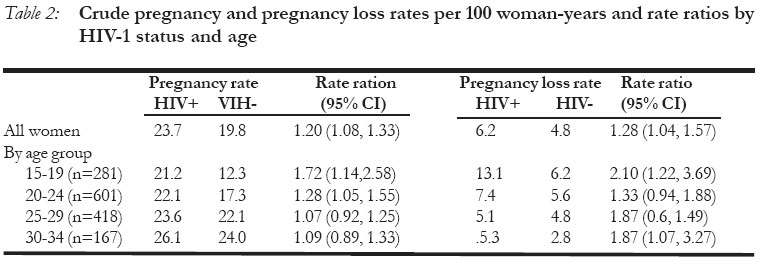
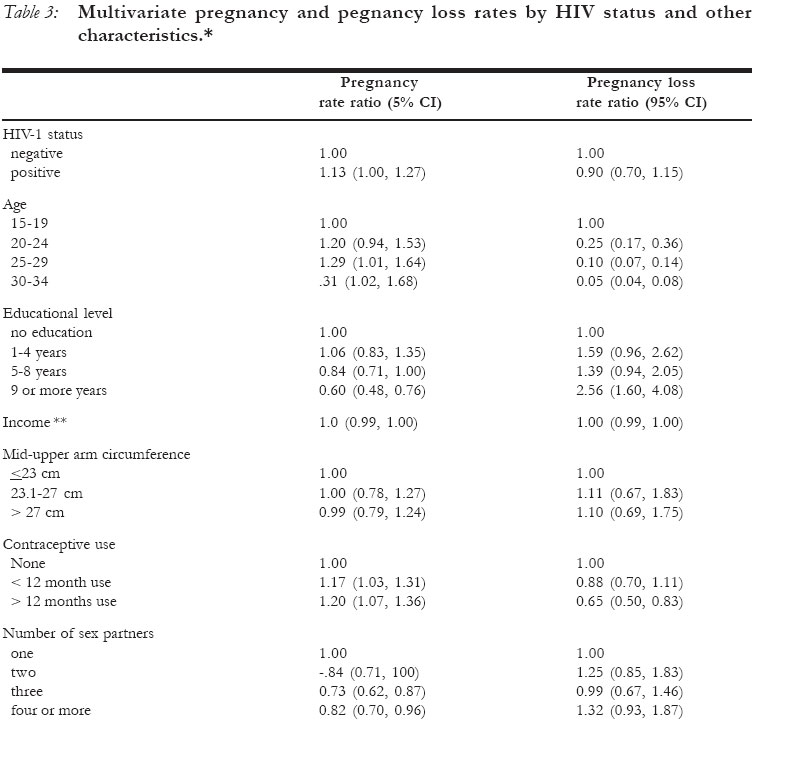
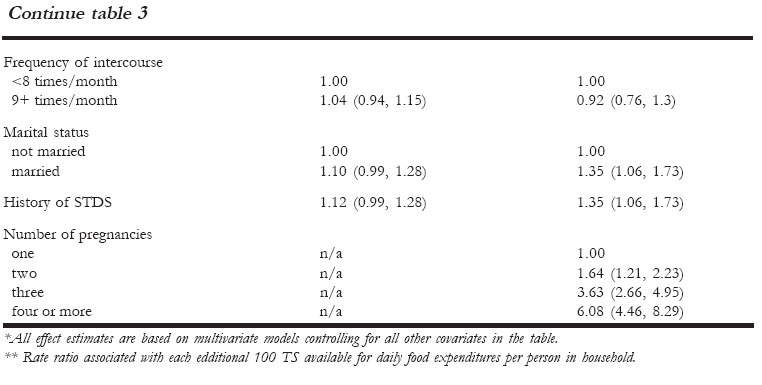
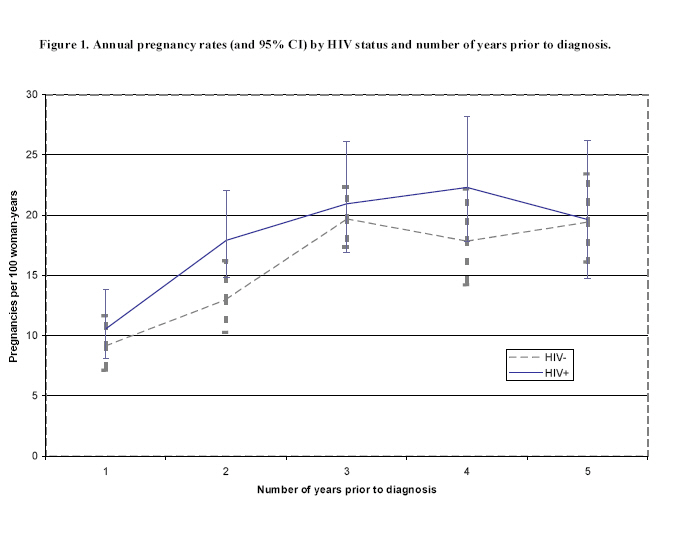
African Journal of Reproductive Health, Vol. 10, No. 3, December, 2006, pp. 41-52 HIV-1 infection and fertility in Dar es Salaam, Tanzania Gilda Sedgh1, Ulla Larsen2, D Spiegelman1,3, Genard Msamanga5, Wafaie W Fawzi1,4 Departments of Epidemiology1, Population and International Health2, Biostatistics3 and Nutrition4, Harvard School of Public Health, Boston MA and the Department of Community Health, Muhimbili University College of Health Sciences, Dar es Salaam, Tanzania5. Correspondence: Gilda Sedgh, Guttmacher Institute, 120 Wall Street, 21st Floor, New York, NY 10005. Tel: 212-248-1111, ext. 2277. Email: gsedgh@guttmacher.org. Code Number: rh06036 Abstract The objective of this study was to examine the association of HIV-1 infection with rates of pregnancy and pregnancy loss in Dar es Salaam, Tanzania. A retrospective cohort study of 1,006 HIV-infected women and 485 uninfected women was employed. In multivariate analyses controlling for other predictors of pregnancy, the association of HIV-seropositivity with a woman's reported number of pregnancies was of borderline significance (RR=1.13, 95% CI=1.00, 1.27). HIV infection was not associated with pregnancy loss in multivariate analysis. The adjusted pregnancy rate ratio comparing HIV-positive women at the earliest stages of infection to all uninfected women was 1.22 (95% CI = 1.04, 1.42). HIV infection was not associated with female fertility when comparing women in the most advanced stages of infection to all uninfected women. We conclude that HIV-1 infected women had higher pregnancy rates than uninfected women. This association disappeared when analyses were limited to women with advanced disease. Abstract word count: 150. (Afr J Reprod Health 2006; 10[3]:41-52) Key Words: HIV-1; pregnancy; pregnancy loss; Africa Résumé Infection du VIH-1 et la fécondité à Dar es Salaam, Tanzanie. Le but de cette étude est d'examiner l'association de l'infection du VIH-1 à la fréquence grossesse et la perte de grossesse à Dar es Salaam, Tanzanie. Une étude cohorte retrospective de 1,006 femmes infectées du VIH-1 et 485 femmes qui l'étaient pas a été menée. Une analyse multifactorielle pour déterminer les indices de grossesse, l'association de la séropositivé _ VIH avec le nombre de grossesses signalées était très peu significative (RR = 1,13, 1,13, 95% CI = 100, 1,27). La séropositivité n'a pas été associée à la perte de grossesse dans l'analyse multifactorielle. La proportion de taux de grossesse si l'on compare les femmes séropositives, tout au debut de l'infection, aux femmes qui ne sont pas atteintes, était 1,22 avec la stérilité chez la femme si l'on compare les femmes non-atteintes. Nous concluons que les femmes séropositives ont des taux de grossesse plus éléves que les femmes non-atteintes. Cette association a disparu quand les analyses ont été limitées aux femmes chez qui la maladie est avancée. (Rev Afr Santé Reprod 2006; 10[3]:41-52) Introduction A causal association between HIV-1 infection and fertility has implications for population fertility patterns and the incidence of orphanhood resulting from the epidemic. Studies have suggested that HIV infection may have a negative impact on fertility1,2,3,4,5 and may be positively associated with the rate of pregnancy loss.6,7 ,8 It is important, however, to ascertain definitively whether these associations exist among asymp-tomatic women who are unaware of their HIV seropositivity, particularly since the prevalence of undiagnosed, pre-clinical HIV infection remains substantial in sub-Saharan Africa. The purpose of this study is to examine the association of HIV-1 infection with rates of pregnancy and pregnancy loss based on reproductive histories in a population of antenatal clinic attendees in Dar es Salaam, Tanzania. Methods The data for these analyses were collected for a randomized trial aimed at studying