 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
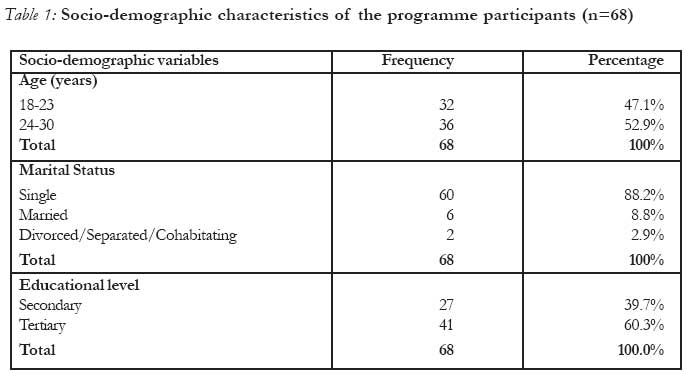
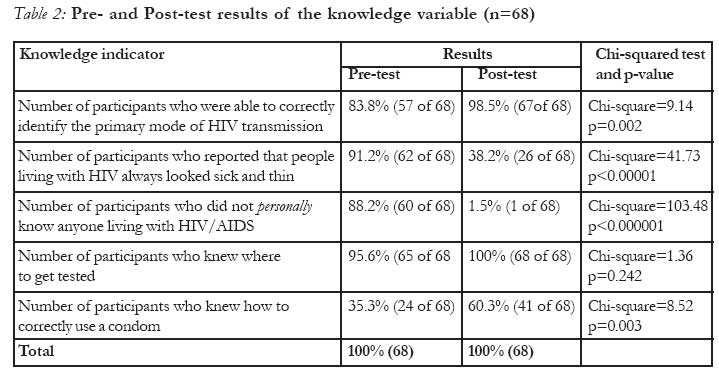
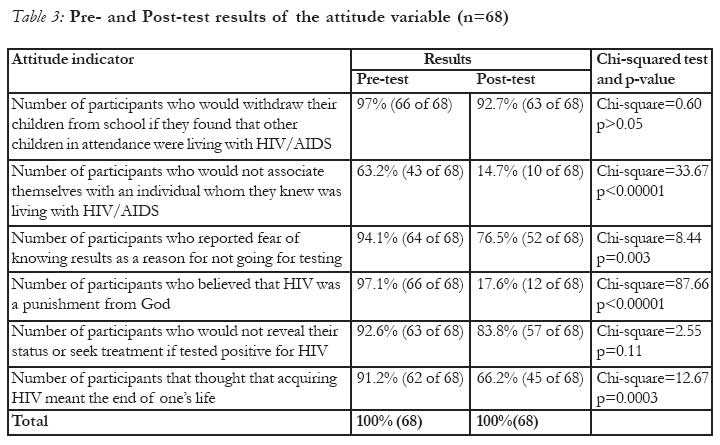
African Journal of Reproductive Health, Vol. 11, No. 2, August, 2007, pp. 90-97 CASE REPORT Findings from an HIV/AIDS programme for young women in two Nigerian cities: A short report Oluseyi O. C. Lawoyin Correspondence: Oluseyi O.C. Lawoyin. National Academy of Sciences, Washington DC. Slawoyin@gmail-com Code Number: rh07025 Abstract This short report describes the findings from an HIV/AIDS programme for young women that was held in two Nigerian cities. Very little information is available on interventions that address the needs of young Nigerian women; a population that represents a high incidence and prevalence of HIV and AIDS. Responses were elicited from the programme participants through the use of pre-and post-test questionnaires, with a view to identifying effective health education strategies for the prevention of sexually transmitted infections including HIV/AIDS among young Nigerian women. Outcomes revealed low knowledge levels, poor attitudes and misconceptions about HIV/AIDS as well as widespread stigma. This indicates a continual need for the design and implementation of a comprehensive and culturally appropriate HIV/AIDS and sexual health program for young women in Nigeria which meets their needs. Résumé Conclusions tirées d'un programme de sensibilisation au VIH/SIDA destiné aux jeunes femmes dans deux villes nigérianes: Bref rapport Ce bref rapport fait une description des résultats d'un programme de sensibilisation destiné aux jeunes femmes qui a été réalisé dans deux villes nigérianes. Il n'existe que très peu de renseignements sur les interventions qui s'occupent des besoins des jeunes femmes nigérianes; une population qui représente une haute incidence et prévalence du VIH/SIDA. Nous avons sollicité des réponses de la part des participants au programme à l'aide des questionnaires de pré et post-formation, dans le but d'identifier les stratégies efficacies de la santé de l'éducation pour la prévention des infections sexuellement transmissibles y compris le VIH/SIDA chez les jeunes femmes nigérianes. Les résultats des enquêtes ont montré de bas niveaux de connaissance, de mauvaises attitudes et des idées fausses à l'égard du VIH/SIDA aussi bien qu'un stigmate répandu. Ceci signale un nécessité continue pour la conception et la mise en place d'un programme du VIH/SIDA et de la santé sexuelle qui soit comprehensif et culturellement approprié destiné aux jeunes femmes nigérians qui répond à leur besoin. (Rev Afr Santé Reprod 2007; 11[2]:90-97). Key Words:Stigma, Nigeria, young women, HIV knowledge Literature review According to the Joint United Nations Programme on AIDS (UNAIDS), there were an estimated 24.5 million people living with HIV/AIDS at the end of 2005 in Sub-Saharan Africa, a number that makes up 65% of the world's total HIV prevalence rates.9 The epidemic disproportionately affects girls and women within the region, where women are 3.4 times more likely to be infected with HIV/AIDS than their male counterparts.9 In Nigeria, the HIV prevalence rate for women between the ages of 15-29 years was at 13.2% by 2005.9 Lack of adequate knowledge has been cited as one of the reasons for high risk hetero-sexual behaviour, which results in the high incidence of HIV among young people within the Sub-Saharan African region. 1 The 2001 United Nations General Assembly (UNGASS) Declara-tion of Commitment on HIV/AIDS called for a 90% coverage of young people on compre-hensive knowledge of HIV/AIDS.9 However, surveys indicate that fewer than 50% of young people failed to achieve comprehensive knowledge levels.1 Although there are many programmes that target HIV prevention in Nigeria, there is a paucity of data on HIV prevention programmes that address the needs of young women, a population that stands a higher risk of becoming infected with HIV than their young male counterparts. In order to address this issue, a culturally appropriate and comprehensive HIV/AIDS programme was organized for young women in two Nigerian cities. The purpose of the programme was to provide the young women with accurate information about HIV and AIDS, to foster positive attitudes towards people living with HIV/AIDS (PLWHA), and to allow young women to develop skills aimed at informing intended behaviour. This short report provides a brief description of findings from this programme, which will help in designing more effective strategies for the prevention of sexually transmitted infections including HIV/AIDS, among young Nigerian women. Materials and Methods Programme Design and Participant Selection The programme was