 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
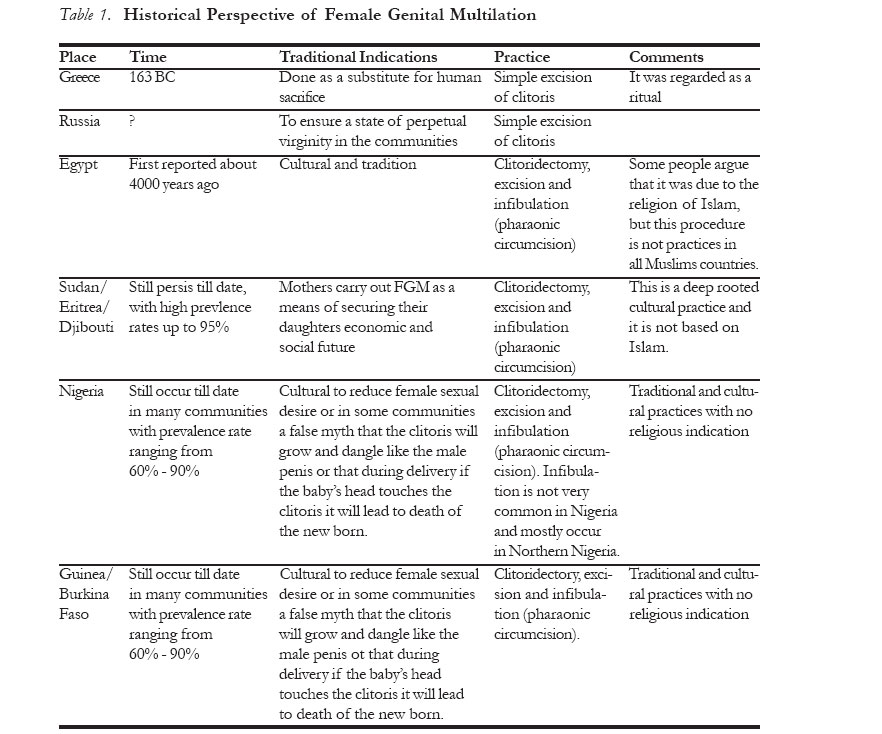
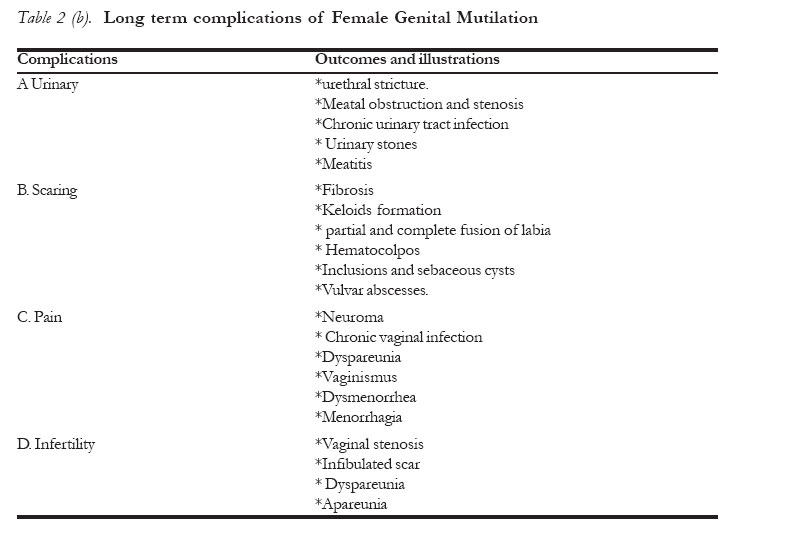
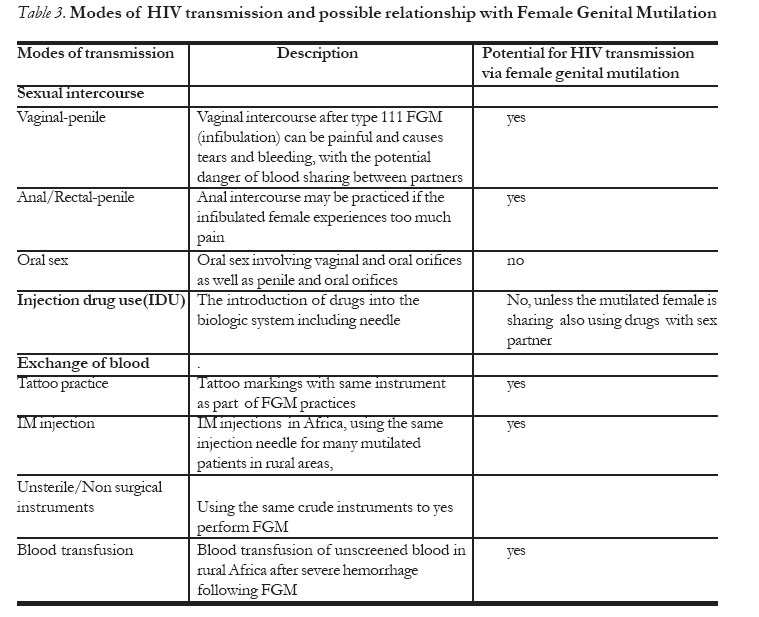
African Journal of Reproductive Health, Vol. 11, No. 1, April, 2007, pp. 33-42 Female Genital Mutilation: Potential for HIV Transmission in sub-Saharan Africa and Prospect for Epidemiologic Investigation and Intervention Emmanuel Monjok,MD,MPH 1, E.James Essien,MD,DrPH 1, 2, Laurens Holmes, Jr,MD,DrPH 1, 2 1 Institute of Community Health, University of Houston, Texas Medical center, Houston, TX 77030, USA, Code Number: rh07004 Abstract Female Genital Mutilation (FGM) which involves alteration of the female genitalia for non-medical grounds is prevalent in Sub-Saharan Africa, associated with long- term genitourinary complications, and possible HIV transmission. This mini-review aims to examine FGM and the possibility of HIV transmission through this procedure. We performed an electronic search using Medline for articles published between 1966 to 2006 for evidence of FGM practice, its complications, and the nexus between this procedure and HIV sero-positivity. The results indicate ongoing FGM practice, albeit prevalence reduction, due probably to the increasing knowledge of the consequences of FGM as a result of non-sterile techniques. Secondly, the complications of FGM are well established which include Genitourinary disorders. Further, while data is limited on HIV transmission via FGM, there is biologic plausibility in suggesting that FGM may be associated with increasing prevalence of HIV in sub-Saharan Africa. This paper recommends further studies in order to assess the association between FGM and HIV transmission. Résumé Mutilation génitale féminine: Potentiel pour la transmission du VIH en Afrique subsaharienne et la perspective pour l'enquête et l'intervention épidémiologiques La mutilation génitale féminine (MGF) qui implique la modification des organes génitaux féminins pour des raisons non médicales est répandue en Afrique subsaharienne et elle est liée aux complications génitaux-urinaires à long terme et peut-être à la transmission du VIH. Cette mini-étude a pour objectif d'examiner la MGF et la possilibité de la transmission du VIH par cette procédure. Nous avons recherché sur l'internet à l'aide de la medline des articles publiés entre 1966 et 2006 pour l'évidence de la pratique de la MGF, ses complications et la liaison entre cette procedure et la séropositivité du VIH. Les résultats montrent que la pratique de la MGFse poursuit bien que la prévalence soit réduite dû probablement à la croissance de la connaissance des conséquences de la MGF à cause des conséquences non-stériles. Deuxièment, les complications de la MGF sont bien établies y compris les troubles génitaux-urinaires. De plus, alors que les données sont limitées par rapport à la transmission du VIH par la MGF, il y a une plausibilité biologique de suggérer que la MGF peut être liée à la prévalence croissante du VIH en Afrique subsaharienne. L'article préconise encore d'études pour permettre d'évaluer le lien entre la MGF et la transmission du VIH. Key Words: Female genital mutilation, HIV transmission, sub-Saharan Africa, HIV risk factors Introduction Female Genital Mutilation (FGM) is a term used to describe traditional practices that involve the cutting of female genitalia. Other commonly used terms for this procedure are female circumcision, female genital cutting or female genital surgeries. FGM persist in sub-Saharan Africa with the practice still associated with non-sterile techniques and multiple complications, including though not limited to, hematological, urologic, hemodynamic, infections and psychosocial morbidities. Further, there is a possibility that this practice may be associated with increased transmission of HIV infection in sub-Saharan populations. There are multiple and diversified conno-tations of FGM. The World Health Organization (WHO) describes FGM as the intentional removal of part or all of the external genitalia, or other damages to the female genitalia for cultural or other non-therapeutic purposes.1 In sub-Saharan Africa this practice involves use of shared and crude instruments; thus the sharing of blood. 