the effects of vitamin supplementation on HIV-1 disease progression and vertical transmission.9 Recruitment of women took place in antenatal clinics between April 1995 and July 1997. Eligible HIV-1 positive women were pregnant, at 10-27 weeks gestation and residing in Dar es Salaam. Data also were collected from a comparable sample of uninfected pregnant women. The study protocol was approved by the Research and Publications Committee of Muhimbili University College of Health Sciences, the Ethical Committee of the National AIDS Control Program of the Tanzanian Ministry of Health, and the Institutional Review Board of the Harvard School of Public Health. Each woman was asked how many pregnancies, live births, stillbirths and abortions she had ever experienced and the year in which each pregnancy ended. Data also were collected on socio-demographic characteristics and potential determinants of fertility, including age; educational level (number of years of schooling); income (money available for food per person living in household per day, in Tanzanian Shillings); mid-upper arm circumference (used as a marker of general nutritional status); marital status; the duration of her current cohabiting union if applicable; the age at which she first had heterosexual intercourse; the average number of times she had intercourse per month prior to the current pregnancy; her lifetime number of sexual partners; contraceptive methods she has ever used and the number of months she used each method; and whether she had been diagnosed with a sexually transmitted disease in the prior five years. Variables representing the number of months a woman used an effective contraceptive method were based on data on the number of months she used oral contraception, Norplant, an IUD or injectable contraception. The duration of use of each method was weighted by expected levels of user effectiveness, adapted from estimates developed by others.10 We used a retrospective cohort study design and Poisson regression models to examine the association of HIV status with a woman's lifetime number of pregnancies and pregnancy losses. The time at risk of pregnancy and pregnancy loss was defined as the time from each woman's first sexual intercourse until the time of HIV diagnosis. For analyses of predictors of pregnancy loss, we excluded women who had never been pregnant. We examined the association of HIV-1 infection with fertility outcomes in univariate models as well as in models controlling for potential confounding by other predictors of fertility. Women reported the year in which each pregnancy was completed, and this information was used to calculate pregnancy rates for each year prior to HIV diagnosis. These data made it possible to examine whether the association between HIV status and fertility changed over time. For these analyses, a new data set was constructed in which each woman provided multiple observations: one for each year beginning with the year of her first intercourse and ending with the year of diagnosis and data collection. General estimating equations with a Poisson variance and a log link function were employed to take into account the correlation between observations on the same woman.11 We present p-values that are based on an unstructured working correlation matrix and empirical standard error estimates. CD4 cell counts measurements were taken from the HIV-positive women only, and in order to assess whether the association between HIV infection and fertility varied by stage of infection we conducted additional analyses comparing all uninfected women and subsets of infected women defined by CD4 cell counts, using a separate model for each subgroup. It order to explore whether HIV infection may be causally associated with reductions in the level of sexual activity, we examined whether levels of sexual activity decreased with progressing disease, represented by CD4 cell count, in infected women. We used constructed a cross-tabulation of CD4 count and frequency of intercourse