 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
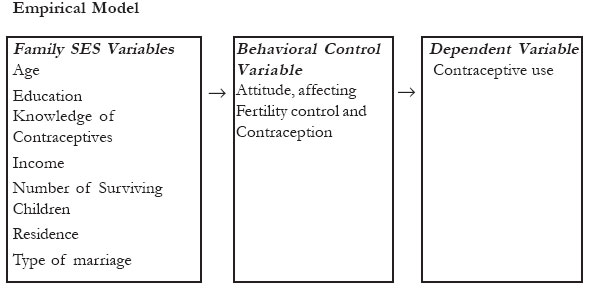
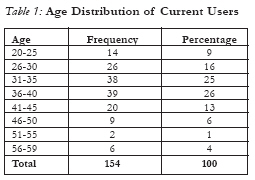
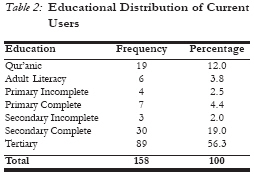
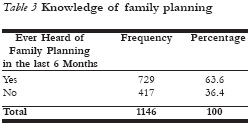
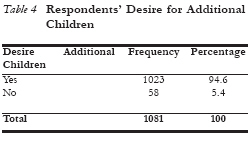
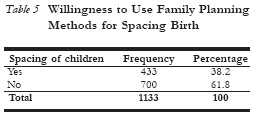
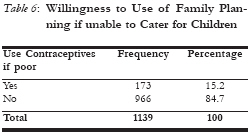
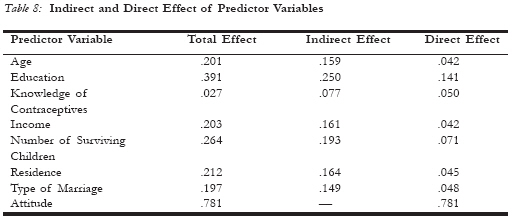
African Journal of Reproductive Health, Vol. 10, No. 3, December, 2006, pp. 53-65 Male Knowledge, Attitudes, and Family Planning Practices in Northern Nigeria Mustapha C. Duze1 and Ismaila Z. Mohammed2 1Professor Mustapha C. Duze, Department of Sociology, Bayero University, Kano and 2Dr Ismaila Z. Mohammed, Department of Sociology, Bayero University, Kano, PMB 3011 Kano, Nigeria, Email ismailazango@yahoo.com Code Number: rh06037 Abstract This paper examines the linkages between socioeconomic characteristics, attitudes, and familial contraceptive use. Past family planning programs in Nigeria have been mainly directed toward women. However, because northern Nigeria (and to a slightly lesser extent all of Nigeria) remains a patrilineal society characterised by early age at marriage for women, men at present continue to determine familial fertility and contraceptive decisions. Consequently, at least for the time period relevant for current policy planning purposes, the willingness of husbands to adopt or allow their spouses to use family planning practices will determine the pace of fertility reduction in Nigeria. The results suggest that there is high knowledge of contraceptives, a generally negative attitude towards limiting family size for economic reasons, and consequently low rates of contraceptive use. Respondents who were willing to use contraceptives were more willing to use them for child spacing purposes than explicitly for limiting family size. Path-analytic decompositions of the effects of predictor variables show that education has the largest direct and total effects on contraceptive use while specific knowledge of contraceptives has the smallest direct and total effect (as well as a paradoxical negative direct effect when education is included in the model). Most importantly, attitudes have the largest direct effect on contraceptive use with a standardized coefficient value of 781. Thus, since knowledge of contraceptive is already high among even those respondents who do not use contraceptives, the attitudes of males are especially important for decisions about contraceptive use. As a result, family planning programs that continue to focus solely on women will continue to achieve only limited successes in northern Nigeria (and likely in the many patrilineal societies where similar programs are pursued). (Afr J Reprod Health 2006; 10[3]:53-65) Key Words: Male Contraception, Family Planning, Attitude, Northern Nigeria Résumé Connaissance, attitudes et pratiques de la planification familiale chez les hommes au Nigéria du nord. L'article étudie les liens entre les caractéistiques socio-économiques, les attitudes et l'usage familial du contraceptif. Les programmes de la planification familiale dans le passé ont été dirigés vers les femmes. Néanmoins, à cause du fait que le Nigéria du nord (et jusqu'à un certain point tout le Nigéria) demeure une société patrilinéaire caractérisée par un mariage précoce pour les femmes, les hommes à préseut continuent à déterminer la fécondité familiale et les décisions sur la contraception. En conséquence, au moins pour la période pertinente pour les causes de la politique actuelle sur la planification, la volonté des maris d'adopter ou de permettre à leurs femmes d'employer les pratiques de la planification familiale determinera le rythme de la réduction de la fécondité au Nigéria. Les résultats montrent qu'il y a une haute connaissance des contraceptifs, une attitude généralement négative envers la limitation de la taille de la famille pour des raisons économiques et en conséquence il y a de bas taux d'emploi des contraceptifs. Les enquêtés qui voulaient employer des contraceptifs étaient plus disposés à les employer pour l'espacement des enfants plutôt que d'un moyen explicit de limiter la taille de la famille. L'analyse des effets des variables des indices ont montré que l'instruction a les plus