2 The genital trauma caused by FGM and the consequences, according to the WHO,3 may increase the susceptibility to HIV infection. Secondly, herbs and foreign bodies inserted into the vagina by traditional methods may increase the possibility of HIV transmission, due to inflammation and abrasions to the vaginal epithelium. Female genital mutilation is practiced in 28 countries of sub-Saharan Africa; a few countries in the Middle East and Asia, and among immigrant populations from these countries in Europe, North America and Australasia. It has been estimated that there are over 120 million girls and women worldwide that have undergone this procedure, and at least 2 million girls are at risk of being genitally mutilated each year, at about 6000 girls per day.4 - 6 Eighteen African countries have prevalence rates of 50% or higher. The highest prevalence is in Somalia and Djibouti (98%), but these estimates vary from country to country and within various ethnic groups.1 In spite of the known complications and the potential for HIV transmission through FGM, there are very limited studies reviewing this practice currently and presenting perspective on the probability of FGM leading to HIV transmission. Biologically, any sexually-related viral or bacterial pathogen has increased propensity for transmission, given trauma or pre-existing laceration to the vaginal epithelium. FGM increases the risk of vaginal epithelial damage and consequently increase the probability of HIV transmission. This mini-review paper aimed to explore the historical perspective of FGM, delving into its description, patterns of practice, and the possibility or likelihood of FGM as a non-sterile technique of mutilation, resulting in HIV transmission. This paper, if anything, may provoke thought process on the probability of increased HIV transmission, given FGM, thus encouraging hypothesis generation and testing on the association between FGM and HIV transmission. MATERIALS AND METHODS Electronic search of published literature was conducted using Medline with the key words: female genital mutilation, female genital cutting, female circumcision, and health complications as well as female genital mutilation, female genital cutting, female circumcision and HIV. The search was restricted to English language articles only. We searched all original articles that were published between 1966 to 2006 on FGM (k=789). The search for the later resulted in the selection of five (5) eligible articles ( 25-27, 29, 30) whereas the former resulted in seven (7) eligible articles (10, 15-18, 21-23). As part of the exclusion criteria, we included only the most comprehensive articles from author/s if two (2) or more articles were published on the same study population in different years. Also, we excluded articles that provided abstracts only. Apart from the historical perspective, only original articles that addressed FGM in sub-Saharan Africa were included in this study. QUALITATIVE SYNTHESES (RESULTS) Notion and Classification of FGM Female Genital Mutilation has been in practice for some 4000 years and continues to be prevalent in most parts of the world, especially in sub-Saharan Africa (Table 1). FGM typically involves the alteration of the female genitalia using a traditional pattern of resection that is charac-terized by non-sterile technique. The World Health Organization (WHO) has classified FGM into four types,7 in order to strengthen policy formulation including legislation, research and training. According to WHO classification matrix, FGM taxonomy includes: Type I - the partial or total removal of the clitoris, Type II - partial or total removal of the clitoris together with partial or total excision of the labia minora, Type III - partial or total removal of the external genitalia and stitching or narrowing of the vaginal orifice and Type 1V - traditional genital surgeries such as pricking or stretching the clitoris and/or surrounding tissues, cauterization by burning of the clitoris and surrounding tissues, introcision, scraping of the vaginal orifice, cuts into the vagina and introduction of substances into the vagina with the aim of tightening or narrowing the vagina. Whereas, there are other taxonomies of FGM, which are not delved