 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 11, No. 2, August, 2007, pp. 86-89 Heparin and Aspirin in Pregnant Sudanese women with Recurrent Miscarriage Associa-ted with Antiphospholipid Antibodies Yagoub M. A/Magid 1, Elsir A. Elussein1, Maha M. Omer1, Samaan I.Samaan1, Fawzi A/Rahim2, Ishag Adam1,3* 1Khartoum
fertility
center,The
Academy
of
Medical
Sciences
and
Technology,
Sudan.
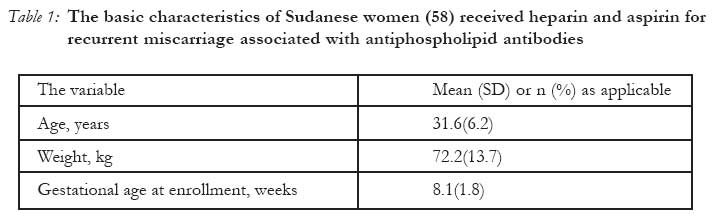
Code Number: rh07024 Abstract This was a prospective clinical trial conducted at Khartoum Fertility Center, during the period June 2002 to February 2005 to investigate the efficacy of unfractionated heparin and low-dose aspirin as prophylaxis against pregnancy loss in 58 pregnant Sudanese women with recurrent (>3) miscarriages associated with antiphospholipid syndrome (APS). Three (5.1%) patients had early miscarriages, three (5.1%) patients developed pre-eclamptic toxaemia and forty-seven (81%) of the 58 patients had cesarean delivery. Forty-seven (81%) women had live births and 8(13.8%) had preterm deliveries. Eight (13.8%) of the neonates were admitted to the intensive care unit for various reasons. There were 6(10.3%) perinatal deaths, all of them were due to prematurity. None of the patients developed thromboembolic episode. There was no maternal death. The rate of live birth in this study was consistent with the previous reports. This was a none controlled study; thus controlled clinical trials using low molecular weight heparin are urgently needed. (Afr J Reprod Health 2007; 11[2]:). Résumé L'héparine et l'aspirine chez les femmes soudanaises enceintes qui ont fait fréquemment des fausses couches liées aux anticorps antiphospholipides Cette étude a été un essai clinique perspective menée au Centre de fécondité à Khartoum au cours de la période du mois de juin 2002 au février 2005 afin d'enquêter l'efficacité de l'héparine nonfractionnée et de l'aspirine à dose faible comme une prophylaxie contre la perte de grossesse chez 58 femmes soudanaises enceintes qui ont fait fréquemment (= 3) des fausses couches liées au syndrome d'antiphospholipide (SAP). Trois (5,1%) patientes ont fait des fausses couches précoses, trois (5,1%) patientes ont fait de la toxémie éclamptique et quarante-sept (81%) sur les 58 patientes ont accouché à l'aide de l'opération césarienne. Quarante-sept (81%) femmes ont eu des naissances vivantes alors que huit 8(13,8%) ont eu des accouchements pré-termes. Huit (13,8%) parmi les nouveaux-nés ont été admis dans l'unité de soins intensifs pour des raisons différentes. Il y a eu 6 (10, 3%) décès périnatals, tous à cause de la prématurité. Aucune des patientes n'a fait de l'épisode thromboembolique. Il n'y a pas eu de décès maternel. Le taux de naissance vivante dans cette étude était en accord avec les rapports précédents. Celle-ci a été une étude non contrôlée; ainsi, on a besoin des essais cliniques contrôlés à l'aide de l'heparine à poids moléculaire faible. Key Words: miscarriage, pregnancy, heparin, aspirin, Sudan Background Antiphospholipid syndrome (APS) is encountered in most areas of clinical medicine with a wide spectrum of signs and symptoms. The etiology and pathogenesis of antiphospholipid syndrome remain uncertain, so its treatment has remained speculative. Recurrent miscarriage affects 1% of pregnant women, 15-40% of these women have APS1. Recently APS was found to be the main risk factor for recurrent miscarriage among Sudanese women2. The optimal therapeutic management of patients with APS during pregnancy is debatable. Low_dose aspirin (LDA), steroid, heparin and combination of these treatments are the treatment for antiphospholipid syndrome3-5. However, because of the contro-versies in the outcome of these clinical trials, there is a need for further researches in this field of medicine. Materials and Methods This was a prospective descriptive study that investigated the efficacy of unfractionated heparin (UFH) and LDA as prophylaxis against pregnancy loss in pregnant Sudanese women with recurrent miscarriage associated with APS. The study was conducted at Khartoum Fertility Center, during the period June 2002 to February 2005. Women with three or more documented consecutive pregnancy losses before 20 gestational weeks and antiphospholipid antibodies (anticardiolipin immunoglobulin G and M antibody and /or lupus anticoagulant) were approached to participate in the study. To minimize inter and intrapersonal error, these tests were conducted by the same immunologist using standard ELISA to detect these antibodies. Women were excluded if they had systemic lupus erythromatosis or history of thrombosis, if they had another cause of the recurrent miscarriage or if they did not have two positive tests for antiphospholipid antibodies. At enrollment, clinical history and physical examination, complete blood count, routine biochemical investigation (including thyroid functions) were performed. Once pregnancy was confirmed (if antiphospholipid was already diagnosed before pregnancy) or on discovery of