grands effets directs compréhensifs sur l'usage du contraceptif alors qu'une connaissance spécifique des contraceptifs a le moindre effet direct et compréhensif (aussi bien quin effet direct négatif paradoxal quand on inclut l'instructon dans le modèle). Le plus important est que les attitudes ont le plus grand effet direct sur l'usager des contraceptifs avec une valeur de coefficient de 781. Ainsi, puisque la connaissance des contraceptif est déjà élevée même chez ces enquêtés là qui n'emploient pas les contraceptifs, les attitudes des hommes sont surtout importantes pour la prise des décisions à l'égard de l'usage des contraceptifs. En conséquence, les programmes de la planification familiale qui continuent à se concentrer uniquement sur les femmes ne cesseront d'accomplir des succès limité au nord du Nigéria (et probablement dans beaucoup de sociétés patrilinéaires où les programmes similaires sont en cours.) (Rev Afr Santé Reprod 2006; 10[3]:53-65) Introduction Many developing societies are characterised by rapid population growth, due to high fertility and high but declining mortality. In sub-Saharan Africa the rate of population growth is one of the highest in the world, with an average growth rate of 2.80%1. This is a consequence of persistent high fertility, although infant mortality has declined in recent years and life expectancy has increased. The rate of population growth in Nigeria is 3.0% per annum largely because of high fertility and moderate mortality2. In spite of an increased emphasis on family planning programmes in the region, the impact on fertility in sub-Saharan Africa compared to other regions of the world is low. One reason offered for why family planning in Asia has been relatively more successful than in sub-Saharan Africa is that Asia has experienced significant socioeconomic change. In addition, vigorous population campaigns in the region have involved local community leaders and other influential people. The campaigns were aimed at creating the desire to limit family size. Typically, concerted efforts were made to increase the desire for small families and then to provide contraceptives and family planning services as a means of controlling fertility. Similar efforts have gained momentum in sub-Saharan Africa but with little results. The economy in the region continues to be agriculture based, with populations that are predominantly rural. Early marriage and low levels of contraceptive use continue to be normative. In fact, until quite recently there was no apparent sign of fertility decline in the 45 countries of the region, with the exception of Zimbabwe, Botswana, and Kenya.1 One factor that might contribute to the lack of success of the African population control programmes may be that they tend to be directed toward women only, ignoring the role of men in contraceptive decisions. The Hausa society located in northern Nigeria is patrilineal with a strong male influence on many household decisions including those involving reproduction. This makes the attitudes of male toward family planning and contraceptive use a significant factor influencing the overall fertility level in the region. Moreover, there are some social and institutional factors that favor men in matters affecting the family. This is related to the significant role men play as household heads, custodians of their lineage and providers for their family. Due to these significant roles men play, decision-making power within the family and society largely lies with men.3 Given the decision-making powers of Hausa men and the fact that they also control economic resources, it is important to consider their attitudes toward and willingness to use contraceptives to control family size. Statement of the Problem The present population of the world is about 6.2 billion people with four-fifth of them living in the developing societies. The population of the world is increasing by 90 million annually, with 90% of the increase occurring in developing societies. This is because population growth rate in developed societies is considerably lower than in developing societies. In the past, the need for family planning had been rationalised by a significant number of women who state a desire to cease childbearing.4 However, in spite this