 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
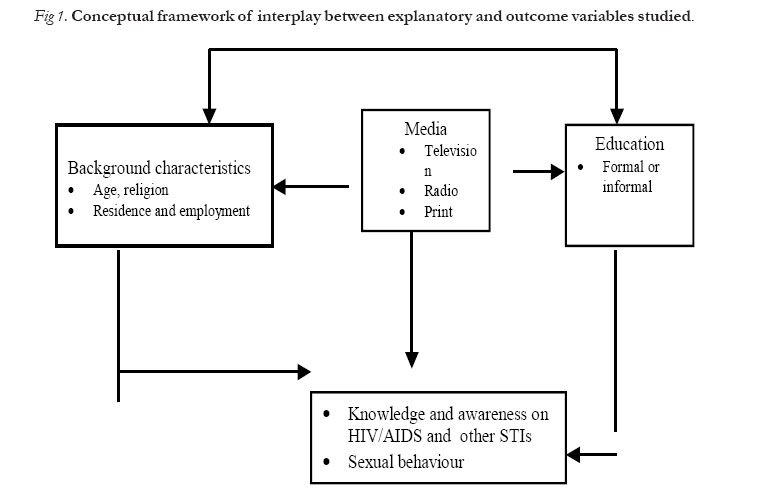
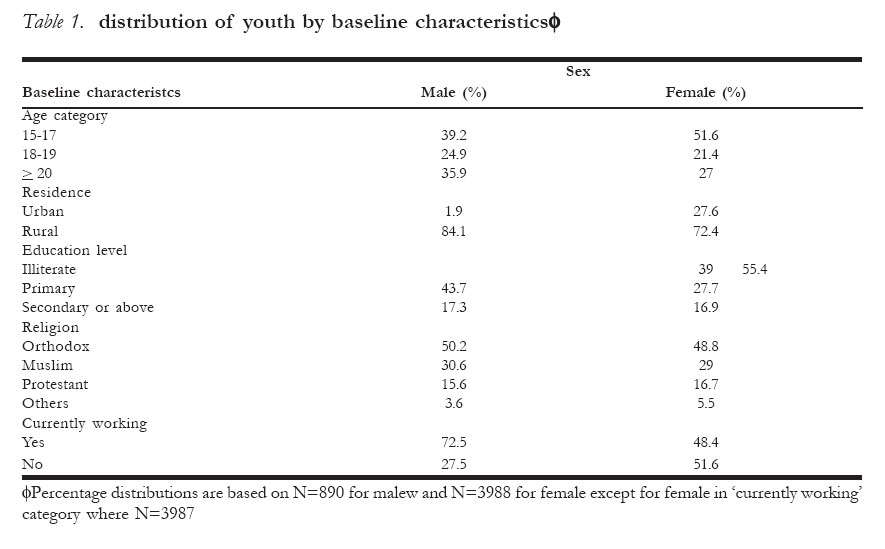
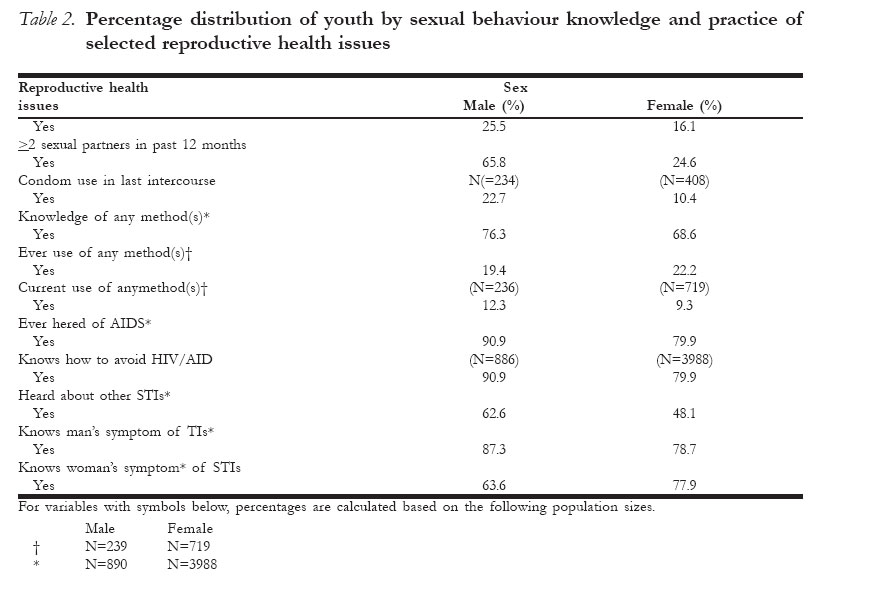
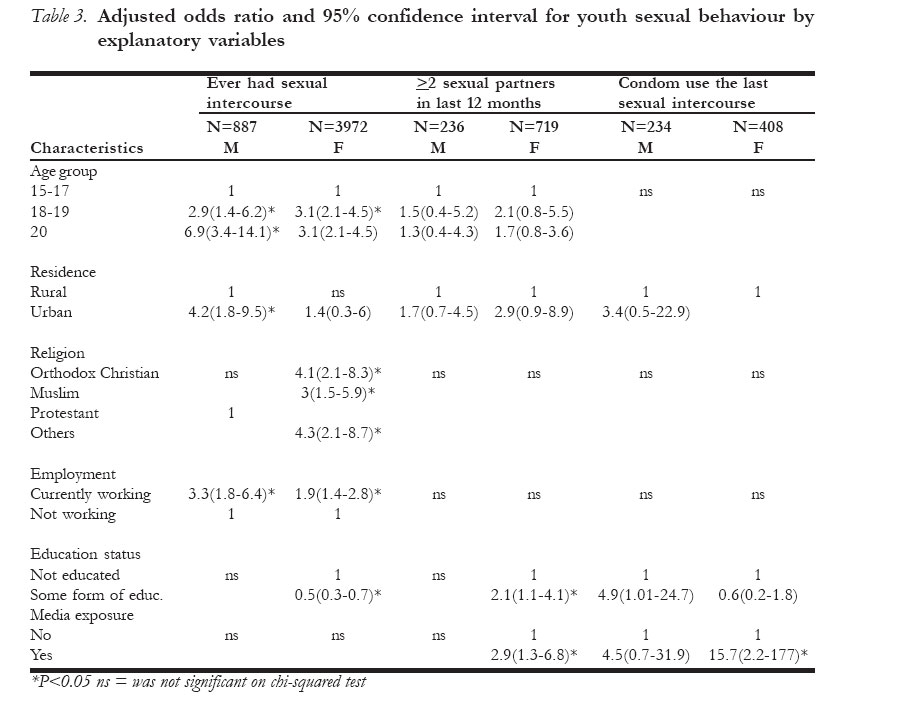
African Journal of Reproductive Health, Vol. 11, No. 1, April, 2007, pp. 14-21 ORIGINAL RESEARCH ARTICLES Sexual Behaviour, Knowledge and Aware-ness of Related Reproductive Health Issues among Single Youth in Ethiopia Wouhabe Maria Wouhabe Maria, MD MSc DLSHTM Good Shepherd hospital P.o.box 2 Siteki Swaziland Code Number: rh07002 Abstract This nationally representative study, encompassing all single youth (15-24 years), was carried out on the subpopulation of Ethiopia DHS 2000 to determine the influences of socio-demographic characteristics on sexual behaviour, and assess the knowledge and awareness of HIV/AIDS and other STIs. There were a total of 890 male and 3,988 female youth. 25.5% of males and 16.1% of females ever had sexual intercourse. Among these, 65.8% males and 24.6% females had two or more sexual partners in the last 12 months. Condom use in the last sexual act was reported by 22.7% and 10% of male and female youth. 19.4% of male and 22.2% of female youth who ever had sexual intercourse ever used family planning method. Although the majority of youth is aware of HIV/AIDS, awareness about other STIs is low. On binary logistic regression analysis, the odds of ever having sexual intercourse were higher for the employed and older youth. Male urban youth was more likely to ever have sexual intercourse than male rural youth (Adjusted OR 4.2; 95% CI 1.8-9.5). Male youth with some form of education were more likely to use condom (Adjusted OR 4.9; 95% CI 1.01-24.7). Female youth with some form of education, the risk of ever having sexual intercourse was reduced by 50% but they were more likely to report having ³ 2 sexual partners in the last 12 months (Adjusted OR 2.1; 95% CI 1.1-4.1). Female youth who had media exposure were more likely to report having ³ 2 sexual partners in the last 12 months (Adjusted OR 2.9; 95% CI 1.3-6.8) but more likely to use condom during last sexual intercourse (Adjusted OR 15.7; 95% CI 2.2-117). Among single Ethiopian youth the overall sexual activity is relatively lower than reported from other African countries but high risk sexual behaviour is common. Socio-demographic factors influence youth sexual behaviour. Résumé Comportement sexuel, connaissance et conscience des questions liées à la santé de reproduction parmi la jeunesse en Ethiopie Cette étude qui est représentative sur le plan national et qui concerne tous les jeunes célibataires (15 - 24 ans) a été menée au sein de la sous-population de l'Ethiopie DHS 2000, pour déterminer les influences des caractéristiques socio-démographiques sur le comportement sexuel et pour évaluer la connaissance et la conscience du VIH/SIDA et les autres ISTs. Il y avait au total 890 mâles et 3,988 femelles - tous des jeunes. 19, 4% des mâles et 22,2% parmi eux qui ont jamais eu des rapports sexuels ont jamais utilisé la méthode de la planification familiale. Quoique la majorité de la jeunesse soient conscientes du VIH/SIDA, la conscience par rapport aux autres ISTs est faible. D'après l'analyse de la regression logistique binaire, la possibilité de jamais avoir un rapport sexuel était plus élevée chez les jeunes employés et plus âgés. Les jeunes mâles qui habitent dans les régions urbainés ont plus la possibilité d'avoir des rapports sexuels que les jeunes mâles qui habitent dans les régions rurales (OR 4, 2; 95% C1 1, 8-9, 5 ajusté). Les jeunes mâles qui ont un certain niveau d'instruction ont plus la possibilité de se server du préservatif (OR 4, 9; 95% C11, 01-24, 7 ajusté). Les jeunes femelles