 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
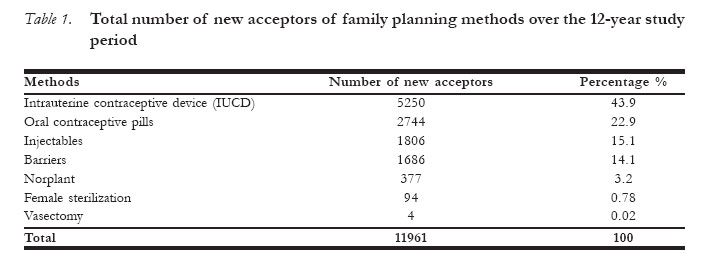
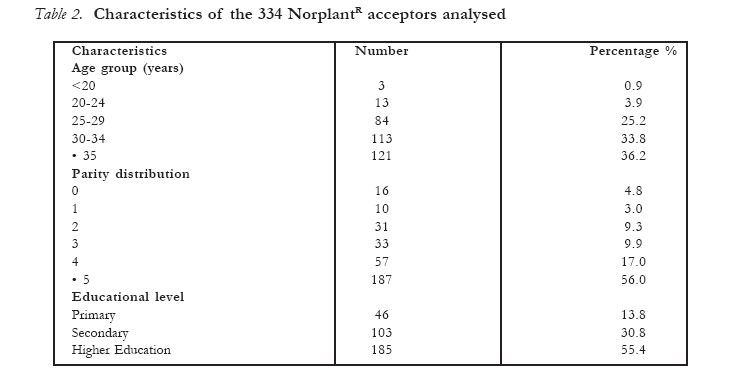
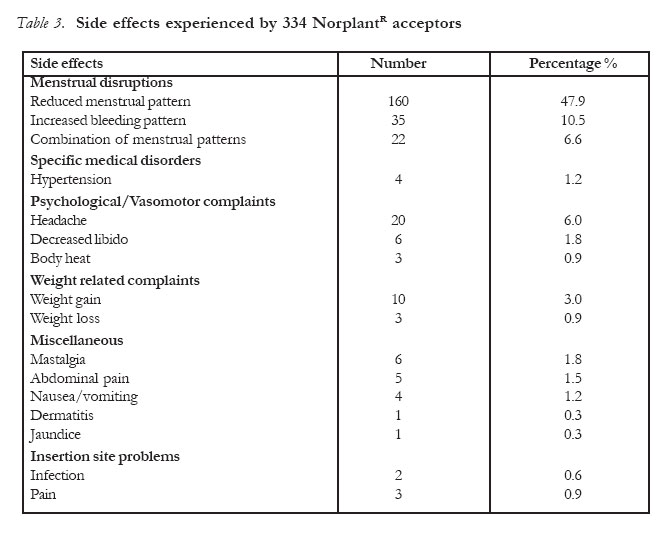
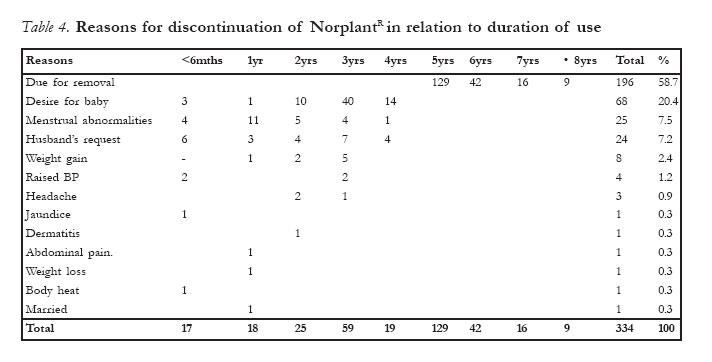
African Journal of Reproductive Health, Vol. 11, No. 1, April, 2007, pp. 90-97 Contraception with Levonorgestrel Subdermal Implants (NorplantR) in Benin-City, Nigeria: A 12-year Review A.O. Aisien NorplantR is the registered trademark of the Population Council for six-capsule subdermal levonorgestrel implants. Code Number: rh07009 Abstract The case notes of 377 clients who accepted Norplant out of 11961 acceptors of family planning methods in the Department of Obstetrics and Gynaecology University of Benin Teaching Hospital, between January 1985 and December 1996 were retrieved and analysed at the end of 2004, for socio-demographic characteristics of the clients, side effects and complications reported and reasons for discontinuation in relation to duration of use. The daily register of the acceptors were analysed for new acceptors of other methods during the same period and confirmed with their case notes. The acceptance incidence of Norplant was 3.2%. The mean age and parity of the acceptors were 32.2 ± 4.5years and 3.9 ± 1.8 respectively. The duration of use ranged between 6 months and 13 years. 65% of the acceptors reported menstrual abnormalities. 48% of them reported reduced bleeding pattern, while 7.5% (25) discontinued method under 4years of use because of increased bleeding episodes. Other side effects reported were headache 6%, weight gain 3%, mastalgia 1.8%, decreased libido 1.8%, abdominal pain 1.5% and hypertension 1.2%. 20.4% (68) discontinued the use under 4years because of desire to have another baby. 38.6% (129) had implants removed at 5years, while 20.1% (67) continued the use for 6-13years before removal and replacement with another set. Husband's request for removal constituted 7.2% (24). The effectiveness was 100% as no pregnancy was reported during the study period. The continuation rate at 5years was 58.7%. 43 clients were however lost to follow up. Norplant was found to be an effective and acceptable method of long-term reversible contraception with minimal side effects. The low incidence was attributed to the fact that the implants were donor driven and not included in the country contraceptive logistic system. Norplant acceptors who continued the use after 5years did so, because they enjoyed it and did not want to part with them without replacement of new sets. Résumé Contraception à l'aide des implants sous-dermiques Levonorgestrel (NorplantR) à Benin-City, Nigéria: Compte rendu convrant une période de douze ans Nous avons récupéré les dossiers des 377 clientes qui ont accepté Norplant parmi les 11961 accepteurs des méthodes de la planification familiale dans le Département d'Obstétrique et Gynécologie du Centre Hospitalier Universitaire de Benin-City (University of Benin Teaching Hospital, Benin - City) entre janvier 1985 et décembre 1996. Les dossiers ont été analysés pour identifier les caractéristiques socio-démographiques des clientes, les effets secondaires et les complications signalées et les raisons pour l'arrêt par rapport à la durée de l'emploi. Le registre quotidien d'accepteurs a été analysé pour identifier les nouveaux accepteurs d'autres méthodes pendant la même période avant de les confirmer avec leurs dossiers. L'incidence de l'acceptation de Norplant était de 3,2%. L'âge moyen et la parité des accepteurs étaient de 32,2 ± 4, 5 ans et 3, 9 ± 1, 8 respectivement. La durée de l'emploi variait entre six mois et 13 ans. 65% des accepteurs ont signalé les anomalies menstruelles. 48% parmi elles ont signalé une habitude d'une hémorragie réduite, alors que 7,5%(25) ont arrêté l'emploi de la méthode en moins de quatre ans à cause des crises d'hémorragie. Autres effets secondaires signalés étaient maux de tête 6%, prise de poids 3%, mastalgie 1,8%, baisse de la libido 1,8%, douleur abdominale 1,5%, hypertension 1,2%. 20,4% (68) ont arrête l'emploi en moins de 4 ans parce qu'elles voulaient avoir encore un enfant. 