apparent unmet need for contraceptives, very little has been achieved in aggregate fertility reduction. The lack of success of the family planning revolution is attributable to the failure of the programmes to recognise the importance of male attitudes and attributes in fertility decision-making. While women are more likely than men to want to discontinue child bearing, however, evidence from including men in formation of joint preference measure appears to indicate that determining contraceptive demand from women alone leads to gross overestimation of demand due to the neglect of men's role and attitudes. Hausa people are patriarchal, characterised by strong male dominance. Consequently the attitudes of males toward contraceptives and their willingness to use or allow their spouses to do so are very significant to population change. For instance in many government-owned hospitals women might not be able to obtain family planning services without the consent of their husbands. In view of the above, this research addressed the following question: What is the attitude of husbands towards family planning, family size, and contraceptive use within the marital union? Conceptual and Empirical Model In an attempt to explain fertility behaviour, the proximate determinants framework not only explained specifically how proximate determinants influenced fertility, but also consider the factors that influence them.5, 6 The role of attitudes in this model is less clear. For instance, attitude, that is the predisposition of an individual to favourably or unfavourably evaluate an object, will influence his behaviour. In this case, the attitudes of people toward family planning and contraception will influence adoption of family planning methods. The attitudes of an individual may be influenced by a number of factors such as education, age, income, influence of other individuals around him, etc. Typically favourable attitudes to family planning methods will translate into use and can be expected to affect fertility. This makes the attitudes of males significant since most decisions to use contraceptives are influenced by men, particularly in sub-Saharan patrilineal societies like the Hausa.7, 8, 9 The focus in the above model is on women and the role of attitudes is explicitly not considered. The empirical model used in the proposed study modifies the Bongaarts model to make it more applicable to men and to explicitly consider psychological factors. This model indicates the relationship between socioeconomic status variables, attitudes, and one proximate determinant: contraceptive use, defined as the dependent variable. The empirical model is presented below. In this model, the background and socio-economic characteristics are posited to influence contraceptive use through their effect on attitudes. Literature Review The determinants of fertility in developing societies are influenced by the demand for a certain number of children, their survival and assessment of their survival. Within the context of these factors, people evaluate availability and cost of fertility regulating mechanisms. The cost revolves around the individual and institutional characteristics. For instance, the individual socioeconomic status may regulate the cost while the institutional framework may raise or lower the cost of contraception through encouraging or discouraging its adoption.10 In this context the subjective cost of fertility regulation in Hausaland is high, as children are seen as a blessing to the family. Moreover, there is the feeling that it is not within human capacity to determine the number of children one should have. In addition, people are still uncertain about the possible side effects of contraception, which also raises the subjective cost. With high demand for children, the motivation to regulate fertility is very low. 11 Apart from the socio-psychological cost, economic cost is also important as well as the time required in obtaining the services. In Nigeria and Kano State in particular, health facilities are largely concentrated in urban centres where over 80 percent of public and private hospitals are located.12 This makes it difficult for rural people to obtain the services due to the low level of motivation to use contraceptives.