into in this paper due to complexities, type III (sometimes known as Pharaonic circumcision or infibulation) is the most severe and accounts for 15% of all genital cuttings,7 while 85% of the cuttings are type I and II,7 and type II being the commonest. With respect to geographic locale, Type III operations occur predominantly in Somalia, northern Sudan and Djibouti, although it has been reported in parts of Ethiopia, Eritrea, northern Kenya, Mali and northern Nigeria. Practice and Resection techniques Female Genital Mutilation which is still practiced in sub-Saharan Africa and elsewhere in the world has been explicitly and unequivocally condemned by the WHO as an unacceptable medical practice and as such should not be practiced by health professionals in any setting.8 The WHO study group on FGM and obstetric outcome results indicated that women with FGM are significantly more likely than those without FGM to develop unwanted obstetric outcomes, with the risk of adverse events greater with type 111 FGM.9 Further, the International Federation of Gynecology and Obstetric (FIGO) supports the WHO stance on medicalization of FGM.10 Female Genital Mutilation, to our knowledge is not a standard surgical procedure in western Medicine, with the practitioners of this "surgical procedure" commonly identified as perpetrators. FGM is usually carried out by traditional practitioners or lay persons, usually older women, using crude instruments and without any anesthesia. The crude instruments range from a scalpel to a piece of glass and are conducted in unhygienic and unsterile conditions. 11 In spite of the non-involvement of western medical practitioners, historically trained medical personnel including doctors and nurses occasionally connive at and encourage FGM. Further, it has been suggested that about 12% of FGMs are carried out by physicians.12 The age at which FGM is practiced varies by locale. Amongst the nomads of Sudan it is performed at a few days old, while in Egypt and in countries of East Africa and the Horn of Africa, it is performed at about the age of 7 years. In addition, in some communities, FGM is performed in adolescence while other communities prefer to carry out the procedure shortly before marriage, e.g. the Ibo tribe in Nigeria.13 Rationale for practice A variety of reasons (sociocultural, religious, psychosexual, hygienic and esthetic) have been suggested for the continuation of FGM in the locale where this procedure persist. These reasons include marriageability, curbing sexual desire, protecting virginity, religious rite, initiation to womanhood, improved hygiene, and beautification.14 In some communities in Eastern Nigeria, it is believed that if the head of the neonate touches the clitoris during child birth, the neonate will not survive.13 Further and of health significance, FGM has a deep-rooted cultural importance that some communities have allowed the medicalization of the procedure to minimize the health consequences associated with the traditional procedure.10, 15 Regardless of this rationale, the WHO very firmly disapproves this procedure because it tends to perpetuate and promote FGM rather than to prevent or reduce its practice.10. Health and social Complications Female Genital Mutilation has been observed to decrease in prevalence in a number of countries despite no well defined interventions to reduce or eliminate this practice,15 due probably to the numerous complications and the potentials for viral infections, namely HIV. The complications of FGM are immediate and long-term, including medical, psychosexual and psychosocial. Severe gynecological and obstetrics complications, of FGM especially with the Type III or Infibulation have been observed.9,16-18 Table 2a and 2b demonstrate acute and chronic complications of FGM respectively.19 FGM has been associated with psychological trauma including post traumatic stress and chronic behavioral ailments such as generalized anxiety, unipolar affective disorder, chronic irritability, frigidity and marital conflicts.20 Specific health and social complications of FGM has been observed to vary with the type of FGM. Circumcised women have been noted to have higher risk of tearing and still births compared with uncircumcised.21, 