 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 11, No. 2, August, 2007, pp. 60-69 Perception and Practice of Malaria Prophylaxis in Pregnancy among Health care Providers in Ibadan Onyeaso N.C, Fawole A.O Department
of
Obstetrics & Gynaecology,
University
College
Hospital,
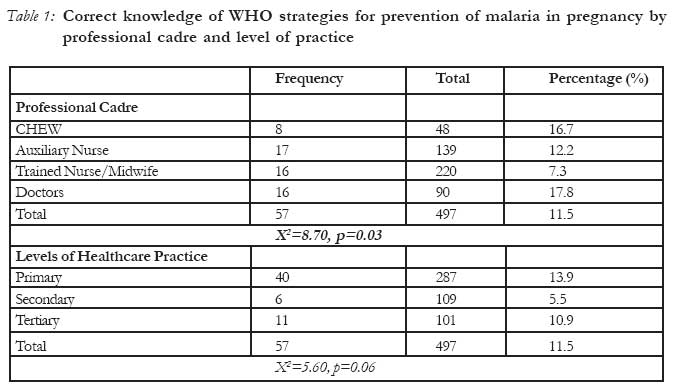
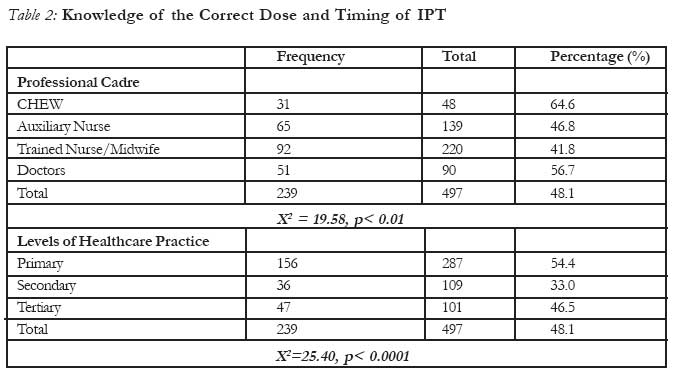
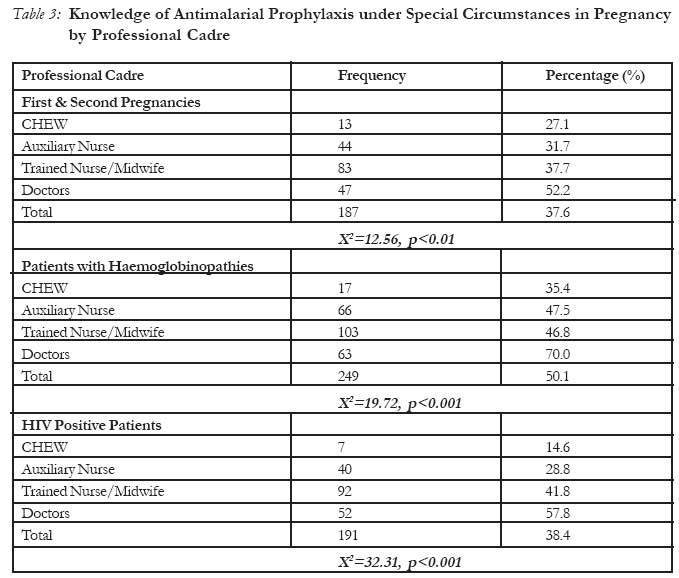
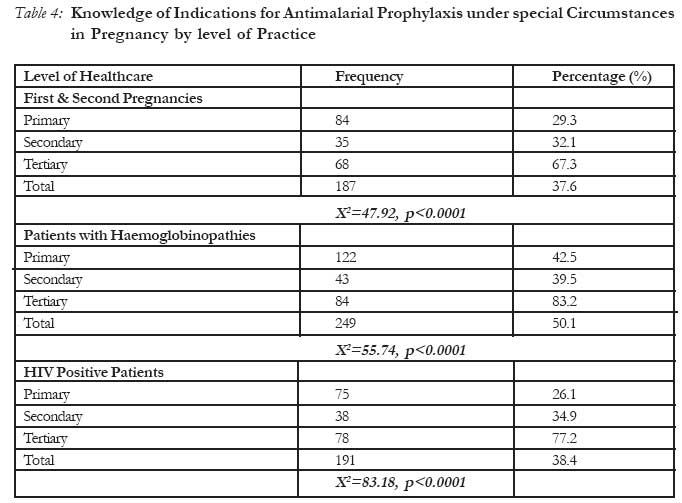
Ibadan Code Number: rh07021 Abstract The study assessed knowledge and practice of health care providers on current concepts on malaria prophylaxis in pregnancy. 497 randomly selected respondents at the three levels of care in two local governments in Ibadan, South western Nigeria were interviewed using a self-administered questionnaire. Respondents were selected from 45 health facilities: 48 (9.7%) community health extension workers (CHEWS), 139 (28.9%) auxiliary nurses, 220 (44.3%) formally trained nurses and 90 (18.1%) medical doctors. Only 57 (11.5%) respondents were knowledgeable about current WHO strategies for malaria prevention in pregnancy. Three hundred and eighty six respondents (77.7%) were aware of intermittent preventive treatment (IPT). Awareness about IPT was highest among CHEWS (95.8%). Pyrimethamine was prescribed mainly by healthcare providers in the secondary (60.6%) and primary (60.3%) levels of care (X2 = 11.54, p < 0.01). Chloroquine was prescribed by 42.5% of respondents. Sulfadoxine-pyrimethamine was significantly more commonly prescribed by primary health care providers than in other levels of care (X2 = 15.07, p < 0.01). Prescription for insecticide treated nets was high. Respondents' practice of anti-malarial chemoprophylaxis was influenced by the cadre of the health care provider and level of practice. There are several knowledge gaps on current malaria prevention strategies in pregnancy among healthcare providers. Multiple strategies are required to improve health care workers' knowledge and practice of malaria prevention during pregnancy. Résumé Perception et pratique de la prophylaxie du paludisme pendant la grossesse chez les dispensateurs des soins de santé à Ibadan L'étude a évalué la connaissance et la pratique chez les dispensateurs de soins de santé à l'égard de concepts courants à l'égard de la prophylaxie du paludisme pendant la grossesse. Nous avons selectionné au hasard 497 répondants à tous les trois niveaux de soin dans deux administrations locales à Ibadan au sud-ouest du Nigéria qui ont été interviewés à l'aide d'un questionnaire auto-administré. Les répondants ont été selectionnés aupres des 45 établissements de santé: 48(9,7%) parmi le personnel des services de santé extra-hospitalier (PSSEH) 139(28,9%) infirmières auxillaires, 220(44,3%) infirmières formellement formées et 90(18,1%) médecins. Seuls 57(11,5%) des répondants connaissaient les stratégies courantes de l'OMS pour la prévention du paludisme pendant la grossesse. Trois cent quatre-vingt-six répondants (77,7%) étaient au courant du traitement préventif intermittent (TPI). La conscience du TPI était la plus élevée parmi les PSSEH (95,8%). Les dispensateurs de soins de santé ont surtout prescrit pyriméthamine au niveau secondaire (60, 6%) et au niveau primaire (60,3%) de soin (X2 = 11, 54, p < 0, 01). Chloroquine a été prescrite par 42,5% des répondants. Sulfadoxine-pyriméthamine a été, de manière signifactive, la plus communément prescrite par les dispensateurs des services de soins primaries qu'à d'autres niveaux de soin (X2 = 15, 07, p < 0, 01). La prescription pour les moustiquaires traités à l'insectide était considérable. La pratique de la chemoprophylaxie antipaludisme a été influencée par le cadre du dispensateur de soin de la santé et le niveau de la pratique. Il y a beaucoup de vide quant aux stratégies actuelles de la prévention du paludisme pendant la grossesse parmi les dispensateurs de soin de la santé. Il faut de multiples stratégies pour améliorer la connaissance et la pratique de la prévention du paludisme pendant la grossesse chez les dispensateurs de soin de la santé. (Rev Afr Santé Reprod 2007; 11[2]:60-69). Key Words: malaria in pregnancy, intermittent preventive treatment, malaria control, health care providers Introduction Malaria is a major public health problem, with the largest population at risk in sub-Saharan Africa. At least 300 million people become acutely ill with malaria each year, and more