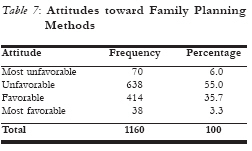
In addition, children in Nigeria are generally valued as economic assets and insurance in old age. Due to this, people tend to have large families with preference for male children, which may delay the usage of contraception by couples who do not have male children. Caldwell's wealth flow theory also emphasises the value of large families in less developed societies. The main reason for high fertility in most developing countries, particularly in the rural agricultural population, is that children are productive agents. Furthermore, the practice of subsistence agriculture with heavy reliance on family labour contributes to high fertility. Due to this, large family is a symbol of prestige. High fertility level in sub-Saharan Africa is associated with early marriage and low contraceptive use.13 Non-marital fertility is, however, low in some societies due to social pressure against premarital sex, and marital fertility is low due to the practice of postpartum abstinence, widow remarriage and long duration of breastfeeding.14 Consequently, African family structures affect individual spousal perception of child-related processes and affect reproductive decision making and actual fertility behaviour. This is because men in these societies contribute more resources in running the family, which gives them more authority. People have pride in their children particularly male children due to present and expected benefits to be derived from them. Similarly, children provide satisfaction by helping in the home, on the farm and provide financial assistance to the family in the absence of organised social welfare and security programmes.3 Men as husbands and heads of the households control the sexuality of their wives. Thus, the perceived wishes of the husband may influence the behaviour of the wife. For instance, a woman wishing to use contraceptives may fail to take the initiative if she understood the attitudes of her husband to be negative. About 88 percent and 78 percent of men and women in Nigeria respectively have indicated that the views of men are more influential in family planning decision-making. This is because men make reproductive decisions, decide whether or not to have sexual intercourse, decide on the duration of abstinence to some degree and make the choice about the contraceptive method the wife is to use.3 In patriarchal Hausa society, with men having absolute power over certain family issues, it has been, for instance, found that 78 percent of the spouses among Hausa and Kanuri interviewed, agreed that the wife has no say on family size. On the other hand only 6.7 percent of the Igbo, 10.5 percent of the Ijaw, and 11.5 percent of the Yuroba gave the same response. This further confirms the significant role men play in reproductive decision among the Hausa people.16 The role of men in making family planning decision is becoming significant especially in sub- Saharan Africa. A number of surveys carried out suggest that husbands are actively involved in making family planning decisions. In Sudan, most family decisions are made by men including decision on family planning. However, most men reported large family, as ideal and only a small proportion prefer small family size. About 80% opined that limiting family size is against their religion. However, in terms of knowledge, 94 perent of men have knowledge of family planning methods. The familiar methods include pills, injections and rhythm, with 91 percent of the men indicating willingness to approve contraceptive use if the health of the woman will be endangered by frequent pregnancy.7, 17 The inclusion of men in Zimbabwe has affected the success of the family planning programme. This is because there are many women who desire to use family planning but could not do so because of unfavourable attitudes of their spouses. The attitudes of men in Zimbabwe are favourable as indicated by their approval, use and involvement in family planning decision-making. Because of this involvement of men in Zimbabwe, there is high prevalence of contraceptive use compared to many countries in sub-Saharan Africa. Typically, in about 78 percent of the decision to use contraceptives, men were involved while wife's involvement was reported in about 46 percent of the decisions. Level of contraceptive knowledge was high and about 84 percent of the men approved usage of contraceptives.9 In a patriarchal society like Zaire children belong to the husband and an extension to his extended family or clan. The husband pays dowry in marriage to the bride's family as a compensation for the loss of her services and expenses of upbringing. In return, she is expected to contribute to the husband's family in terms of labor and bearing of children. For this reason, a woman cannot cease child bearing voluntarily because it will be seen as failure of the wife to fulfill her obligation.18 Knowledge of contraceptives in sub-Saharan Africa varies from country to country. Furthermore, knowledge varies with age and place of residence. The differences are most pronounced in West Africa. Urban residents have more knowledge of contraceptives than the rural residents, young people more knowledgeable than older people, and educated men more knowledgeable than uneducated men.19, 20 The