22 A study of 1836 cohort of healthy premenopausal Nigerian women found a statistically significant increase in lower abdominal pain, malodorous vaginal discharge and genital ulcers among those with FGM compared to those without.23 FGM and Association with HIV Transmission HIV/AIDS epidemic The latest AIDS epidemic update in sub-Saharan Africa shows that about 2.58 million people are living with HIV, which represent 64% of the world's HIV cases with 3.2 million new cases and 2.4 million deaths.24 It is therefore obvious that more than 60% of all people with HIV live in sub-Saharan Africa.24 There is little evidence of a declining epidemic in this region despite decline in HIV prevalence in many other countries. Prevalence levels remain "exceptionally" high and might not have reached their peak in several countries. Women are disproportionately affected by HIV and most still remain poorly informed. HIV modes of transmission The various modes of transmission of HIV and their possible association or enhancement through FGM procedure is shown in Table 3. These modes include sexual intercourse, which may be vaginal/penile, anal/penile, or oral sex, injection drug use and the sharing of needles and the exchange of blood products during non-sterile female genital mutilation. Unscreened blood transfusions still occur in some rural hospitals in sub-Saharan Africa, with its dangers of trans-mission of HIV and Hepatitis. HIV transmission and FGM HIV transmission from this FGM practice is enhanced through shared instruments and blood products during the practice of genital cutting as well as damage to the vaginal epithelium associated with the trauma, inflammation and complications. Other modes of HIV trans-mission, as well as other HIV risk factors may occur in association with this practice, making it difficult to ascertain whether FGM is the sole predisposing risk factor, as well as a contributing variable to the cumulative incidence of HIV in sub-Saharan Africa. Similarly, if approximately 6000 young girls undergo FGM daily and about 2 million young girls are at risk of being genitally mutilated in a year, the odds of FGM as a risk factor to HIV transmission remains to be assessed. A recent article,25 revealed the transmission of HIV to girls who have non-perforated hymen (virgins) and that 97% of the time, the same instrument could be used on 15-20 girls.26 This data suggest the possibility of FGM procedure as a risk variable in HIV transmission. Female Genital Mutilation may predispose women to HIV in many other ways. For example, the increased need for blood transfusions due to hemorrhage either when the procedure is performed, at childbirth, or a result of vaginal tearing during defibulation and intercourse. These tears would tend to make the squamous vaginal epithelium similar in permeability to the columnar mucosa of the rectum, thus facilitating the possibility of HIV transmission.27 In addition, many women with type III (pharaonic) mutilation experience dyspareunia, as well as repeated tissue damage and bleeding. Difficult and painful vaginal intercourse in some of these women eventually lead to anal intercourse with heterosexual partners, further increasing the HIV risk in these women. Thus, it is plausible that HIV transmission may be enhanced by the widespread practice of FGM.27- 30. In spite of this biologic casual plausibility, there are no epidemiologic data associating HIV transmission with FGM. Discussion This mini review paper has a few relevant observations. First, FGM continues to persist among populations in sub-Saharan Africa. Second, the non-sterile technique of this procedure has not been replaced by modern surgical technique. Third, FGM is not a standard surgical procedure in the western medical tradition. Fourth, there exists propensity or probability of HIV infection being transmitted through this practice. Fifth, epidemiologic data are needed to assess the risk of HIV infection, given exposure to FGM. This paper which was based on original articles and other review articles on FGM has shown that in sub-Saharan Africa, countries such as Nigeria, Guinea, Ethiopia, Somalia, Djibouti and Sudan still continue to practice FGM despite a relative reduction in its prevalence. The