 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 10, No. 3, December, 2006, pp. 76-83 Knowledge of HIV/AIDS and Sexual Practi- ces among Adolescents in Benin City, Nigeria 1Wagbatsoma VA, 2Okojie OH. Corresponding: Department of Community Health, School of Medicine College of Medical Sciences, University of Benin, Benin City, Nigeria. Code Number: rh06039 Abstract A cross sectional study to determine the knowledge of HIV/AIDS and sexual practices of adolescents was undertaken in Benin City, Nigeria. Benin City the capital of Edo State, Nigeria, has 40 government owned secondary schools comprising 6 boys, 10 girls, and 24 mixed. Out of these 3 schools were randomly selected for survey viz; Adolor (boys only), Iyoba (girls only), Army Day (mixed). The sample size for the survey was 920 while the total population for selected schools was 1692 giving a sampling ratio of 1:2. Using the systematic sampling method and class register as sampling frame every other child was selected for the study. However, only 852 students consented to participate giving a response rate of 92.6%. An overwhelming majority of the adolescents were aware of HIV/AIDS but only 16.2% knew the cause of the disease. The submission that kissing, living with infected persons and sharing their utensils could lead to infection was an indication of ignorance. Sexual intercourse was the predominant route of transmission mentioned by 60.0% while multiple sexual partners was prevalent among age group 13-15 years. Playing with sharps, frequent clean head shave with unsterilised instruments in the barbing saloon and promiscuity were some of the activities that adolescents were involved in that could lead to HIV/AIDS infection. In conclusion, the knowledge of the study population was poor and correlates with their reckless sexual practices. Prevention is the best option to the disease. Better informed youths on HIV/AIDS will enhance the principle of prevention. (Afr J Reprod Health 2006; 10[3]:76-83) Key Words: Adolescent, Knowledge, Sexual Practices, HIV/AIDS. Résumé La connaissance du VIH/SIDA et les pratiques sexuelles chez les adolescents à Benin-City, Nigéria Arrière Plan: VIH/SIDA est une maladie sexuellement transmissible. La maladie a un taux de mortalité élévé et la fatalité la plus élévée est subie par les Africains. Les traditions culturelles, les croyances, la peur et les autres inhibitions ont empêché les enfants de cette région d'acquérir la connaissance au sujet du sexe et des maladies sexuellement transmissibles de la part de leur parents et leurs enseignants tandis qu'ils ont un grand désir de s'explorer, se rendant ainsi vulnérables à l'infection.
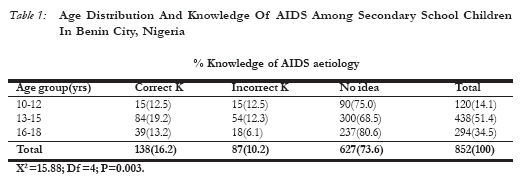
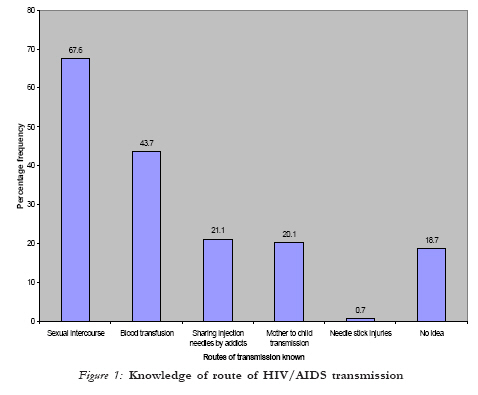
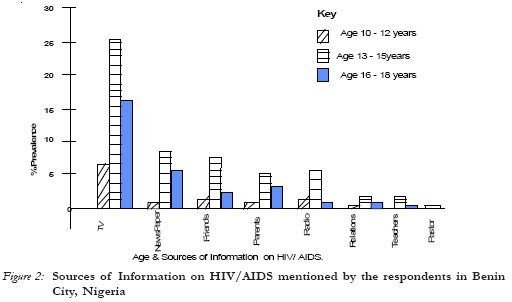
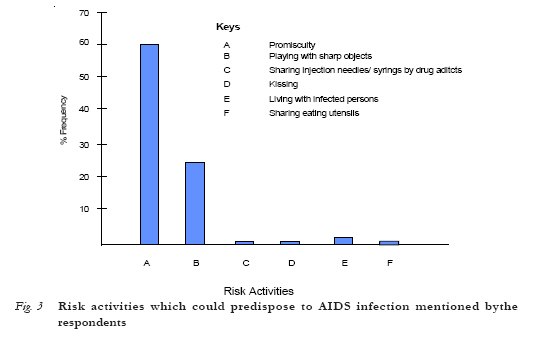
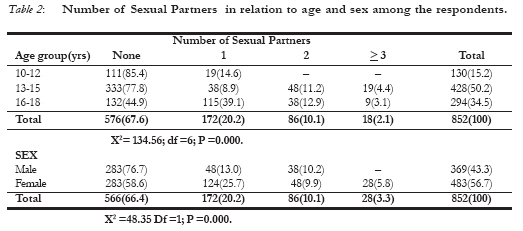
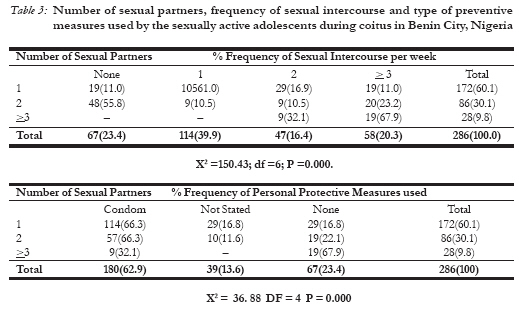
Introduction HIV/AIDS is one of the various sexually1-4 transmitted infections in the world today and ranks 10th5 among the world's killer diseases. Since the pandemic of HIV/ AIDS, 2.7 million children less than 15 years have died of the disease. Available statistics as at 1997 show that 1.1 million children less than 15 years live with AIDS, 590,000 acquired new infection while 460, 000 have died from the diseases globally5. Between 1997 and 2001 the population of infected adults including adolescent have doubled globally. In 2001, an estimated 40 million6 people world wide were living with HIV/AIDS comprising 37.1 million adults and 3 million children less than 15 years. Unfortunately, Africa South of the Sahara bears the greatest burden of the disease and adolescents in this region are the worse hit. About 88.2% of