38,6% (129) ont enlevé les implants au bout de 5 ans, alors que 20,1% (67) ont continué à l'employer pour 6 - 13 ans avant de les enlever et de les remplacer avec un autre jeu. La demande de la part du mari pour l'enlevement a constitué 7,2% (24). L'efficacité était de 100% puisqu'aucune grossesse n'a été signalée au cours de la période de l'étude. Le taux de la continuation à 5 ans était de 58,7%. Toutefois, nous n'avons pas pu bien suivre 43 clientes que nous avons perdus de vue. On a trouvé que Norplant est une méthode de contraception reversible à long terme qui est efficace et acceptable ayant des effets secondaires minimaux. L'incidence réduite était attribuée au fait que les implants dépendent énormément aux donateurs et qu'ils ne sont pas inclus dans le système logistique contraceptif du pays. Les accepteurs de Norplant qui ont prolongé l'emploi après 5 ans l'ont fait parce qu'elles l'aimaient et ne voulaient le laisser tomber sans les remplacements de nouveaux jeux. Key Words: NorplantR, Acceptability, Place amongst Other Family Planning Methods. Introduction Levonorgestrel implants were the first new contraceptive to be made available since 1960s when the oral contraceptive pill was developed and the intrauterine contraceptive devices (IUCD) were rediscovered1. Norplant, a levonorgestrel implant system has been found world to be safe, effective, reversible long-term method of contraception suitable for many women who require them to space or limit child bearing2,3,4,5.6.7.8. Norplant like any other family planning methods is not free from side effects. Its major side effects is menstrual abnormalities which occur in 60%-100% of the women9,10,11. Such bleeding aberrations were mainly responsible for discontinuation in the first year of use12,13,14. Inspite of the bleeding irregularities, increased haemoglobin levels had been documented11,15,16,17,18. This is a beneficial effect in developing countries with high prevalence of anaemia. Other side effects documented which are hormone related include, headache, weight changes, mastalgia and hirsutism8,19,20. Worldwide 11 million women in over 60 countries are using Norplant. Female sterilization by 210 million, intrauterine devices by 156 million and oral contraceptives by 80 million21. The reverse is actually the trend in developing countries were IUCD is most commonly accepted and female sterilization the least accepted. Norplant was introduced into our setting in 1985 by Family Health International as part of the pre-introductory clinical trial. By 1989, it was introduced into clinical setting by AVSC (Association for voluntary Surgical Contraception now ENGENDERHEALTH) overlapping with the clinical trial. Norplant has been in use in our family planning clinic for over 15years. Unfor-tunately its supply has been donor driven and not integrated into the national commodity logistics system hence its continuous supply had been epileptic and depended on donors and their priorities. The study therefore evaluated the safety, efficacy and acceptability of Norplant implant over a 12-year period of use amongst its acceptors in Benin-city. Materials and Methods The case files of the 377 clients who accepted Norplant contraception after counseling between 1985 and December 1996 were retrieved from the family planning clinic record section and analysed retrospectively at the end of 2004 for socio-demograhic characteristics of the acceptors, their side effects and complications, and reasons for discontin-uation in relation to duration of use. The acceptors' registers were also analysed for the acceptors of other family planning methods during the same period. Norplant implants were inserted and removed by trained providers following standard protocols23. The acceptors were followed up at 6weeks, 3months, 6months and subsequently annually. Clients were encouraged to return to the clinic outside revisit date, if complications arose. At each clinic visit history was taken followed by examination. Clients were managed according to assessment. All information was documented in the case note. The clients were always reminded about the benefits, side effects, and duration of use of implants and the need to have them removed at the end of 5years of use. A client was considered lost to follow up if she defaulted for more than 6months following scheduled follow up visit. Results During the study period, there were 11961 new acceptors out of which 377 accepted Norplant giving an incidence of 3.2%. Acceptors of IUCD, oral contraceptive pills, injectables constituted 43.9%, 22.9% and 15.1% respectively (Table 1). 