than a million die from the infection1. Over 80% of malaria deaths occur in Africa2. Malaria costs Africa an estimated 12 billion US dollars in lost production yearly2. Pregnant women and their unborn babies are especially vulnerable to malaria. Each year, more than 25 million African women in malaria-endemic areas become pregnant and are at risk of infection with Plasmodium falciparum2,3. Infection with Plasmodium falciparum during pregnancy increases the risk of maternal anaemia, spontaneous abortion, stillbirth, low birth weight and neonatal death, and is thought to be responsible for the death of approximately 10,000 African women and 200,000 infants each year4. The World Health Organization (WHO) recommends a package of interventions for the prevention and control of malaria during pregnancy. This comprises of intermittent preventive treatment (IPT), use of insecticide treated nets (ITNs), and access to effective case management for malaria illness and anaemia3. Routine prophylaxis for malaria during pregnancy is associated with reduced incidence of severe antenatal anaemia, higher birth-weight and fewer perinatal deaths5. ITNs have been shown to have beneficial impact on pregnancy outcome in malaria-endemic regions of Africa when used by communities or individual women6. Presently, sulfadoxine-pyrimethamine (SP) is the only antimalarial medicine for which data on efficacy and safety for IPT is available from controlled clinical trials, and WHO recommends that at least 2 doses of SP are given after quickening during the second and third trimesters, at least one month apart. However even a single dose has been shown to be beneficial7. One of the major challenges facing the implementation of malaria prevention strategies in pregnancy is creating awareness among healthcare providers8. A recent evaluation of the malaria prevention strategies using drugs among Nigerian obstetricians revealed that the majority were deficient in current evidence-based recommendations9. A policy document has been produced by the Nigerian health authority to guide health care workers on strategies for the prevention and control of malaria during pregnancy10. Therapeutic regimes used by healthcare workers are usually not in compliance with such guidelines as shown in the Republic of Benin where physicians and health care workers were unaware of their national policies for the control of malaria11. Thus there appears to be a poor knowledge base regarding current evidence-based guidelines on malaria control during pregnancy among health care workers. Yet healthcare workers are crucial to effective malaria control. Therefore it is necessary to investigate their knowledge base on this crucial issue. Thus this study was designed to assess the knowledge of health care providers in Ibadan, south-western Nigeria on current concepts on malaria prophylaxis in pregnancy, to ascertain their preferred drugs and to identify strategies that would enhance programmes for preventing malaria during pregnancy. Methods This cross sectional descriptive study was conducted in Ibadan, Oyo state of south-western Nigeria between June and August 2006. Two of the five local government areas (LGAs) within Ibadan municipality were selected by random sampling. The selected LGAs were Ibadan North and Ibadan North East respectively. In each local government area, two public primary health facilities and a secondary health facility and at least 25% of all registered private health facilities were randomly selected from a list of all registered health facilities obtained from the Oyo state ministry of health. Within Ibadan North LG, there were 10 public primary health facilities, one public secondary facility and a tertiary health facility. There were 115 registered private hospitals, clinics and maternity centre within the local government. In Ibadan North East local government, there were 13 public primary health facilities, 2 public secondary health facilities and 14 registered private hospitals, clinics and maternity centres. The only tertiary health care facility in Ibadan located within Ibadan North local government was selected. The main study population consisted of all health care personnel who provide antenatal services in the selected health facilities. These included community health extension workers (CHEWs), auxiliary nurses, formally trained nurses and medical doctors. CHEWs are individuals with minimal