
|
African Journal of Reproductive Health
Women's Health and Action Research Centre
ISSN: 1118-4841
Vol. 11, Num. 3, 2007, pp. 18-27
|
Untitled Document
African Journal of Reproductive Health, Vol. 11, No. 3, December, 2007,
pp. 18-27
Improving Health, Improving Lives: Impact of the African
Youth Alliance and New Opportunities for Programmes
Ugochi Daniels
Africa Division, United Nations Population Fund, New York, NY, United States daniels@unfpa.org
Code Number: rh07032
Abstract
The African Youth Alliance (AYA) was a partnership to improve adolescent sexual and reproductive health, and prevent HIV/AIDS in Botswana, Ghana, Tanzania and Uganda. The AYA model was a comprehensive range of integrated interventions, implemented concurrently and at scale using a multi-sectoral approach. AYA was funded for five years (2000-2005) with $56.7 million from the Bill and Melinda Gates Foundation. Over 35,000,000 stakeholders were reached through media campaigns, almost 400,000 young people received Life Planning Skills training, and over 2,500,000 visits were made by young people to static clinics and outreach services.
A post-test evaluation was conducted by John Snow Inc. (JSI) in 2006 and combined case-control and self-reported exposure design. Case-control design data were analyzed using Propensity Score Matching (PSM), and the Self-Reported Exposure design data were analyzed using PSM and Instrumental Variable (two-stage regression) (IV). The results show AYA's significant and positive treatment effects on sexual knowledge, attitudes, and behaviours. The research suggests a comprehensive, multi-component approach such as AYA's can be effective in improving some key ASRH variables.
Key Words: African Youth Alliance, programmes, young people, impact
Introduction
Various global committments to decrease prevalence of HIV among young people focus on increasing young people's access to core interven-tions for the prevention of HIV, as well as decreasing their vulnerability to HIV/AIDS. A global consultation held in Tailloires, France, May 20041 concluded that young people remain at the centre of the HIV/AIDS pandemic in terms of transmission, vulnerability, impact and potential for change. Prevention works, but interventions need to be taken to a scale capable of halting and reversing the pandemic. Though progress is being made, we are still far from achieving 2010 and 2015 global targets. From Tailloires, we know that effective, practical and doable interventions exist.
In 2005, world leaders recognized that achieving the Millennium Development Goals requires achieving universal access to reproductive health. We also recognize that we urgently need to link our HIV/AIDS efforts with sexual and reproductive health. Based on the experience and results from multi-country programmes for young people, lessons have been learned that provide ideal opportunities to scale up SRH and HIV prevention programmes for young people.
Multi-country Programmes for Young People: An Overview of AYA
The African Youth Alliance (AYA) was a partnership of the United Nations Population Fund (UNFPA), PATH, and Pathfinder International (PI) with the goal to improve adolescent sexual and reproductive health (ASRH), including the prevention of HIV/AIDS, among young people aged 10-24. The AYA programme was implemented in four countries — Botswana, Ghana, Tanzania and Uganda — in partnership with their governments, non-
governmental organizations (NGOs),
community -based organizations (CBOs), and key
stakeholders including: youth, parents, religious leaders,
the media and policy makers.
To accomplish AYA's goal, six programme components were developed using evidence-based strategies:
- Policy and Advocacy (P&A)
- Behaviour Change Communication (BCC)
- Youth Friendly Services (YFS)
- Integration of ASRH into Livelihood Programmes
- Institutional Capacity Building (ICB)
- Coordination and Dissemination (C&D)
AYA also integrated partnerships, youth participation, gender equity, sustainability, scaling up, and community involvement in each component. At the country level, programme components and crosscutting objectives were adapted to meet the specific needs and context. AYA developed a results framework that guided programme planning, implementation, monitoring and evaluation. Using various country-specific approaches, youth were involved and played a significant role in all stages of the AYA programme.
The AYA model was designed as a compre-hensive range of integrated interventions, implemented concurrently and at scale using a multi-sectoral approach. Funded for five years (2000-2005) with US $56.7 million from the Bill and Melinda Gates Foundation as "venture capital", AYA was an unprecedented innovation to implement this model and build the capacity required for governments and other development agencies to sustain and scale up SRH and HIV prevention interventions for young people.