and conducted a Mantel-Haenzel chi-square test to examine this association. Data were collected from 1,078 HIV-infected women and 499 HIV-uninfected women. Thirty-eight infected women and 14 uninfected women were excluded from analyses because they were not 15-34 years of age. Thirty-four HIV-positive women were excluded because their pregnancy histories were not available. In all, 1,006 women who were diagnosed with HIV-1 contributed 7,153 person-years of observation from the year of their first sexual intercourse to the date of data collection, and 485 HIV-uninfected women contributed 2,454 person-years of observation. HIV-infected women reported 1,698 pregnancies including 440 pregnancy losses, and uninfected women reported 486 pregnancies and 118 pregnancy losses. Findings HIV-infected and uninfected women were similar with regard to educational level, income, marital status and overall nutritional status (Table 1). The average age of infected women was 24.3 years, versus 22.2 years among uninfected women. HIV-positive women reported a greater lifetime number of sexual partners (4.0 vs. 2.6), slightly more contraceptive use (5.5 months vs. 3.7 months) and a lower frequency of sexual intercourse (8.7 events per month vs. 9.6) compared to HIV-negative women. A larger proportion of infected women had been diagnosed with an STD in the five years prior to HIV diagnosis compared to uninfected women (19.0% vs. 4.8%, respectively). HIV-positive women experienced on average 24 pregnancies per 100 woman-years of observation, while uninfected women experienced 20 pregnancies per 100 woman-years. The crude relative rate of pregnancy comparing infected and uninfected women was 1.20 (95% CI = 1.08, 1.33) (Table 2). The difference between infected and uninfected women was greatest in the 15-19-year old age group (RR=1.72, 95%CI = 1.14, 2.58). There was no significant difference among women aged 25 and older. After adjusting for known determinants of female fertility, including age, marital status, income, educational level, STD history, months of contraceptive use, lifetime number of sexual partners, recent frequency of intercourse and nutritional status, the difference between the two groups was considerably attenuated (RR = 1.13, 95% CI = 1.00, 1.27) (Table 3a, b). The association between HIV status and pregnancy did not vary significantly across strata of any of the factors used in these analyses. The rate of pregnancy loss in infected women who had ever been pregnant was 6.2 per 100 woman-years, compared to 4.8 per 100 woman-years in uninfected women (RR=1.28, 95% CI=1.04, 1.57). After adjusting for determinants of pregnancy loss, the difference between infected and uninfected women again disappeared (RR=0.90, 95% CI= 0.70, 1.15). The association between HIV status and the rate of pregnancy loss was not significantly modified by any of the factors used in the multivariate analysis. Using women's reports of the year in which each pregnancy was completed, annual pregnancy rates were calculated for each year prior to diagnosis. We examined whether the pregnancy rate ratio associated with HIV infection changed over time, starting at five years prior to HIV diagnosis and continuing to the year immediately prior to diagnosis (Figure 1). There was no clear trend in the magnitude or direction of the association over time. It was not possible to estimate the annual rate of pregnancy loss because information was not available on the year of each pregnancy loss. The adjusted pregnancy rate ratio comparing women with CD4 counts of at least 500 cells/mm3 to all uninfected women was 1.22 (95% CI = 1.04, 1.42). Among women with CD4 cell counts between 200 and 499 cells/mm3 the pregnancy rate ratio associated with seropositivity was 1.09 (95% CI = 0.95, 1.25), and in the women with CD4 cell counts below 200 cells/mm3 the pregnancy rate ratio was 1.04 (95% CI = 0.75, 1.42). As noted earlier, infected women reported a lower average frequency of intercourse than uninfected women (Table 