education who have received some basic formal training; they are employed in primary health centres and provide maternity care. Auxiliary nurses are individuals with minimal education who are employed in private health facilities. They are given on-the-job training by individual Physicians; they also provide maternity care. Auxiliary nurses do not have formal training prior to employment. At the primary level of care in public health facilities, the health care personnel include CHEWs, trained nurses and midwives and a few Physicians. Auxiliary nurses, CHEWs, trained nurses and midwives and Physicians are the personnel in private health facilities. There are only trained nurses and midwives and Physicians in public secondary and tertiary health facilities. A pre-designed semi-structured self-administered questionnaire was given to randomly selected healthcare workers representing all cadres of healthcare workers who managed pregnant women in the different levels of healthcare. The questionnaire explored the respondents' knowledge of the hazards posed by malaria to pregnancy, current strategies for preventing it and their current practice regarding prophylaxis for malaria among pregnant women. It was pre-tested and the questions validated prior to commencement of the study. Ethical approval was obtained from the Joint University of Ibadan/University College Hospital institutional review board. Approval for the study was also sought from the authorities of all selected health facilities. A trained research assistant distributed the questionnaires and recruited participants for the study. Each participant signed a written consent form after being given adequate explanation about the purpose of the study. Completed questionnaires were cleaned and edited prior to data entry. Data entry and analysis were performed using the EPI-Info 6 statistical package from the US Centers of Disease Control and Prevention. The chi-square test was used to test for associations and the level of statistical significance was set at p < 0.05. Results A total of 551 questionnaires were administered; of these 501 were retrieved and 497 were sufficiently completed to permit detailed analysis. They were administered in 45 randomly selected health facilities in Ibadan North and Ibadan North East local government areas of Ibadan. The distribution of the un-completed questionnaires cut across the different levels of care and private and public health facilities. No refusals were reported. Of these 45 health facilities, one was a tertiary healthcare facility and two were secondary healthcare facilities; one public and the other a missionary hospital. Of the remaining forty-two primary healthcare facilities, five were public health facilities and 37 were privately owned. Two hundred and ninety six respondents (59.6%) were in Ibadan North LGA while the remaining 201 respondents (40.4%) were in Ibadan North-East LGA. Overall, 287 (57.8%) respondents were in primary, 109 (21.9%) were based in secondary and the remaining 101 (20.3%) were found in the only tertiary healthcare facility. Forty-eight respondents (9.7%) were community health extension workers (CHEWS), 139 respondents (28.9%) were auxiliary nurses. Formally trained nurses comprised 220 respondents (44.3%) while the remaining 90 respondents (18.1%) were medical doctors. The majority of respondents (94.6%) felt that training on malaria control should be institutionalized. Most respondents (90.3%) felt the Federal government should subsidize antimalarial interventions. Knowledge of WHO strategies on malaria prevention in pregnancy was poor with 57 respondents (11.5%) having correct knowledge of all WHO strategies. Table 1 depicts knowledge of all WHO recommended strategies by professional cadre and levels of healthcare. A total of 386 respondents (77.7%) were aware of intermittent preventive treatment. Awareness was highest among CHEWS (95.8%). Though 349 respondents (70.2%) believed IPT to be effective, 93 respondents (18.7%) felt a single dose could be beneficial. Knowledge among professional cadres and levels of healthcare practice of the correct drug, dose and timing of IPT is depicted in Table 2. CHEWs were more likely than other cadres of healthcare workers to correctly indicate the correct dose and timing of IPT (X2 = 19.58, p < 0.01); respondents at the primary level of care were also more likely to report the correct dose and timing