held in the cities of Ibadan and Lagos in southwest Nigeria, and was attended by a total number of sixty-eight participants between the ages of 18 - 30 years of age, with thirty-five and thirty-three young women in attendance in both Ibadan and Lagos respectively. These two cities were chosen because of their affiliations with United States diplomatic presence in southwest Nigeria at the time of programme implementation. This provided for easy access to avenues of support in terms of programme setup and arrangement. The sample of young women who participated in both sessions were randomly selected by invitation from local secondary and tertiary institutions. A total number of seventy invitations were distributed equally between the two cities. Over one third of the programme participants (39.7%) attended secondary institutions, while more than half (60.3%) attended tertiary institutions (see table 1). In the city of Ibadan, schools were selected based on their large size, with the aim of reaching a broad selection of potential participants. The University of Ibadan and The Polytechnic, Ibadan were chosen based on this criterion. The programme was advertised in the schools and young women who were interested in attending it received an invitation on a first come first serve basis. All thirty-five recipients of the invitations attended the programme. The sessions were held at the American Corner located in the old British Council Building in Jericho, Ibadan. In preparation for the programme in the city of Lagos, the programme was advertised at the U.S. Consulate's Educational Advising Center (EAC), a venue where students interested in further studies in the United States received training. The EAC was chosen based on its ability to reach a broad selection of programme participants due to the diversity of the students that attend the center. Consequently, the programme in Lagos had young women who were at the time, currently attending both secondary and tertiary institutions in different parts of the city. Young women who were interested in attending the programme were allowed to pick up invitations from the EAC's information desk. Thirty-three young women honoured the invitations. The sessions were held in the pressroom of the U.S. Consulate's Public Affairs Section. A facilitator, who was also a young Nigerian woman and an expert in the area of HIV prevention and advocacy, was invited to conduct the programme in both cities. Sessions were a daylong, and were held from eight in the morning to five in the evening in both cities. The programme was small in size in order to promote an informal, relaxed and open environment to allow for interaction and the young women to ask questions about sensitive issues of concern to them. Participants in both cities volunteered their time and monetary resources to attend the programmes. While they were responsible for arranging their own transportation to and from the venues, they were provided with lunch packs to compensate for it. The use of visuals and educative materials were employed to illustrate messages. Copies of these along with other informational brochures and pamphlets were handed out in folders to the participants during the sessions. Although the programme was held in two different locations, the content was the same. It followed an HIV/AIDS prevention and life skills education curriculum that was developed by the programme facilitator, and was divided into the following components: Abstinence to negotiating safe sex; providing care and support for people living with HIV/AIDS (PLWHA); culture and sexuality; stigma and discrimination; and HIV prevention, testing and treatment. In addition, the women were shown how to put on a male condom and were introduced to the female condom. Data collection and analysis Data and information was collected using structured questionnaire and informal group discussions. The instruments used for quantitative data collection were self-reported pre- and post-test questionnaires that were administered by the author, and were designed to assess knowledge and attitudes towards HIV/AIDS and sexual health as part of the programme activities. Participants filled out the pre-test questionnaires before the programme commenced and were given the same set of questions in post-test questionnaires to fill out a few minutes before it ended. Verbal informed consent was obtained from respondents. Confidentiality was maintained and their names were not required. Questions were asked on the socio-demographic characteristics of the participants (see table 1) as well as on HIV/AIDS knowledge that addressed HIV transmission, knowledge of serostatus, knowledge of the use of contraceptives and places to get tested, and