1). If HIV infection was causally associated with declines in sexual activity we might expect frequency of intercourse to further decrease with stage of disease in infected women. Cross-tabulations using the categorical variables in Table 1 indicated that CD4 count was not associated with reported frequency of intercourse among the infected women in our study (p=.49) (results not shown). Discussion HIV-infected women had a history of higher pregnancy and pregnancy loss rates than uninfected women in this study. The association between infection and lifetime pregnancy rates was strongest among the youngest women in our sample. After adjusting for confounding by a number of independent predictors of fertility outcomes, the positive association between HIV infection and lifetime pregnancy rates was of borderline significance, and the association between HIV infection and pregnancy loss disappeared. In multivariate subset analyses, HIV-1 positive women at the earliest stages of infection exhibited a significantly higher fertility rate than uninfected women. In the absence of information on the date of seroconversion, we assumed that all person-time contributed by currently infected women represents infected (exposed) person-time. It is possible, however, that women were not all infected from the start of the observed person-time. If the relatively high pregnancy rates observed among HIV-positive women occurred primarily before they were infected, the results might overestimate the positive association between HIV-status and fertility. We used women's reports of the year of each pregnancy to assess whether the positive association between infection and fertility changed over time, as currently-infected women crossed into the likely period of seropositivity. Notably, the positive association between HIV status and fertility did not change over time. Subset analyses using infected women at different stages of disease demonstrated that the positive association between HIV infection and fertility was confined to women at early stages of infection. These results suggest that the fertility rate ratio would continue to decline with further follow-up and disease progression. Early follow-up studies in Zaire and the U.S. observed lower fertility among women with advanced disease compared to women with asymptomatic infection,12 ,13 but sample size and data limitations precluded control for potential confounders of this association. In one of the few prospective studies of HIV and fertility, Gray et al followed a cohort of HIV-1 infected women in Uganda followed for three years and found that infected women had a 27% lower pregnancy risk than uninfected women. The present study is somewhat unique from Gray's in that it focuses entirely on the association of HIV with fertility in women who were asymptomatic and unaware of their HIV status during the observation period, and therefore not likely to have changed their behavior as a result of their status. Using retrospective antenatal clinic data and methods similar to those presented here, Desgrees du Lou et al found that HIV-infected women in the Ivory Coast had up to 13% fewer pregnancies than uninfected women.15 Infected women in that population also were at greater risk of experiencing an abortion or stillbirth. In addition to the socio-demographic characteristics that were included in the analysis by Desgrees du Lou et al, the analyses presented here controlled for other important predictors of fertility, namely contra-ceptive use, prior exposure to sexually transmitted diseases and recent exposure to sexual intercourse. Investigators have suggested a number of biologic and behavioral mechanisms by which HIV-infection might be associated with subfertility and pregnancy loss. These include menstrual dysfunction, excessive weight loss, and compromised fertility in male partners. Closer scrutiny reveals that the evidence for many of these postulated mechanisms requires further elaboration. One possible mechanism by which HIV-infection