qui ont un certain niveau d'instruction, le risque de jamais avoir eu des rapports sexuels a été réduit de 50%, mais elles avaient plus la possibilité de signaler avoir eu > 2 partenaires sexuels au cours des douze derniers mois (OR 2, 1; 95% C1 1, 3 - 6, 8 ajusté) mais elles avaient plus la possibilité d'utiliser les préservatifs au cours de l'acte sexuel (OR 15, 7; 95% C12, 2 - 117 ajusté). Le niveau de l'activité sexuelle chez les jeunes célibataires éthiopiens est relativement inférieur à celui qui a été signalé dans d'autres pays africains, mais le comportement sexuel de haut risque est commun. Key Words:Knowledge and awareness of related reproductive health issues Introduction The sexual and reproductive health issues of young people are of international and national concern as a result of HIV/AIDS pandemic, growing rates of other sexually transmitted infections and complications of early, unplanned or unwanted pregnancy. The issues also have demographic and social dimension. The demographic dimension is that close to 30% of the world's population is in the age range of 10-24. The population size in this age group is increasing, particularly in the developing world, significantly contributing to the global population momentum as a result of early sexual activity, union and child bearing(1, 2).The social dimension is that reproductive ill health or untimely reproductive outcomes have dire consequence on the life of young people, especially for their future, their offspring and the society they live in(3). Studies from Sub-Saharan African countries, many of which are predominantly school based, show high prevalence rates of sexual intercourse; infrequent use of condoms and other contracep-tives; high prevalence of two or more lifetime sexual partners among young people(4). Information on Ethiopian single youth is relatively limited and those already available are predominantly school based. This study was conducted to determine the extent of sexual activity, knowledge and awareness of HIV/AIDS and other STIs and to examine the influences of socio-demographic factors on sexual behaviour of single youth in Ethiopia. Methods The dataset for the study was obtained from the Ethiopian DHS-2000, which was a nationally representative survey that used standardized questionnaire administered to a sample of 15, 367 women in the age range of 15-49 years and 2, 607 men in the age range of 15-59 years. The specific details and methodology of the survey can be found elsewhere(5). For the purpose of the study, a subpopulation of males and females in the age range of 15-24 years constituting youth were selected. Age, educational status, residence, religion, employment status and exposure to media were explanatory variables. History s of ever having sexual intercourse, the number of sexual partners in the last 12 months during the survey and condom use during last sexual intercourse were outcome variables. The conceptual framework for the assumed interplay between explanatory and outcome variables is shown in figure 1. Data were cleaned, examined for consistency and outcome variables were dichotomously recoded for logistic regression analysis. The cells for explanatory variables education level and media exposure which had multiple categories in the original data set were collapsed into two cell categories to improve analysis power. Univariate analysis was done using chi-squared test to identify association between explanatory and outcome variables followed by logistic regression analysis to control for confounding and estimate odds ratio. Proportion, mean, odds ratio and confidence interval are used for presenting and interpreting data. An association with P-value of <0.05 or confidence interval