general knowledge on the effect of HIV on the human body (see table 2). The main components of the attitude variable included questions that addressed stigma and discrimi-nation towards PLWHA, stereotypes and personal risk (see table 3). Participants recorded positive (yes) or negative responses (no) to a total of twelve questions on the knowledge and attitude variables. It is important to note that although all qualitative information was recorded on tape, there are no raw numbers to represent it. Many of the reasons behind the responses to the questions on the questionnaires were discussed informally among the programme participants during the course of the sessions and used to complement the data obtained from the questionnaires. Differences in responses were identified using the chi-square analysis. Findings from the pre-test questionnaire Knowledge of HIV and AIDS Knowledge levels were fairly low, while miscon-ceptions were very common. When programme participants were asked how the HIV virus was transmitted, only 57 (83.8%) of the participants were able to correctly identify the primary mode of transmission. Many expressed the belief that they could become infected by sharing the same eating utensils or bed with a person living with HIV/AIDS (PLWHA). Some of the participants thought they could become infected with HIV if the saliva from a PLWHA accidentally sprayed on their skin while talking to them. Others thought they could become infected by shaking hands or hugging a PLWHA. When asked if they correctly knew how to use a condom, a low number, over a third, 24 (35.3%) responded in the affirmative. Almost all participants, 65 (95.6%), knew where to get tested for HIV and AIDS, However, 64 (94.1%) participants did not know their HIV serostatus. 62 (91.2%) were of the belief that people living with HIV/AIDS always looked sick and thin. 62 (91.2%) also believed that acquiring HIV meant the end of one's life and saw the situation as a death sentence. When asked if they personally knew anyone who was living with HIV, 60 (88.2%) participants responded that they did not. For testing purposes "personally" was defined in this instance as participants who knew a PLWHA on an individual basis without the influence of hearsay or a third party. Attitudes towards HIV and People living with HIV/AIDS (PLWHA) A scenario was depicted where participants were asked if they would withdraw their own children from school if one of the other children in the classroom was living with HIV, 66 (97.1%) participants responded in the affirmative, stating that the nature of the interaction among young children might cause the infection to spread. Participants who agreed to keep their children in the classroom responded stating that taking their children out of school would be discriminatory, and they would prefer to talk to the teacher about maintaining precautionary measures among the children (for example, keeping them away from sharp objects). Over half, 43 (63%) of programme partici-pants said that they would not associate themselves with a person whom they knew was living with HIV/AIDS (PLWHA). As a follow-up to knowledge question on individual HIV serostatus, participants (those who did not know their serostatus), were asked if fear of knowing results was a factor influencing their decision to go for testing. All 64 (94.1%) responded in the affirmative. A majority of the participants, 63 (92.6%) would not reveal their status to anyone or seek treatment if they tested positive for HIV. In discussion, the reason cited by many was the fear of being mistreated or discriminated against by people. 66 (97.1%) believed that HIV was a punishment from God, as being infected with HIV was associated with sexual promiscuity and sin. Findings from post-test questionnaire Knowledge of HIV and AIDS There was a significant increase in knowledge levels as observed in the post-test results. At the end of the programme in both cities, 67 (98.5%) participants reported that they knew how HIV was transmitted, indicating a significantly higher proportion of participants who knew how the infection was transmitted (chi-square=9.14,p=0.002). As participants were not able to get tested during the sessions, there was no difference in the number of young women who did not know their serostatus, 64 (94.1%). However, the participants were given information on places to get tested and as a result there was a 100% response rate on knowledge of places to get tested from the participants at the end of the programme. The number of participants who believed that PLWHA always looked sick and thin declined. Of the participants, 26 (38.2%) still held on to this notion even after the programme. A review of the data, revealed that these young