adolescents under 15 years living with HIV/AIDS in the world reside in Sub-Saharan Africa7 while 87% of infected adolescent are Africans5. Ages 15 - 24 years account for 60% of all new HIV cases in Africa while more females than males are infected at a ratio of 2:18. The first case of HIV/AIDS in Nigeria was a 13 year old sexually active adolescent girl reported in 19844 and since then the disease has been on the rising phase4,5. Nigeria has the 4th largest number of people living with HIV/AIDS and contributes about 8% of the global and 10% of Africa's HIV/AIDS burden9. The national prevalence rate has increased from 1.8% in 1990 to 3.8% in 1993, 4.5% in 1995, 5.4% in 1999 and 5.8% in 2001,while age specific prevalence reveal that age group 15 - 19 years (adolescents) are most affected with 6%9,10 confirming the vulnerability of this population. In Benin City, the sero-prevalence of HIV infection among adolescents aged 13 - 19 years was also high 11.4%, with a higher proportion for females 11.7% than 10.5% for males11. Meanwhile these adolescents who are at the greatest risk are not educated enough on sex related matters. Evidence12, have shown that they are aware of the disease but have poor knowledge12,13 of same. Cultural traditions, beliefs, fear and other inhibitions are known to prevent adolescents from acquiring knowledge from their parents and teachers while poverty, parents unemployment and the desire to explore themselves expose them to the risk of infection. Poverty is kown to significantly increase the likelihood of a number of unsafe sexual behaviour. In South Africa, poverty and orphanhood was reported to influence coerced sex and multiple sexual partner especially among female adolescent.14 This survey is aimed at finding out how much this vulnerable group and indeed leaders of tomorrow know about the disease and such practices they engage in that could predispose them to HIV/AIDS infection. Knowledge is the best tool for prevention of disease as it has the power to influence change in attitude and practice. It is therefore important that adequate and necessary health education on family health with emphasis on sex and HIV/AIDS be inputted in the school curriculum while the existing awareness campaign by The National Action for the Control of AIDS (NACA) should be intensified to empower the adolescents to improve their health. Materials and Method Study Area A cross-sectional study to determine the knowledge of AIDS and sexual practices of adolescents was undertaken in Benin City, Nigeria. Benin city the capital of Edo state, Nigeria, has 40 government owned secondary schools. The choice of government school for the survey was due to the large population of students which is representative of the adolescents in the metropolis. Advocacy/Ethical Considerations The principals of selected schools were visited and informed on the scope and benefit of the survey after which consent was obtained. Similarly, only those students who gave their informed consent participated in the study. Sampling and Sampling Methods Multi-stage sampling method was used. Stage 1, There are 40 public schools in Benin City, comprising 6 boys, 10 girls and 24 mixed. A school each was selected from each strata viz Adolor (boys only), Iyoba (girls only) and Army Day (mixed). The total population of each of the selected schools were 505, 546 and 461 respectively giving a total of 1692 children from JSS1 to SS3. The sample size for the survey was 920. The sampling fraction was derived from the product of 920/1692 and multiplied by the population of individual schools to give 275, 297 and 346 participants respectively. Stage 2: All the selected schools have an average of 2 arms per class and an arm each