 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
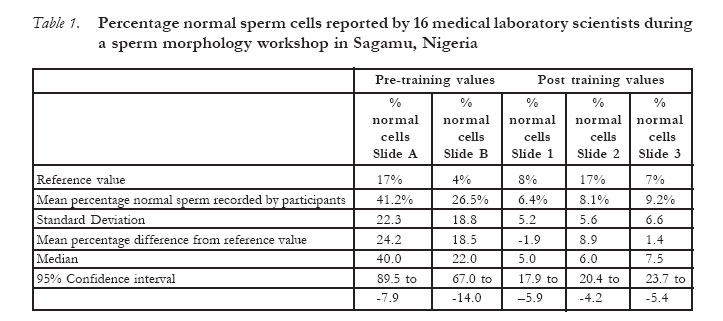
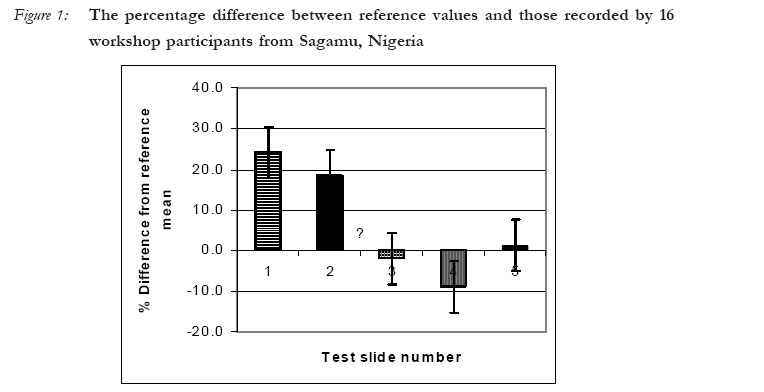
African Journal of Reproductive Health, Vol. 11, No. 1, April, 2007, pp. 107-112 Does Training Assist Medical Laboratory Scientists with Better Evaluation of Sperm Morphology? DR Franken1, PhD OA Dada2, PhD 1Department of Obstetrics & Gynaecology, Tygerberg Hospital, University of Stellenbosch, Tygerberg 7505 Cape Town, South Africa 2Centre for Research in Reproductive Health, Olabisi Onabanjo University, Sagamu, Nigeria. Code Number: rh07011 Abstract This study aimed to evaluate the quality of sperm morphology evaluation skills of 16 technologists who are responsible for semen analyses in their institution. The 1-day workshop was held at the Centre for Research in Reproductive Health in Sagamu, Nigeria. Participants were requested to complete a questionnaire that provided information regarding their experience and training as technologists in their institution. The workshop consisted of 4 sections, namely (i) pre-training test, (ii) lectures on morphometric characteristics and details of normal and abnormal sperm (iii) a laboratory-based hands-on, post training test and (iv) a consensus training session. The findings of the questionnaire indicated that none of the participants had any previous formal training and that all participants had very little knowledge about the morphological appearance of normal spermatozoa. These findings were supported by the results obtained during the pre-training session that showed a mean percentage difference of 24% between the reference and participant's values. These somewhat alarming results highlight the need for training facilities for technologists who work in the clinical diagnostic field of reproductive science. Résumé Est-ce que la formation aide les scientifiques de laboratoire médical à mieux évaluer la morphologie du sperme? Cette étude avait pour objectif d'évaluer la qualité de la compétence de l'évaluation de la morphologie du sperme chez 16 technologues chargés de l'analyse de la semence dans leur établissement. L'atelier qui a duré un jour a eu lieu dans le Centre de la Recherche sur la Santé de reproduction à Sagamu, Nigéria. On a demandé aux participants de remplir un questionnaire qui contenait des renseignements concernant leur expérience et leur formation en tant que technologues dans leurs établissement. L'atélier comprenait 4 sections à savoir (i) le test d'avant stage (iv) les cours sur les caractéristiques morphométriques et les détails du sperme normal et anormal (iii) un test basé sur le laboratoire, le test d'après-stage (iv) une séance de stage de consensus. Les constats des questionnaires ont montré qu'aucun participant n'avait une formation formelle préalable et que tous les participants n'avaient qu'une faible connaissance de l'apparence morphologique des spermatozoïdes normaux. Ces constats ont été appuyés par les résultats obtenus pendant la séance de l'avant stage qui ont montré une différence dans le pourcentage moyen de 24% entre les valeurs de la référence et des participants. Ces résultats, en quelque sortes alarmants, mettent l'accent sur la nécessité d'avoir les possibilités de formation pour les technologues qui travaillent dans le domaine de la diagnostique clinique de la science de reproduction. Key Words: Sperm, morphology, Introduction The analysis of human semen in developing countries still remains the cornerstone of the male fertility investigations. Sperm morphology has been described as a single most important semen parameter that is consistently correlated with fertilization success both in vitro as well as in vivo1,2,3,4,5. The evaluation of the percentage normal sperm cells in a given ejaculate is an inexpensive and reliable method to obtain information regarding a man's fertility potential. In the absence of sophisticated first world technologies such as sperm functional assays (sperm zona binding, acrosome reactions), the evaluation of bioche-mical markers (Reactive oxygen species, creatinin kinase) and genetic investigations (chromatin packaging, DNA breakages), sperm morphology can be used as clinical tool to assist in the therapeutic choice6,7,8,9,10 However, the value of sperm morphology as predictor of a man's fertilizing potential has often been challenged due to different classification systems11. Several factors are responsible for this technical variation including differences in the methods used to prepare and stain specimens12, 13 differences in proficiency among technicians14,15,16 and inherent differences in classification criteria and methods17, 18, 1, 19. The discrepancies in laboratory results have increased to such an extent that some investigators often refer to the semen analysis as the `neglected test. 20 The objective of the present report was to record the (i) sperm morphology evaluation skills of a randomly selected group