not containing one was considered statistically significant. Results The general characteristic of the study population is provided in table 1. There were a total of 890 male and 3, 988 female youth. The majority were under the age of 20 years and rural residents. Female youth were more likely to be illiterate (55.4%) than male youth (39%). Orthodox Christian and Muslim, which are the main religions in the country, were the predominant religions. Fourteen percent of females and 4% of males were formerly married. A significant number of male youth had access to radio (61.9%); few had access to magazine (26.3%) and television (31.2%). Compared to male youth, less number of female youth had access to radio (42.4%), magazine (22.3%) and television (20.1%). Table 2 shows the percentage distribution of youth by sexual behaviour, knowledge and practice of selected reproductive health issues. Only 25% of male youth and 16% of female youth ever had sexual intercourse. Comparison of the mean age at first sexual intercourse showed that female youth are sexually initiated at earlier age (15.7years) than male youth (16.5years). Once sexually initiated, a high proportion of male youth (65.8%) and significant proportion of female youth (24.6%) report two or more sexual partners in the previous 12 months. The proportion of youth using condom during the most recent sexual intercourse was low. Only 22.7% of male youth and 10.4% of female youth with a history of ever having sexual intercourse used condom during the last sexual act (table 2). 31.3% of male youth and 21.2% of female youth who reported two or more sexual partners in the last 12 months used condom during the last sexual act. Information on awareness of family planning methods was available for both who had and had not sexual intercourse. 76.3% of male youth and 68.7% of the female youth were aware of some form of family planning methods (table 2). The proportion of youth ever having sexual intercourse who are currently using any method was 12.3% for males and 9.3% for females. For those currently using any method, the methods used by male youth were condom 82.7%, pills 9.2%, periodic abstinence 4.6% and injectable contraceptives 3.5% (pills and injectable contraceptives used by their female partners). The methods used by female youth were condom 34.5%, pills 27.2%, periodic abstinence 18.8%, injectable contraceptives 16.7% and withdrawal 2.8%. The majority of the study participants said they were aware of AIDS and they know how to avoid AIDS (table 2). Being faithful to a single partner, condom use and abstinence which are the often promoted methods of HIV prevention were mentioned as ways of avoiding HIV infection by 58.9%, 47% and 24.3% of male youth respectively and 45.6%, 24.8% and 12.3% of female youth respectively. Knowledge of other ways of avoiding HIV infection was generally low. For example, only 16.7% of female youth and 15.6% of male youth thought avoiding injections will prevent AIDS. 2% of both sexes believed avoiding a partner who has many sexual partners was a way of avoiding AIDS. 14% of males and 6% females believed avoiding sex with commercial sex workers was a way of avoiding AIDS. 29% of the male and 54% of the female respondents stated that a healthy looking person can have HIV infection (figures do not add to 100% due to multiple responses). Awareness of STIs other than AIDS and man's and woman's symptom of STIs is low for both sexes. While girls are aware of man's and woman's symptom of STIs almost comparably, boys report more awareness to man's symptom of STIs (table 2). Table 3 shows the results of binary logistics regression analysis of explanatory variables associated with ever having sexual intercourse, two