differences in usage of contraceptives in Nigeria reflect education and regional differences. For instance, only 2 percent of women without education were using contraceptives, while 30 percent of women with secondary education use a method. The regional differences are also glaring, with only 1 percent of women in the northeast using contraceptives, against 15 percent of women in the south west.21 Consequently, there is a general negative attitude towards use of family planning. Negative attitude results from low literacy level5 and prevailing religious, political and cultural beliefs of the people. Inaccessibility of the services, especially in rural areas, may be a limiting factor, while the apparent benefits parents derive from their children do not support fertility control. Consequently, there is a desire for large family resulting from positive values attached to family life, marriage and procreation. The desire for a large family is deeply entrenched in the fundamental belief that children are a gift from God, which makes people desire as many children as God grants. This belief is buttressed in the dominant religions in the country, Islam and Christianity. All the ethnic groups abhor barrenness, while women with many children among some ethnic groups are honored. For instance among the Igbos "Ewu-Ukwu" is a ceremony for mothers of ten or more children. Women who attain this position of distinction enjoy some privileges with high esteem.22 In addition; the perception of family planning by people in northern Nigeria is remarkably influenced by the religion of the people, which is deeply rooted in their culture and tradition. The negative perception is also related to the external source of the program. The programme is viewed as an attempt by western powers to curtail the population of the Muslims.23 Data and Method The population of the study consists of Hausa males currently married between the ages of 18-59 years. This is because the study is interested in assessing the influence of males' attitudes toward family planning and the subsequent decision to use contraceptives. The study was conducted among the Hausa people, a dominant ethnic group in northern Nigeria. The choice of this ethnic group was largely predicated on the traditional character of this patriarchal group and its high fertility. The Hausa people constitute a significant proportion of the population in Nigeria, the largest country in Africa. The Hausa people are undergoing rapid socioeconomic change manifested in expansion of education and urbanisation. A sample of one thousand one hundred and sixty (1,160) respondents was drawn from both rural and urban areas. The sample size was considered adequate due to the homogeneous nature of the population. In order to draw the sample, a combination of sampling methods was employed appropriate to the sampling units. A multistage selection process was adopted involving cluster, simple random and systematic sampling methods. Quantitative data were gathered for this study in 1998. Retrospective and prospective data were gathered from the respondents regarding their fertility and contraception. Respondents were asked about number of children ever born, desire for more children, last use of contraceptives, current use, and future use where applicable. Likert scale was used to measure attitudes of respondents using a combination of negative and positive statements pertaining to practices related to family planning methods. Respondents indicated their responses ranging from strongly agree to strongly disagree on a four-interval scale. The main instrument for the data collection was a questionnaire administered in the form of interview conducted in Hausa language. Six research assistants; mainly graduate and undergraduate students from Bayero University Kano were recruited to assist with the data collection. All the research assistants were indigenous Hausa people, familiar with the norms and values of the respondents. Path Analysis was used to decompose the zero order correlation between the variables into direct and indirect effects. Each path coefficient reflects the magnitude of the direct effect of that particular variable from which the path derives on the dependent variable to which the path leads. The magnitude of the coefficient is an estimate of the net change in the dependent variable that could result from one standard deviation change of the independent variable, which is equal to a standardized regression coefficient or Beta weight. In the path analysis an equation consisting of the variables upon which it is assumed to be dependent and a term representing the residuals represent each dependent variable in a causal model. For each independent variable in the equation, there is a path coefficient indicating the amount of expected change in the dependent variable as a result of a net change in the independent variables. The effects of other independent variables not included in the model are represented by a residual term. Results Table 1 shows the age distribution of current users of contraceptives. The table shows an increasing use of contraceptives up to the age 40 years and declines from age 41 years. For instance only 9 percent of current users of contraceptives are between the ages of 20-25. This is largely