of health care workers from the Sagamu area in South-Western Nigeria and (ii) to evaluate the influence of hands-on training on their technical ability. Material & Methods During recent sperm morphology workshop held at the Centre for Research in Reproductive Health in Sagamu, 16 technologists enrolled for a 1-day sperm morphology workshop. The participants were requested to provide information regarding their experience and training as technologists in their institution. The format of the workshop consisted of 4 sections namely (i) pre-training evaluation, technologists were to record the percentage normal sperm on 2 pre-stained Papanicolaou slides prior to the training sessions (ii) lectures on morphometric characteristics and details of normal and abnormal sperm as described by Tygerberg strict criteria and the WHO 1999 manual (iii) a hands-on test during which participants were requested to evaluate a second set of 3 pre-stained slides and (iv) a consensus training session during which high quality photographs of numbered sperm cells were projected on a screen. For the consensus training session, each participant was provided with report forms allowing space for their own recordings as well as the reference recording. The reference results (results recorded by a trained sperm morphology technician, DRF) for each numbered sperm cell were only provided after completion of their own evaluations. Training material Delegates received a take-home reference set of 5 pre-stained Papanicolaou slides that were prepared using 3 donors. These slides were stained and scored for percentage normal sperm cells by the Reproductive Research laboratory at Tygerberg Hospital and served as reference slides during the workshop. Slide A and B were used to record the pre-training morphology reading skills of the participants, while 3 slides were used as post training material and served as test slides. Slide A contained sperm with >14% normal forms and slide B contained sperm with <4% normal forms. Slides 3, 4 and 5 contained sperm samples with varying percentage normal sperm on each slide for example slide 4 contained >14% normal cells, while slides 3 and 5 had between 5-9% normal cells. These slides served as a control to evaluate the participant's ability to identify normal sperm cells. Statistical analyses The pre-training results were used as a baseline to compare the results with the post training data. The pre-and post training sperm morphology results of the group were collected and presented as percentage difference from the mean value for each of the test slides that used during the training sessions. Findings Questionnaire The number of semen analyses performed by the group was 2-3 per day. One participant, a teacher from the anatomy department, did not perform semen analyses, since he attended the workshop for information purposes only. None of the 16 participants received formal training in the analysis of human semen. Unfortunately no details regarding their training are available. From the info provided in the questionnaire, the workshop delegates received informal in-house training provided by a senior laboratory person. Four participants had access to the WHO manual for the analysis of human semen and subsequently trained themselves. Six used a wet semen preparation to evaluate sperm morphology while, the rest used some staining method ranging from Papanicolaou (n=2), Eosin only (n=1), Sperm stain (BDH, Poole, England; Sperm stain, Cat number 35219 2F) (n=3) and the rest used a one-step haematoxylin staining method. None had access to a micrometer. Only 3 used a 1000X magnification, 2 used 400X while the rest used 100X magnification. Training sessions The (mean ±SD) pre-and post training results for the percentage normal sperm reported present on Slide A and B (pre-training slides) and Slides 3, 4 and 5 (post training slides) are tabulated in Table 1. The mean (±SD) percentage normal sperm cells reported by the participants for pre-training slide was 41.2±22% (range 10-70%) compared to the 17% normal forms recorded by the reference laboratory. The mean percentage normal forms reported by the participants on the pre-training slide B was 26.5±18.8% (range 3-64% normal forms), compared to the 4% normal forms recorded by the reference laboratory (Table 1). The mean percentage difference between the values reported by participants and reference values were 24.2±22% and 18.5±26% for pre-training test slides A & B. Following a hands-on training session the percentage difference between the participants and reference laboratory decreased to <10% for all 3 post-training test slides. Discussion The participants for the study were selected from a group of laboratory scientists that are actively working in a clinical andrology laboratory in the region of Sagamu. Although this small group of 16 participants can not represent the medical andrology laboratory population, we regard the