43 Norplant acceptors were lost to follow up and only 334 records were analysed. The age range of the clients was 17-48years with a mean ± SD of 32.2 ± 4.5years. The parity ranged from 0-7 with a mean ± SD of 3.9 ± 1.8 (Table 2). Most of the clients 99.7% (333) were married. They all had formal education (Table 2). 85% of the clients reported side effects out of which 65% reported menstrual abnormalities. Reduced bleeding episode was reported by 47.9% (160) of the clients. 7.5% (25) discontinued the use of method under 4years out of the 10.5% (35) of those who reported increased bleeding patterns. Other side effects reported were headache 6% (20), weight gain 3% (10), mastalgia 1.8% (6), decreased libido 1.8% (6) and abdominal pain 1.5% (5) (Table 3). 20.4% (68) of the clients discontinued the use of implants under 4years because of their desire to have another baby. At 5years of use, 38.6% (129) had their implants removed. However 20.1% (67) kept implant beyond 5years and subsequently removed them at various time between 6-13years. The reason given was that they were satisfied with the method and held on to them because they could not get replacement of new sets of the capsules. Discontinuation following husband objection accounted for 7.2%. Eight clients (2.4%) had implants removed under 3years because of weight gain (Table 4). Discussion Our study had shown that the incidence of Norplant amongst other contraceptive methods over the 12 years study period was 3.2%. The incidence was rather low when compared with incidences in other studies3,24,25,26,27,28,29. The reduce incidence was attributed to the fact that Norplant supply was donor driven and not integrated into the country's contraceptive logistics system with full access and continuity of supply like other methods. The most popular contraceptive method of choice was IUCD which required the least motivation30. Other authors24,27,28,29 had also documented similar findings. The least accepted method was female sterilization with an incidence of 0.8%. This had been similarly reported24,29. The reverse is the trend in developed countries where the most popular method is female sterilization followed by the IUCD and oral contraceptive pills. Many women who should be considering permanent method are still using reversible methods of contraception out of fear of: reincarnation without fallopian tubes, death of husband and operation31.Some of the reasons that have also been advanced for the high parity before tubal ligation included uncertainty of survival of children in view of the high perinatal and infant mortality in Nigeria32, security in marriage, and the need to have a full complement of both genders33. The mean age and parity of the clients were similar to those found in previous studies in Nigeria3,22,24 and elsewhere34. Many of the acceptors were over 30years and grandmul-tiparous, but were unwilling to have sterilisation. Some other studies however documented lower age and parity distributions26,35,36 ; especially in women using the method to space child bearing. The major side effect of Norplant was bleeding irregularities which was reported by 65% of the acceptors and accounted for 7.5% discontinuation in the first 4years of use. In clinical studies 40-60% of users discontinued the use of Norplant implants in the first year of use37,38. Our previous studies17,18, had reported irregular reduced bleeding pattern amongst the acceptors over 36months of use. After the insertion of the six capsules, levonorgestrel is slowly released through the polydimethysiloxane tubing at a rate of 85µg/day at first. Within about 18months, the concentration of