because many respondents in the age group are yet to have their first child, and as earlier noted most couples will only start using contraceptives after having their first child. Current users of contraceptives between the ages of 26-30 years constitute 16 percent and the rate of use increases reaching its peak among users in the age group of 36-40. However, from age 41-45 years, the proportion of current users decreases by about half to 13 percent. Furthermore, the least percentage of current users (1%) is among respondents in the age group of 51-55 years. This shows that 67 percent of the current users of contraceptives are between the ages of 26-40 years and only 24 percent are between the ages of 41-59 years. This implies that contraceptive use is more prevalent among individuals in the middle age categories while on the other hand older people are not inclined to use contraceptives due to lack of desire to do so as some of them may not be sexually active. Table 2 shows the educational distribution of current users. The table shows that 15.8 percent of current users are those without any form of western education and 6.9 percent have attained some form of western education (primary, incomplete to complete). The proportion of current contraceptive users who have attained complete secondary education is 19 percent, which is almost quadruple the percentage of respon-dents with some form of western education. The highest proportion of current user of contraceptives comes from those with high level of western education with 56.3 percent. This shows a positive relationship between education and contraceptive use. In other words, among those who currently practice contraception, education is a very important factor. Knowledge of contraceptives among the respondents is generally high with 63.6 percent of the respondents indicating knowing at least one method. Knowledge of family planning methods is associated with place of residence, age and education. (Table 3) Table 4 indicates that desire for additional children is common among the respondents, 94.6 percent want additional children. However, a large proportion of the respondents did not give an exact figure of the additional number of children they want. Even among those who want to have a specific number, 66 percent want to have over 5 children. Consequently, large family size is desired which possibly accounts for the negative attitude toward family planning method by large proportion of the respondents. Table 5 shows that 38.2 percent of the respon-dents are willing to use and allow their spouse to use family planning methods in order to practise child spacing. This clearly shows the possibility for improvement in the number of people willing to use contraceptives. On the other hand, 61.8 percent of the respondents are not willing to use any family planning method to space birth. However, most men do not object to breast-feeding, which has contraceptive effects, which they may not be aware of. In addition, the culture of Hausa people and the religion of Islam do not object to spacing of children. In particular the Hausa culture strongly supports child spacing and discourages short birth intervals Kwanika. Economic reasons have been observed as an explanation for declining fertility in Europe, and many theories have been put forward to support that. However, Table 6 shows that inability to cater for children in Hausa society is not a strong reason for people to use family planning methods. (Table 7) It is indicated in the table that 84.7 percent of the respondents are not willing to use or allow their wives to use family planning methods on economic grounds. Only 15.2 percent of the respondents are willing to use or allow their wives to use contraceptives on economic grounds. This is largely related to the influence of Islam on the people (Islam discourages people from stopping child bearing because of economic reasons). In addition, there is s strong belief among the people that every child delivered is accompanied by his wealth. Furthermore, children, especially in the rural areas assist parents with work on the farm and with house chores. The attitudinal disposition of the respondents towards family planning methods is generally unfavorable, with 55 percent of the respondents having unfavorable attitude and 35.7 percent having favorable attitude. This is possibly related to the cultural and religious beliefs of the people which discourage the practice unless on medical grounds. Results of Path Analysis In an attempt to analyse the factors influencing the use of contraceptives, a distinction was made between socioeconomic variables (age, education knowledge of contraceptives, income, number of children, place of residence and type of marriage) and the proximate determinant (attitude). The proximate determinant in this regard is the psychological readiness of an individual to act, which is closely, associated with attitude. The assumption is that the variables affect use of contraceptive through the proximate determinant, attitude, by changing or modifying an individuals’ attitude. The result is presented in Figure 2 and Table 8. Table 8 presents the decomposition of the total effect into direct and indirect effect. The decomposition into direct, indirect and total effects of the