or more sexual partners in the pervious 12 months and condom use in last sexual intercourse. Compared to male youth in the age range of 15-17years, the odds of ever having sexual intercourse were three times higher for male youth in the age group 18-19 years and seven times higher for those in the age range of 20 years or over. Urban dwellers and currently employed male youth were more likely to ever have sexual intercourse. For females, increasing age, current employment status, religion, and education status were significantly associated with ever having sexual intercourse. Compared to Protestants, girls in the other religious affiliation were more likely to ever have sexual intercourse. Employed girls were also more likely to have sexual intercourse than unemployed ones. For female youth, education was associated with 50% reduction in ever having sexual intercourse. Female youth who had some form of education or exposed to mass media were more than twice likely to report having two or more sexual partners in the last 12 months. The variables that remained significantly associated with condom use during last sexual act were having some form of education for males and exposure to media for females. Discussion Compared to other African studies, the propor-tion of single youth ever having sexual intercourse in this study is low (6, 7, 8). This could be due to that the majority of male youth in Ethiopia begin sexual debut later than other African countries and female youth are sexually active usually under marriage(5, 9). However, Ethiopia is a multi ethnic country and sexual behaviour is influenced by culture, the proportion of sexually active youth is likely to vary by region or ethnic grouping. There for this finding may not reflect the truth at grassroots level. Since Demographic Health Survey uses highly structured data collection tool, social desirability bias can not be eliminated because in typical Ethiopian context sexual activity at younger age is not socially acceptable. As would be expected, the heterogeneity of sexual activity among youth was reflected in this study. More males, older, urban and employed youth ever had sexual intercourse. Girls who had some form of education and protestant Christian in faith were less likely to be sexually active (table 3). Analysis of DHS data on youth form Sub-Saharan countries showed that education increases the age of sexual debut among girls, but reduces among males(10). 65.8% of male and 24.6% of female youth who ever had sexual intercourse had two or more sexual partners in the last 12 months, which is high but comparable with one recent school based urban study from this country that found out 47% of males and 35% of females in the age range of 14-26 had multiple sexual partners(11). Studies form other developing countries also indicate the proportion of youth involved in multiple sexual partnership ranges form 25-69% for males and 15-36% for females(12). More females with some form of education and media exposure had two or more sexual partners in the last 12 months. This is not unexpected as education, urbanization and media exposure are proximate to modernization that heralds liberalization of social sanctions on sexuality(10). The proportion of female and male youth who ever had sexual intercourse using condom in the last sexual act was 10.4% and 22.7% respectively. The proportion of youth with two or more sexual partners in the last 12 months who used condom was 31.3% for male youth and 21.2% for female youth. These figures are low compared to other studies and the HIV epidemic the country is facing(13, 14). On logistic regression analysis, male youth with some form of education were more likely to use condom than those