might suppress fertility is through increased rates of fetal wastage. In a follow-up study of this study population, the infected women did not experience higher rates of pregnancy loss compared to uninfected women.16 Where infection has been positively associated with pregnancy loss, a proposed mechanism for the association has been vertical transmission of HIV in utero.17,18,19,20 It appears however, that the risk of vertical transmission during pregnancy increases with mother's disease stage as measured by viral load or CD4 cell count,21,22,23 and can be as low as 2-5% for women with low viral loads.24,25 This is consistent with the finding that the risk of fetal wastage increased with mother's disease stage during follow-up in this population. It has also been suggested that the immuno-suppressive effects of HIV infection somehow increase the rates of spontaneous abortion. We27 found no evidence to support this theory. In fact a study of the immunological impact of HIV-infection on pregnant women found no difference between infected and uninfected women on changes in T-lymphocyte subset profiles during pregnancy.28 Some have suggested that HIV infection may be causally associated with menstrual dysfunction, resulting in lower pregnancy rates. But research on this association has yielded mixed results, with some investigators observing an association between HIV infection and menstrual dysfunction,29,30 and others finding no such association.31,32,33 Loss of at least 10% of body weight is a defining characteristic of HIV disease stage three according to the World Health Organization disease classification system.34 There is evidence that loss of 10-15% of body weight is also associated with the incidence of amenorrhea in the general population.35 While weight loss-induced amenorrhea may represent a pathway by which advanced illness can compromise fertility, this mechanism is unlikely to affect women comparable to those in our study, who are infected but largely asymptomatic. HIV might also compromise fertility through its biological effects on infected male partners. Two studies found an association between advanced disease stage and poor performance on semen parameters that affect fertility;36,37 these studies found no association between early disease stage and values of these semen parameters. Nearly all of the proposed mechanisms of an association between HIV infection and suppressed fertility are relevant primarily for women at clinically advanced stages of disease. They do not preclude the possibility that women at early stages of infection may experience higher pregnancy rates than their uninfected counterparts. Eighty-four percent of the HIV-infected women in our study were at stage one upon recruitment, using a modified version of the World Health Organization's recommended staging system,38 and 99% were at stage one or two. Heterosexual transmission of HIV requires intercourse in the absence of barrier contraception; it is possible that infected women were more exposed to unprotected intercourse than uninfected women. Although the infected women in this study reported slightly higher rates of contraceptive use than the HIV-1 negative women, they only reported the number of months they contracepted, and gave no information on the consistency of use. Moreover, the most prevalent method of contraception among both exposed and unexposed women in our sample was the condom, which, unlike long-term methods, is highly susceptible to inconsistent and even sporadic use.39,40 HIV-1 positive women may be at greater risk of pregnancy as a result of greater exposure to unprotected sexual activity. Alternatively, a number of studies have indicated that a common route of HIV transmission to married women is through their husbands' extramarital sexual relationships.41,42 Studies have also suggested that married men's exposure to other sex partners is greatest during periods of post-partum abstinence.43,44 These findings together would imply that women who bear many