women who believed this constituted the number of participants who already knew people who were living with HIV/AIDS, knowledge which may have informed their beliefs even after the programme ended. A hands-on involvement in condom demonstration by the participants increased their knowledge on condom use. 41 (60.3%) participants knew how to put on a male condom correctly by the end of the programme. There was also a decrease in number of young women who held a fatalistic view of HIV infection, where 45 (66.2%) participants still believed that acquiring HIV/AIDS meant the end of one's life by the end the programme. Attitudes towards HIV and people living with HIV/AIDS (PLWHA) There were varied responses by the end of the programme when it came to questions that related to attitudes towards HIV/AIDS and PLWHA. While there were significantly fewer participants 63 (92.7%) who, if in the situation, would not let their children attend the same school with other children who are infected with HIV, only 10 (14.7%) participants still refused to associate themselves with people who they knew were living with HIV/AIDS. There was also a wide gap between pre-and post-test results when it came to the number of people, 12 (17.6%) who believed HIV was a punishment from God. 57 (83.8%) would still not reveal their status or seek treatment if they tested positive for HIV. The difference between pre- and post-test results were not statistically significant (chi-square=2.55, p=0.11). In verbal discussions with some of the participants in regards to this question, a few responded that they were afraid of rejection from their friends and families if they did so. Stigma is still clearly an issue that needs to be addressed. More than half of the participants, 52 (76.5%) would still not go to be tested for HIV because of fear of knowing the results. In verbal discussions with some of the participants at the end of the programme who did agree to get tested, a few responded by giving the reason being that they had a new understanding of how HIV was transmitted and felt confident that they had not been involved in behaviour that would have put them at risk of contracting HIV. Overall, a significant reduction in the misconception about HIV and AIDS among programme participants and an increase in knowledge of HIV/AIDS and sexual health which helped to foster positive attitudes towards PLWHA was observed. The young women reported that with the new information, they would be less likely to avoid people living with HIV and be more compassionate towards them. There was also an increase in the perception of personal risk. The young women were empowered to own their bodies realizing that the power to prevent HIV laid within them. Participants expressed overall satisfaction with the content of the programmes and appreciated this avenue of social support. A sample of post-session responses is given below: "I will surely appreciate it if this kind of lecture is done more often to create more awareness on both HIV/AIDS and sex education" "This is one of the most outstanding programmes I have ever seen or attended. I just wish it would be done on a larger scale as a lot of women out there need this information" "This programme has really helped to shed more light on so many things that are unknown or hidden to ladies. It has helped to bring ladies together, to know our rights and so many things in a relationship" "This was splendid. I loved this programme. I wish it could go on and on. I was naïve about HIV, but now I can go out and educate others" Lessons Learned HIV is beginning to have a face among young Nigerian women, however, stigma is still an issue that needs to be addressed among this age cohort. In creating HIV prevention programmes, it is very important to address negative attitudes and dispel misconceptions about HIV and AIDS in order for people to fully accept the messages. It has been recognized that HIV and AIDS related stigma is determined by pre-existing notions of contagion, infection, the incurable and the inevitably fatal nature of the disease. 