antiphospholipid antibodies during the index pregnancy, the patients were taught to self-administer UFH subcutaneously (5, 000 IU, twice daily) and LDA (100 mg, daily, the only available form in Sudan) and were followed with serial ultrasound and clotting profile (including platelets count) every two weeks until delivery. The treatment was continued at full term (37 weeks) and was discontinued only when the patient initiated spontaneous labour or 12 hours before elective cesarean section delivery. The treatment of UFH and LDA were resumed one day after the delivery as maternal thrombosis prophylaxis. The compliance of UFH was assessed by inspection of the injection site and that of LDA by the frequency of the prescriptions and by asking the patient directly. The outcome measures were the rates of live births, antenatal complications, delivery and neonatal outcomes. Ethical clearance The study received ethical clearance from the Ethical Committee of the Faculty of Medicine, The Academy of Medical Sciences and Technology, Sudan. Results Sixty- one consecutive patients were enrolled in the study; three patients lost to follow-up and the rest (fifty-eight) completed the study. The basic characteristics of the women are shown in Table 1. Three (5.1%) patients had early miscarriages. Three (5.1%) patients developed pre-eclamptic toxaemia (diastolic blood pressure > 90 mm Hg in two readings 6 hours apart with 2+ or more of proteinurea). One patient suffered diabetes mellitus during pregnancy. Forty-seven (81%) of the 58 patients had cesarean delivery. Forty-seven (81%) women had live births and 8(13.8%) had preterm deliveries. The mean (SD) birth weight was 2.7(0.54) Kg. One baby had cleft lip. Eight (13.8%) of the neonates were admitted to the intensive care unit for various reasons. There were 6(10.3%) perinatal deaths all of which were due to prematurity. None of the patients developed thromboembolic episode. There was no maternal death. Discussion This is the first published clinical trial to investigate the efficacy of UFH and LDA in APS among Sudanese women. The study showed that the rates of live births and perinatal deaths were 81% and 10.3 % respectively, most of the perinatal deaths resulted from prematurity. This goes with previous observations6, 7 using heparin and LDA in spite of the difference in the types of heparin between the present and the former trial. However, both types of heparin (low molecular weight and unfractionated heparin) were reported to have similar results in terms of maternal and fetal complications6, 8. This should be weighted against the patients' compliance and the adverse effects of UFH. Surprisingly, even though LMWH was used without LDA, 92.59% of the cohort delivered live infants9. In contrast to the success rate of 70% -75% when UFH was used with LDA compared with the succesful pregnancy rate of 45% when LDA was used alone7,10. However, it has been reported that, the addition of LMWH to LDA did not significantly improve pregnancy outcome in pateints with APS11. In contrast to previous reports, where treatment with LDA and UFH had signficanlty higher rate of live birth in comparison to LDA alone7. Patitison and colleagues reported eighty-five percent of the placebo group and 80% of the aspirin-treated group for APS delivered live infants without signficant difference in antenatal complications or neonatal morbidity between the groups. It is noteworthy that, in the absence of APS, the live birth rate for a prospectively observed group with idiopathic recurrent miscarriage is 75%, with 20 % and 5% embryo and fetal loss respecively12. Neverthless, any discussion of treatment of recurrent miscarriage associted with APS must take into account the spontaneous cure rate which is 50 % among unselected cases and 10% of women with APS have live birth without treatment13,14 . Extensive obstetrical monitoring was performed in this trial and in all clinical trials conducted to investigate APS and its treatment, this might be one of the reasons behind the high perecentage of live births in all these trials in spite of the use of different regimens. High caesarean section rate (81%) was also observed in this trial, probably because many factors like maternal age and the duration of marriage influenced the decision of the operative deliveries rather than APS or its treatment. In this study, fetal outcome was favourable in 89.7% of the treated women. This goes with other observations in cohorts of treating pregnant women with APS15,16. This trial, like all other trials in this field, is small but its results bring into question the need for pharmacologic intervention for women with APS for whom recurrent fetal loss is the only sequela. Our results highlight the need for a large randomized controlled trial to identify the optimal treatment for this group of women. Further controlled clinical trials using LMWH are urgently needed. References
© Copyright 2007 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh07024t1.jpg] |
| |||||||||

{kind=link}