data as a "dip-stick" evaluation of a specific population form one region in Nigeria. To establish the true level of knowledge of the laboratory scientists, a national study on a much broader base should be conducted. The findings of this study should be seen as a wake-up call for centres in developing countries that provide semen analyses for referring clinicians. If we regard the present findings as representative of medical laboratory scientist's sperm mor-phology reading skills, clinicians in Africa should be concerned about the diagnostic quality as far as male infertility is concerned. It is well known that the evaluation of the percentage of normal sperm morphology features with light micros-copy is subjective and therefore difficult to compare between laboratories, even within laboratories. Different means of assessing sperm morphology have been described2, 19, 21, 22, The most prominent problem in morphology classification and morphology scoring is the large variation coefficient (CV) that exists between and among different technicians in different laboratories. Despite the problems associated with the preparation of slides and staining methods, the use of different classification systems and the subjective nature of visual sperm morphology assessment, we still believe in the power of this important parameter in the routine semen analysis. This is especially true for laboratories in developing countries where the lack of sophisticated diagnostic laboratories is not readily available. Even basic material such as sperm stains can be difficult to obtain in certain areas of the continent. The lack of proper stains was basically the only reason why the majority of the workshop participants used unstained wet preparations for the morphology evaluations. The use of wet preparations is not acceptable, since not all the morphological details i.e. acrosome size, mid-piece and tail defects, can be observed. The inability of the participants to recognize sperm aberrations is clearly demonstrated by the findings of this study. The pre-training scores reported by the group ranged from 10-70% (median 40%) and 3-64% (median 22%) thus illustrating their total lack of knowledge regarding sperm morphology. Although, the study provided a pre-training test to obtain some idea of what the quality of semen examination among the group is. We acknowledge the fact that the pre-training evaluation was only done for morphology and future training courses should include all semen parameters i.e. sperm concentration, vitality and motility to get a better idea of the semen analysis quality. The authors strongly recommend medical laboratory scientists formal in-service training, before embarking in the field of diagnostic andrology. Tertiary institutions in each region should be able to provide training facilities in each of the different clinical technology diagnostic fields. These training sessions can be arranged in conjunction with established training centers if local expertise is not available. This arrangement would improve the quality service delivery and should become part of a national regulation for medical scientists that are responsible for clinical diagnostic reports. We firmly believe that the technical main-tenance for morphology readings is, apart from the initial training sessions, also dependant on a follow up external quality assurance programme23, 24. We have been recording the results of an external quality control programme for sperm morpho-logy since 1997, during which time pre-stained Papanicolaou slides were sent to trained individuals on a quarterly basis25, 26, 27. The results from previous studies showed, once trained, the technicians will maintain for a period of at least 6 months a high level of accuracy in their morphology assessments. Training of technicians as well as regular proficiency testing will ensure continuous communication with the referring laboratory. Proficiency testing of technician skills is of the utmost importance if andrology laboratories want to secure a professional code of conduct. We believe that this is a tendency that will occur in any andrology unit and laboratory directors should be aware of this phenomenon. Keel et al.,28 concluded that the only way to ensure comparable inter-laboratory results is through participation in a multicenter proficiency testing program28 The authors firmly believe that global quality control measurements in andrology laboratories will eventually become mandatory. A high quality semen analysis still represents the cornerstone in the investigation of the infertile couple. In order to maintain low intra- and inter-technician variation and high quality proficiency testing among laboratory technicians, continuous teaching programmes should be available to all. References
© Copyright 2007 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh07011f1.jpg] [rh07011t1.jpg] |
| |||||||||

{kind=link}
{kind=link}