9 It was apparent from the test outcomes, that a large majority of the young women embraced these notions. The issue of stigma and discrimination initially served as a barrier in delivering messages. However, the young women were soon receptive when they realized that although HIV is indeed infectious, it cannot be acquired by shaking the hands of a PLWHA or sharing the same plate, spoon or cup; and while it is incurable, it can be managed and controlled and will not result in a death sentence when proper treatment is given. One of the young women, a PLWHA, who attended the programme in both cities boldly revealed her serostatus to the rest of the programme participants on her own volition prior to the distribution of the post-test questionnaires. This not only reduced the rate of participants who did not personally know someone living with HIV at the end of the sessions (see table 1), but it helped reduce the stereotype associated with PLWHA. The young woman served as an example of someone who even though living with HIV, was still able to live a positive and active life while achieving her goals. None of the participants who were able to witness this revelation would have believed that she was a PLWHA if she had not revealed her serostatus. A study that was undertaken in Uganda found that revealing one's seropositive status in some cases helped reduce stigma associated with the disease. 6 A continuous effort needs to be made to provide a safe context under which young women who are living with HIV/AIDS are able to reveal their status without the fear of judgment or discrimination, and to help in reducing the stigma related to HIV and AIDS. An association between education levels and knowledge of HIV/AIDS and sexual health was observed among the participants. In the population of women that participated in the programme in both cities, it was observed that there was a faster rate of response to questions among the relatively older women in tertiary institutions than those in secondary institutions, and discussions on topics relating to sexual health and HIV/AIDS were better engaged by the older women as well. This is consistent with studies which revealed an inverse correlation with educational levels and HIV vulnerability, where the higher the level of education, the greater the potential for decreasing HIV vulnerability.7,8 It has been concluded that although the education of girls and young women may be initially linked to higher HIV vulnerability, this trend tends to change over time as more educated women have the ability to actively engage the epidemic 7, which may eventually lead to lower HIV incidence rates. A large majority of the young women who attended the programmes had never been exposed to this type of knowledge and expressed their desire to educate other young women in their respective schools and religious institutions. It was important to promote this attitude, as this reinforces the importance of peer training in HIV prevention strategies targeted at young people. Findings from the evaluation of the West African Youth Initiative (WAYI) in Nigeria and Ghana concluded that peer education was most effective at improving knowledge and promoting attitudinal and behavioural changes.9 It is important that HIV prevention pro-grammes are targeted towards young Nigerian women in their early adolescent years, as data reveals that young women are exposed to sexual behavioural practices at a relatively young age and may not be correctly informed about their sexuality, HIV and other sexually transmitted diseases. Recent statistics indicate the percentage of 15-19 year-old Nigerian youth who have had sex before the age of 15 at 20.3% in females as opposed to 7.9% in males.1 In addition, the percentage of young Nigerian women and men between the ages of 15-24 years who reported condom use during their last sexual encounter with a non-regular partner was 46% in males compared to the low rate of 24% in females.1 Conclusion and Recommendations HIV/AIDS programmes, when appropriately designed and implemented, have the potential to increase HIV knowledge levels and enable attitudes that have the potential to effect positive behavioural change. In creating comprehensive programmes for young women in Nigeria, it will be important for the government, NGOs, civil societies and other interested bodies to integrate HIV/AIDS into reproductive health services. The integration of services will allow young women to learn about HIV and AIDS, while being provided with the opportunity for testing and counselling services as they make other reproductive health decisions. New leadership should be encouraged among young women living with and without HIV/AIDS in both urban and rural areas to advance the response, by involving them in the development and implementation of HIV prevention strategies and life skills education targeted towards young women. Acknowledgement The HIV/AIDS programme for young women was made possible through the support provided by the Public Affairs Section of the US-Consulate General, Lagos where the author worked as an intern. The opinions expressed herein are those of the author and do not necessarily reflect the views of the US Consulate General, Lagos. References
© Copyright 2007 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh07025t2.jpg] [rh07025t1.jpg] [rh07025t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}