the progestin in plasma stabilizes at an average of 30µg/day giving a plasma concentration of 0.30nanogram/milliliter which is maintained for about 5years2. Levonorgestrel concentrations among women show considerable variation depending on the individual clearance rates, body weight and possibly other factors8. The release rate may account for the irregular menstrual pattern observed in Norplant users. Inspite of the abnormalities in menstrual flow, the volume of blood loss either does not change or decrease in amount16,39. The packed cell volume had been found to increase significantly2,15,16,17,18, a change that may prevent anaemia in the users. Other side effects reported in the study were headache, weight gain, decreased libido, hypertension, nausea and vomiting, mastalgia. These are method related and had also been documented in the literature8,20,21,40. 1.2% and 2.4% of the clients discontinued the use of the method under 3years because of elevated blood pressure and weight gain respectively. Sodium and water retention could occur as a result of progestogen contraceptive method and this could account for the increase in blood pressure. About 30% of Norplant users have reported changes in body weight. In many, the weight gain was associated with an increase in appetite after insertion of the implants41. In addition longitudinal studies of bone mineral density of the lumbar spine and distal forearm have shown an increase at 1 and 2 years after insertion of Norplant in adolescents and women ages 20-4542,43. Levonorgestrel is a derivative of 19 nortesto-sterone whose action is androgenic and anti-estrogenic. The weight gain may also be a consequence of the anabolic effect of progestogen in the body. Husband's objection to continuous use of the method caused discontinuation in 7.2% (24) of the clients. This has also been reported27, 44,45, but could be minimized by having male involvement in their partner's contraceptive choices at counseling sessions. Infection complication in the series was minimal at 0.6%. and within the range of 1.6% reported19. This was because strict infection prevention practices were observed and trained service providers inserted and removed implants. Serious insertion site infection however could occur and lead to hospitalisation46. 20.4% (68) of the clients discontinued the use of the method under 4years. These were the younger women with low parity who used the method for spacing. 38.6% (129) had the implants removed at five years. However 20% (67) did not turn up for removal until between 6-13years of use. The reason given for not coming for removal was that new sets of implants were not available for replacement and they were satisfied with the old sets inserted. These were the older multiparous clients who did not want to have more children, but were unwilling to have sterilization. The effectiveness of Norplant was 100% as no pregnancy was reported. In clinical studies the average annual pregnancy rate over a 5year period was 1%8. The continuation rate at the end of 5years was 58.7% which was within the range of 33%-78% reported in studies11. 43 (11.4%) clients were lost to follow up. It can be presumed that these clients were satisfied with the method that is why they are still continuing with it. In conclusion the retrospective study had shown that Norplant was safe and effective amongst the women. The low incidence of acceptance had to do with supply as it is donor driven which could be corrected by including implants in the country's contraceptive logistic system in order to continue to uphold the rights of clients to access and continuity in services. The side effects and benefits of Norplant docu-mented should form part of the information given to clients to make informed decision. The unit will need to trace the defaulters since their addresses were documented in their case files. References
© Copyright 2007 - Women's Health and Action Research Centre
The following images related to this document are available:Photo images[rh07009t1.jpg] [rh07009t3.jpg] [rh07009t2.jpg] [rh07009t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}