children are at greater risk of HIV infection than women with lower fertility rates, because their spouses are more likely to contract HIV during the post-partum period and subsequently expose their wives. Again, however, our finding that the relative fertility rate remains unchanged over time suggests that fertility in infected women does not necessarily decline after seroconversion. The original study design did not include a mechanism for collection of data from the male partners of the women in the study. Indeed, one of the conditions of the study was the assurance of confidentiality for the participating women. Therefore information was not available on the disease status or fertility of male partners of the study participants. It is possible that variations in the fertility levels among the HIV-positive women were due at least in part to differences in the disease status of their male partners. Our results concur with another recently published cohort study indicating that HIV-1 infected women exhibit higher fertility than uninfected women.45 These findings may have implications for projections of population fertility rates, HIV prevalence and the incidence of orphanhood in the face of the HIV epidemic. Estimations of the effect of HIV infection on fertility have led investigators to propose that population fertility may decline by as much as 0.4% for each percentage point of HIV prevalence in the female population.46 Our findings suggest that the effect of the epidemic on population fertility can vary substantially according to the state of health of those infected, and may have a much milder effect on population fertility where a large proportion of infections are sub-clinical. Our findings call for caution when adjusting clinic-based estimates of HIV-1 prevalence upwards to account for expected subfertility among infected women. In populations similar to our sample, these adjustments may actually produce overestimates of HIV prevalence. It has also been suggested that subfertility of HIV-1 positive women will have an advantageous effect on the incidence of orphanhood.47 Projections of orphanhood incidence vary by as much as 40-50% depending on whether they adjust for the supposed suppressive effects of HIV on fertility. Our findings call into question the extent to which subfertility will contain the incidence of orphanhood. The women in our sample represent a select group of women of reproductive age in Dar es Salaam in that they are necessarily fecund and users of antenatal care services. Notably, data from the 1996 Demographic and Health Surveys (DHS) in Tanzania indicate that eighty-three percent of women in Dar es Salaam aged 15-34 used antenatal care services of some kind during their pregnancy, and 92% of these women had received antenatal care by 23 weeks gestation.48 The positive association between HIV infection and fertility in this study suggests that the negative associations observed in other studies are not universal. In particular, the inverse associations observed by others may not apply to women at early stages of the disease. The associations observed here can have important consequences for the incidence of orphanhood, estimates of the effect of the HIV epidemic on population fertility levels, and efforts to estimate population prevalence of HIV using serosurve-illance data from antenatal clinics. Acknowledgements The authors gratefully acknowledge the women who participated in this study and the research team responsible for data collection. We also thank Gretchen Antelman and Ellen Hertzmark for data management and programming and Sidney Atwood for technical support of statistical analyses. This study was supported by a grant from the National Institute of Child Health and Human Development (NICHD R01 32257). References
© Copyright 2006 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh06036t1.jpg] [rh06036t3b.jpg] [rh06036t4.jpg] [rh06036t2.jpg] [rh06036f1.jpg] [rh06036t3a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}