predictor variables reveals that attitude has the largest direct and total effect on contraceptive use. In other words attitude has a significant effect on contraceptive use and is an important mediator between the predictor variables and contraceptive use. Furthermore, all the predictor variables have a relatively larger indirect effect than direct effect. The significance of the entire predictor variables is minimal without a positive attitude. Essentially, attitude which has largest direct and total effect (.781) is very crucial in determining behaviour, as a favorable attitude is likely to lead to contraceptive use. Discussion The direct effect of education on contraceptive use in standardised coefficient is .141 and the indirect effect of education via attitude is .250. Thus, the total effect of education on contracep-tive use is very large (.391). In fact the total effect of education is larger than the total effects of each of the other predictor variables on contra-ceptive use. The large effect of education on contraceptive use is related to the role of education in empowering individuals to make rational decisions and understand that it is possible to control fertility using family planning techniques. In other words the development of the consciousness about the ability to decide is critical and education is crucial in that respect. Age and income on the other hand tend exert a significant total effect on contraceptive use with a substantial portion of their total effect being mediated by attitude (.159 and .161 for age and education respectively). Knowledge of contraceptive is the only predictor variable having a negative direct effect on contraceptive use. Of all the predictor variables knowledge seems to have a relatively smaller direct, indirect and total effect on contraceptive use. In other words it only explains a relatively amount of the variation in contraceptive use (total effect .027). Knowledge does not seem to have significant effect due to the nature of the media through which information on contraceptive were communi-cated. As earlier noted large proportion of the respondents obtain information on contraceptives through radio, friends and posters. These sources may not provide details required for individuals to have accurate information about contracep-tives in terms of effectiveness, side effects and methods of use. In addition, information from friends may not necessary be accurate. Emphasis is often placed on the side effects as means of discouraging people from adopting and using contraceptive methods in a predominantly pronatalist society. The negative direct effect of knowledge of contraceptive use is related to this unauthenticated information from friends in the community, which is further compounded by lack of effective outreach programs and centers in the communities. Better level of knowledge may not necessarily be associated with current use of contraceptives.6 The direct effects of age, income, education, number of children and type of marriage on contraceptive use are smaller than their indirect effects. With the indirect effect larger than the direct effect, it further shows the significance of attitude to contraceptive use. Essentially, awareness of and attitude toward contraceptives are affected by socioeconomic characteristics. The proportion of individuals living in urban areas with knowledge of contraceptives is twice the proportion of people with similar knowledge in rural areas. Furthermore, approval of family planning increases with increasing level of education, while young people tend be more aware of contraceptives and have a more favourable attitude. In addition, the tendency to approve use of family planning methods increases with increasing number of children.24 It is evidently clear that having access to information and approval of family planning methods are affected by socioeconomic characteristics, which subsequently assist in the formation of favourable attitude. It has been established that attitude to a great extent affects behavior. It is evident from table 8 that the indirect effect of education, age, income, residence and number of children largely work through attitude to affect contraceptive use because attitude has the largest direct and total effect on contraceptive use Type of marriage, either polygamous or monogamous, shows an indirect effect of .149 and a direct effect of .048. The indirect effect is larger than the direct effect, which means that individuals that are monogamous and have favourable attitude toward contraceptive use will be more inclined to use contraceptives than those in polygamous marriage. This is more particularly so due to competition to bear children among the co-wives. Individuals in polygamous unions are less likely to use contraceptive than people in monogamous marital unions. In addition, women in polygamous marriages have fewer numbers of children because the time with husband is shared, which reduces the possibility of conception.21 Education seems to have the largest total effect and the largest direct effect. However, the indirect effect of education is larger than its direct effect because duration of schooling is critical to use of contraceptives. This is very important because a large proportion of the respondents have only Islamic