of IPT (X2=25.40, p < 0.0001). Sulfadoxine-pyrimethamine was the most widely prescribed antimalarial for prophylaxis with 335 respondents (67.4%) prescribing it. Its use was highest among CHEWS (77.1%) followed by auxiliary nurses (73.4%) and medical doctors (64.4%). It was least prescribed by trained nurses/midwives (62.7%). These differences however did not reach statistical significance (X2=6.86, p > 0.05). Healthcare providers at the primary level of care were significantly more likely to use sulfadoxine-pyrimethamine for IPT than other levels of care, followed by tertiary healthcare providers (65.4%). SP was least used by secondary healthcare providers (53.2%). These differences were statistically significant (X2 = 15.07, p < 0.01). The prescription for use of insecticide treated nets was generally high with 75.1% of respondents prescribing it. It was most prescribed by trained nurses/midwives (80.0%) followed by auxiliary nurses (79.9%) and CHEWs' (72.9%). It was least prescribed by doctors (56.67%); these differences were statistically significant (X2=20.95, p < 0.001). Two hundred and eleven respondents (42.5%) prescribed Chloroquine (CQ) as antimalarial prophylaxis in pregnancy. CQ was most prescribed by CHEWs' (54.2%) followed by auxiliary nurses (48.9%) and trained nurses/midwives (44.6%). CQ was least prescribed by Medical Doctors (21.11%) and the differences were statistically significant (X2 = 22.25, p < 0.0001). Chloroquine for antimalarial prophylaxis was more frequently prescribed by primary healthcare providers (49.8%), followed by secondary healthcare providers (36.7%); only 27.7% of tertiary healthcare providers prescribed it (X2=16.83, p < 0.001). Proguanil was prescribed by 191 respondents (38.43%). Its prescription was highest among medical doctors (55 respondents, 61.1%), followed by trained nurses/midwives (93 respondents, 42.3%) and auxiliary nurses (35 respondents, 25.2%). It was least prescribed by CHEWS (8 respondents, 16.7%). The differences in these prescription patterns attained statistical significance (p < 0.0001). By level of healthcare, tertiary healthcare providers prescribed it most (82 respondents, 81.2%) followed by secondary health care providers (35 respondents, 32.1%) while 74 primary healthcare providers (25.8%) prescribed it (p < 0.0001). Two hundred and eighty-one respondents (56.5%) prescribed pyrimethamine for antimalarial prophylaxis. It was mostly prescribed by auxiliary nurses (98 respondents, 70.5%), followed by trained nurses/midwives (123 respondents, 55.9%) and CHEWs' (23 respondents, 47.9%). It was least prescribed by medical doctors (37 respondents, 41.1%). The differences reached statistical significance (X2 = 21.24, p < 0.0001). Pyrimethamine was mostly prescribed by secondary healthcare providers (66 respondents, 60.6%) and primary healthcare providers (173 respondents, 60.3%). It was least prescribed by tertiary healthcare providers (42 respondents, 41.6%). These differences also reached statistical significance (X2 = 11.54, p < 0.01). CHEWs were least likely to correctly identify groups of pregnant women that required IPT as shown in Table 3. The majority of respondents from primary and secondary levels of care could not correctly indicate groups of pregnant women at higher risk of the effects of malaria (Table 4). Discussion Provision of care conforming to standard guidelines is one of the major elements of quality of care12. Consequently, periodic assessment of practice will yield valuable insights regarding the quality of care given to pregnant women. Such an endeavour is particularly relevant in the control of malaria during pregnancy from the public health perspective. Current strategies for malaria control in pregnancy are based on the tripod of IPT, vector control and prompt treatment of acute illness. The performance of any health system with regards to control of malaria and thereby reduction of malaria related morbidity and mortality can thus be evaluated by the extent to which it meets these best practices. This study revealed a poor knowledge of WHO strategies against malaria in pregnancy among healthcare providers; only one-tenth were aware of the correct WHO strategies. This poor knowledge was evident among all cadres and levels of healthcare providers. Approximately three-quarters of respondents were aware of intermittent preventive treatment. Sulfadoxine-pyrimethamine (SP) was the most