persis-tence in this practice may be due to cultural beliefs, norms and traditional health beliefs, maintained among these populations. In addition, it is plausible that the practice persist due to financial gains that are associated with its practice.10 The observation of the non-sterile technique in FGM practice is supported by the fact that this procedure has not been accepted as a standard surgical procedure by modern medicine. Further, the expenses involved in sterile procedure may promote the continuous use of non-sterile technique which is less expensive and therefore affordable by the perpetrators. Regarding the acute and chronic complications associated with FGM, it is very unlikely that this practice will ever be accepted as a standard surgical procedure in the western medical tradition Also, the non-acceptability of this practice may be due to the lack of its therapeutic benefits and the life threatening outcome, including septicemia associated with more than 40% mortality rate in sub-Saharan Africa. Human Immunodeficiency Virus trans-mission through FGM is plausible. First, the probability of pathogenic transfer to the blood stream increases with any non-sterile procedure. Second, bleeding or blood loss during this procedure increases exchange of blood and blood contacts which serves as one of the modes of HIV transmission. Third, blood loss during the process may compromise immune respon-siveness thus increasing the probability of HIV sero-conversion. Fourth, the presence of genital lacerations augments the probability of transmission, given sexual contact with an infected individual. The lack of epidemiologic data necessitates further hypothesis generation and testing, commencing with ecologic design, cross-sectional design and case-control studies to assess whether or not FGM increases the risk of HIV transmission. To date, there are a few reported cases, which limit any epidemiological inference on the role of FGM in HIV transmission. Albeit the strength in this paper, there are a few limitations. It is possible that our mini- review is biased since we were not able to guarantee the inclusion of all published papers in this topic. Secondly, the lack of data on original studies, if one existed, on the association between FGM and HIV transmission significantly restricts any possible conclusion that may be drawn from this mini-review, requiring, therefore, a cautious interpretation and application of these obser-vations. Thirdly, our paper might be biased since we were not able to examine studies published in other languages besides English. Despite the above limitations, in summary, we have shown through this mini-review the practice of FGM, its health consequences and the limited data on the nexus between this practice and HIV transmission. In sub-Saharan Africa, while the trend of FGM does not seem to increase, the practice currently persist. The health consequences include reproductive and urinary disorders and septicemia, given the non-sterile technique involved in most of these practices performed outside the medical setting. HIV transmission involves multiple routes, one which includes blood contamination through non-sterile technique and other measures that have potentials for an association with FGM. Though case reports/series are limited in this perspective, there is plausible mechanism to implicate FGM in HIV transmission especially in populations with HIV preponderance such as the sub-Saharan Africa. To assess this postulate, further studies are required to answer the research question as to whether or not FGM increases the chance of HIV transmission. The knowledge of such studies will enhance our cognizance of HIV risk factors and the potential for intervention prevention in sub-Saharan Africa. Acknowledgement The preparation of this manuscript was facilitated by National Institute of Mental Health grant number RO1 MH073361-02. Also, the authors would like to thank Dr. Doriel Ward, Orsolya Garrison, MPH, Jennifer Krueger and Jonathan Brunt for reviewing the final draft of this manuscript. References
© Copyright 2007 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh07004t1.jpg] [rh07004t2b.jpg] [rh07004t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}