was selected from each class. Stage 3: Participants were selected from each class using the class register as sampling frame. Systematic sampling method was adopted to select every other child in the class.Although 920 adolescents were selected only 852 participated giving a response rate of 92.6%. The definition of adolescent by FMOH15 (10-19years) was adopted and only students that fell within the age bracket were eligible to participate in the study. For the purpose of this survey sexually active adolescents have been characterized by their early exposure to sex before the age of 15 years, frequent coitus, masturbation, promiscuity, high fertility and abortion16.The tool for data collection was structured questionnaire that was self administered which sought infor-mation on age, sex, knowledge of HIV/AIDS , source of information on the disease, mode of transmission and sexual practices of the adolescents. HIV or Virus was accepted as correct knowledge of cause of HIV/AIDS while any other cause proffered was recorded as incorrect knowledge. Data generated were collated and analyzed using PEPI18. The computer programme for epidemiological studies. Pearson's chi-square test was the statistical test of association used at 95% confidence limit. Results Of the 852 students studied 369(43.3%) were males while 483(56.7%) were females. Most 439 (51.4%) of the study population were in the age group 13 - 15 years followed by age group 16 - 18 years and the least were in age group 10 - 12 years (Table 1). An overwhelming majority 850 (99.8%) were aware of HIV/ AIDS. Table I shows age, knowledge of HIV/AIDS aetiology and route of transmission among the study population. Knowledge of HIV/AIDS aetiology was poor. Only 138(16.2%) had correct knowledge. Knowledge of HIV/AIDS improved with age and the relationship was found to be statistically significant (P=0.003). Meanwhile 87(10.2%) said the disease was caused by bacteria and evil spirit while most 627(73.6%) who claimed to be aware of the disease were completely ignorant of the cause of the disease. Among the different route of AIDS transmission mentioned by the adolescents ,sexual intercourse ranked first with (67.6%) followed by blood transfusion, (43.7%) and sharing injection needles by drug addict( 21.1%) among others (Figure 1). Television was the predominant source of information followed by newspapers and friends respectively as shown in (Figure 2). Regrettably, parents and teachers who should lead the sex education of the children lagged behind. Figure 3 represent some of the risk activities that students engage in which could predispose to infection. Sixty percent of the adolescents mentioned promiscuity. Playing with sharp objects like knives, blade, broken bottles as well as sharing injection needles/syringes among hard drug users were some of the high risk activities mentioned. A few (6.4%) had the wrong idea that kissing, living with infected persons and sharing their eating utensils could lead to infection as shown in (Figure 3). Two hundred and eighty-six (33.6%) of the study population were sexually active as shown in (Table 2). The ages of the sexually active students ranged from 12 - 18 years with a mean of 15.2 ± 1.9 years. Multiple sexual partners and promiscuity were more prevalent among age group 13 - 15 years. Adolescents within age group 16 - 18 years and females were more sexually active. Chi-square test shows a significant relationship between age and number of sexual partners (P < 0.000) while a significant difference in number of sexual partners existed between males and females. ( P < 0.000). Most of the sexually actives have coitus once weekly. Others (23.4%) have sexual intercourse but did not reveal the frequency