widely prescribed antimalarial for prophylaxis with approximately two-thirds of respondents prescribing it in pregnancy. This was not surprising as its low cost, wide availability, easy deliverability and acceptability make it the clear choice in countries where efficacy of the drug remains good13. However, further assessment of the awareness revealed surprising knowledge gaps. Only half of respondents knew the correct dose and timing of IPT. This was dependent on both professional cadre and level of healthcare with the CHEWs' and primary healthcare providers being most knowledgeable. This could be due to the fact that WHO efforts are focused on developing primary healthcare practice in the developing world, so these groups are better educated and informed about current WHO strategies. Three-quarters of respondents prescribed insecticide treated nets (ITNs) for use. As heartwarming as this might be, it is important to note that prescription for use does not necessarily lead to similar coverage results. Attributable reasons for the difference include cost of ITNs' which is a barrier to their widespread use and the erroneous perception in some areas that chemicals for treatment of nets could be harmful14. The disheartening and alarming news is that approximately half of our doctors do not counsel patients on the use of ITNs' which has been shown to be effective. Approximately two-fifths and three-fifths of healthcare providers still prescribe chloroquine and pyrimethamine respectively despite overwhelming evidence against such practice due to increasing resistance to these drugs, and reducing efficacy of chloroquine (CQ) chemo-prophylaxis15 and weekly pyrimethamine16,17. The possible reasons for this would include easy availability, affordability. Another important but often overlooked reason could be the inefficient dissemination of current information to healthcare providers leading to ignorance and poor knowledge of drug resistance patterns and efficacy. Assessment among respondents of knowledge of the groups of pregnant women that need antimalarial prophylaxis again showed several knowledge gaps. Only about two-fifths of all respondents agreed to use of malaria prophylaxis for first and second pregnancies and HIV patients, while only half felt use of prophylaxis for sickle cell disease patients was appropriate. This is disappointing as it is known that the deleterious impact of malaria is particularly more in first and second pregnancies18. Additionally women with HIV infection are more likely to have symptomatic malaria infections and to have an increased risk of an adverse birth outcome due to malaria3. Anti-malarial prophylaxis in this group is justified given the association of placental parasitaemia with increased risk of vertical transmission of HIV 19, 20. The WHO therefore recommends three IPT doses for HIV positive women3. IPT is also recommended for patients with sickle cell disease as this reduces the possibility of sickle cell crisis due to malaria infections21. Conclusion and Recommendations This study has highlighted several knowledge gaps on current malaria prevention strategies in pregnancy among healthcare providers. Lack of awareness is apparently the major obstacle to changing practice8; incorporating new strategies into routine antenatal care programmes will therefore require active dissemination of this information among the various cadres of health workers providing antenatal care. Possible solutions include institutionalizing malaria prevention strategies in pregnancy22 and continuing professional development programmes on current concepts by healthcare providers. Professional associations by their strategic positions should indeed take the lead in this area. Some researchers have advocated the creation of an organization to promote consultation and communication between health care authorities and workers11. Acknowledgements We acknowledge the co-operation of the staff of Obstetrics and Gynaecology departments of the University College Hospital, Ibadan, Catholic Hospital, Oluyoro, Ibadan, and Adeoyo Maternity Hospital, Ibadan. The contribution of the research assistants and all the participants in this study is gratefully acknowledged. References
© Copyright 2007 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh07021t1.jpg] [rh07021t3.jpg] [rh07021t4.jpg] [rh07021t2.jpg] [rh07021f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}