with no form of education. Similarly, female youth who had some form of media exposure were more likely to use condom. Evidence corroborating an association between education and condom use has been reported by other workers too(8). It is important to note that in this study more male youth were educated than female, as a result of which media probably contributes more significantly to female condom use than education. The extent of contraceptive method awareness in this study is similar to figures reported by other investigators form the country(15, 16). But, compared to reports form other African countries, which show figures of as high as 99.2%, this is low (17). The proportion of youth that use contraceptives varies enormously from country to country by gender, type of method, and the reason for use. Figures reported for the developing countries range from 8% to 50% (12, 16). The results in this study are low which is not unexpected as the contraceptive prevalence in the country is one of the lowest in the world and there are few youth friendly services addressing contraceptive needs. Condom is the most common form of method used, which is popularized as a result of HIV/AIDS prevention campaigns(10). As reported in other studies, traditional methods that have less effectiveness, such as periodic abstinence and withdrawal are also used (12). The proportion of youth who report awareness of AIDS and ways of avoiding is high which is similar to findings by other workers(13, 15). The majority of youth answered becoming faithful to a single partner followed by condom use as way avoiding AIDS. This reflects the often promoted probably unbalanced HIV/AIDS prevention information promoted to youth(10). A significant proportion of youth gave inappropriate answers to ways of avoiding AIDS, which indicates the depth of knowledge is inadequate. Awareness of STIs other than AIDS is low. One rural school based study in the country also showed a similarly low figure(13). Public education about STIs and their symptoms in Ethiopia is unpopular and available information mainly focuses on HIV/AIDS. Personal experience and socio-cultural factors likely play a role on the extent of the awareness reported. Other African studies have recorded better specific knowledge and awareness (17). Woman's symptoms of STIs are less well known than man's symptom. In conclusion, the study shows that Ethiopian youth exhibit high risk sexual behaviour evidenced by the high proportion of multiple sexual partners, low condom use rate, and less reliable and infrequent use of contraceptive methods. Sexual behaviour of youth varies by socio-demographic features. Similar to many other studies, awareness of AIDS is high but this has not translated into better depth of knowledge. Awareness of STIs other than AIDS and their symptoms which may vary depending on personal experience and socio-cultural factors is low, reflecting the inadequacy of information available. The findings have implication on the distribution of reproductive health services for youth. Acknowledgments This project was completed while the investigator was recipient of WHO research training grant (Department of RHR/HRP) for which I am heavily indebted. I would like to thank Professor Cleland Johns for supervision while conducting the work and Emma Slaymaker for help during data analysis. The data set used in this work comes form Ethiopia DHS 2000 originally collected by Central Statistical Authority, Ethiopia and ORC MACRO, Calverton Maryland. They are duly acknowledged. References
© Copyright 2007 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh07002t2.jpg] [rh07002t3.jpg] [rh07002f1.jpg] [rh07002t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}