per week. Meanwhile (20.3%) have sex thrice or more times weekly as shown in (Table 3). More than half the sexually actives use condoms as prevention against HIV/AIDS while (13.6%) did not specify the preventive measures used. Unfortunately, those who did not use any prevention during coitus have the highest number of sexual partners and are likely to accelerate the spread of the disease. Discussion The findings of the survey revealed that the students were aware of AIDS but had poor knowledge of its aetiology12, 20 - 23 33.6% of the respondents were sexually active compared to the 70.0% observed among a similar population22. Meanwhile, the mean age of 15.2 ± 1.9 years and age range of 12 - 18 years of the sexually active adolescents observed in this survey is an indication of early exposure to coitus among the study population. This is dangerous and bothers on ignorance of the population about the disease and requires proper education. Health education encourages behaviour that promotes health, prevents illness, cures diseases and facilitates rehabilitation25. It also gives members self confidence, self reliance and facilitates responsible health behaviour26. The frequency of sexual intercourse coupled with the multiple sexual partners among the respondents especially the females is dangerous and represents a high risk behaviour. Although changing attitude is much slower, less direct and less certain than changing knowledge and skills,27 it is however possible. Since students know that condoms could protect against HIV/ AIDS infection, its safe use to achieve the desired objective must be encouraged and sustained as the major route of HIV/ AIDS transmission is through unprotected sexual intercourse2-4,20-22,28. Knives, blades, broken bottles are some sharp objects that students handle and play with that could place them at the risk of infection as well as enhance crime. It is also possible that the current clean shave heads among male adolescents using the same sharp instruments could predispose to infection. Desmyster29 claimed that exposure to unsterilized needles and other skin pricing instruments is a possible means of HIV/AIDS infection. Although the use of injectable hard drugs may not be common in Nigeria as sniffed hard drugs, the likelihood of its use cannot be ruled out since it was proffered by the respondents. It is possible that transmission through sharing of needles may be minimal as needles/syringes are by far cheaper than the injectable drugs. Television was the main source of information on HIV/AIDS for the study population. The use of this medium for health education of this age group should be encouraged. However, the incessant power interruption in the country is a major handicap to this important source of information and needs to be improved upon. An important observation in this survey is the fact that friends ranked higher than parents as a source of information on sex and AIDS. Previous studies22,30 revealed that parents could influence their children and also have the primary responsibility to provide family life education. On the contrary peers seem to have overtaken parents in this function as family life educator. Since youths can influence themselves better1 and are more willing to share such information among themselves rather than with their parents, it is vital that adequate and appropriate information be imparted to them through health education programmes so that they would be able to transfer correct information to their peers. References
© Copyright 2006 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh06039f2.jpg] [rh06039t2.jpg] [rh06039f3.jpg] [rh06039t1.jpg] [rh06039f1.jpg] [rh06039t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}