and primary education, which are often characterised by short duration. Furthermore, a large proportion of current users are among those with tertiary education, which is characterised by long duration of schooling. Education is a strong influential factor on contraceptive use through attitude. In essence, education exposes people to more information, provide knowledge and better understanding of the desire to use contraceptive. Increase in contraceptive prevalence increases with improved level of education. This further supports the notion that obstacle to rapid change in contraceptive behaviour is high level of illiteracy.7, 14, 21, 24 Conclusion The rate of population growth in Nigeria is 3.00%, which is among the highest in the world. Consequently, there is need to encourage the use of contraceptives in order to reduce the alarming growth rate. This is particularly important considering the age at first marriage among the Hausa people. It is, however, important to note that the attitude towards family planning method is not very favorable among a large proportion of the respondents. Use of family planning among the Hausa people is greatly influenced by their religion and social values. The small proportion of respondents who are willing to use or allow their spouse to use contraceptives for economic reasons typifies this. On the other hand the proportion of respondents willing to use or allow their spouses to use contraceptives for child spacing purposes is twice the proportion of those willing to use it for economic reasons. This may be largely related to religious beliefs of the people, and Islam, which is a dominant religion, does not encourage birth control for economic reasons. However, the culture of the people encourages child spacing and even Islam encourages women to breastfeed children up to a period of 24 months. In addition, the path analysis results show that all the predictor variables have relatively larger indirect effects on contraceptive use than the direct effects. Education has the largest direct, indirect and total effect on contraceptive use, while awareness of contraceptive has the smallest indirect and total effect on contraceptive use as well as a negative direct effect. Attitude has the largest direct effect on contraceptive use. In other words the mediating role of attitude between the predictor variables and contraceptive use is very strong. Furthermore, cultural and normative influence on contraceptive use is possibly strong, though these factors have not been included in the model. Policy Implications The rate of population growth in Nigeria is among the highest in the world. This is related to a number of factors, which include age at first marriage, use of contraceptives and negative attitude toward family planning methods. Consequently, there is the need to achieve a goal of improving the standard of living and quality of life of the people by reducing the rate of population growth in the society through encouraging fertility control. Findings from this study show that large family size is still desired, use of contraceptives is very low and generally unfavorable attitudes are displayed toward family planning. Results from the path analysis confirm the significance of attitude to contraceptive use. (1) Large number of the respondents still want additional children. In other words, in order to control population growth it is imperative to change the peoples' attitude toward large family size and the desire for such through extensive media campaign and individual contact by change agents. (2) Hausa society is still largely partrilineal with strong male dominance in areas of family planning decision-making including contraceptive decision. This means family planning programmes and services should be tailored to incorporate men through outreach programmes. In addition, female education should be emphasized as a means of empowering them. (3) Child spacing is widely accepted and practiced among the Hausa people. Therefore, this should be emphasised in family planning programs (4) One cogent reason for using family planning methods, is medical reason. That is a woman is allowed to use contraceptives if becoming pregnant will endanger her health or the health of the child. This point should be emphasised, as childbirth at close intervals is likely to expose women to health problems, which can contribute to the high maternal mortality rate in sub-Saharan Africa. (5) Young people seem to be more favourably disposed to family planning methods. In view of this, the main focus of future family planning programmes should be the young people and people of middle age. (6) There is a need to make a significant effort to establish outreach family planning programs in the rural areas where the least prevalence of contraceptive use was found. Acknowledgement The funding for this research was partly provided by Centre for Research and Documentation (CRD) Kano and Bayero University, Kano. CRD is a nonprofit organization based in Kano. References
© Copyright 2006 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh06037f2.jpg] [rh06037f1.jpg] [rh06037t7.jpg] [rh06037t5.jpg] [rh06037t6.jpg] [rh06037t1.jpg] [rh06037t3.jpg] [rh06037t4.jpg] [rh06037t8.jpg] [rh06037t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}