Summary of Results
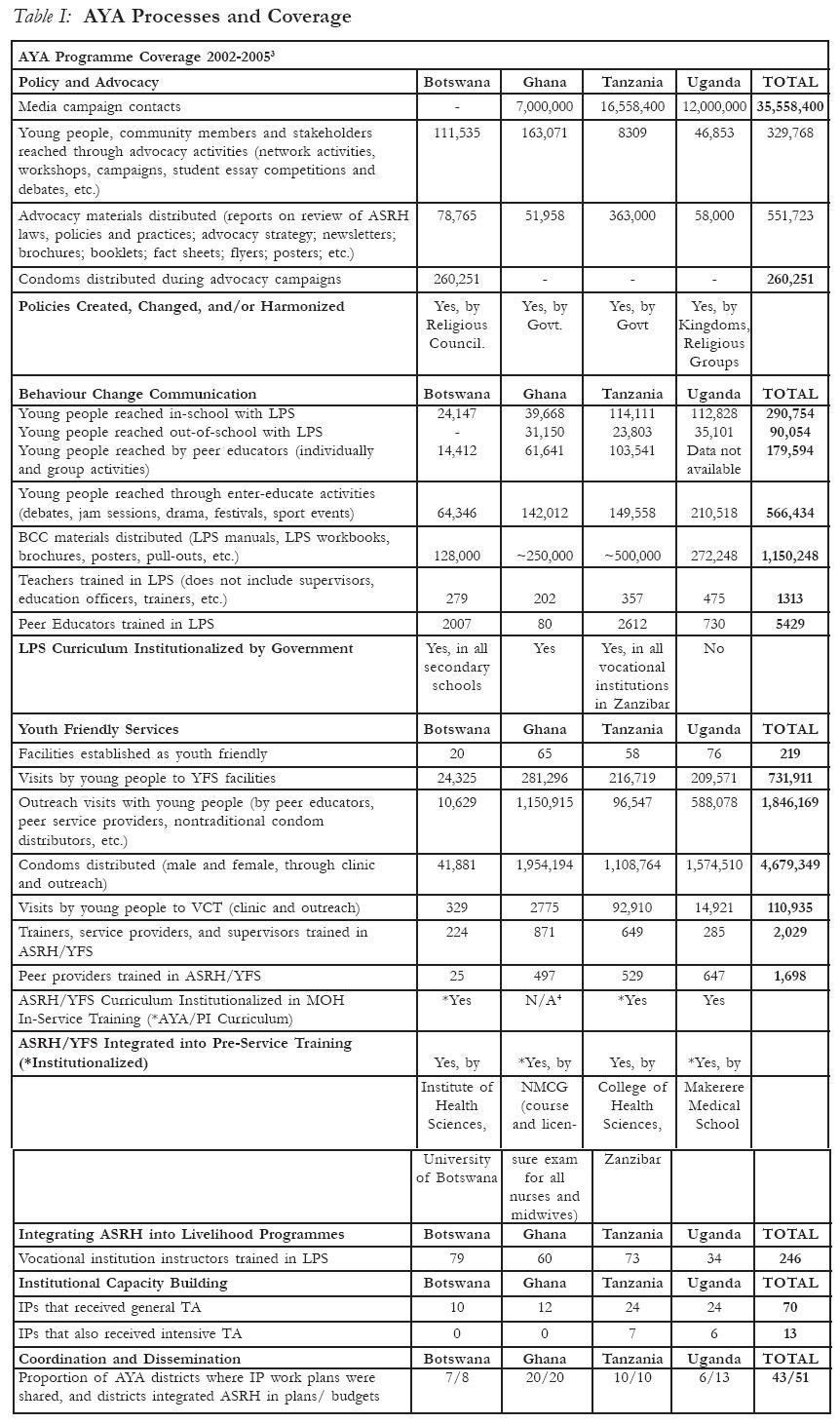
I. Programme Coverage1: Who did AYA Reach?
Fundamental in the delivery of AYA model, was ensuring that young people (and key stakeholders) were reached with consistent messages, multiple times, using multiple approaches, in multiple settings. Over 35,000,000 stakeholders were reached through media campaigns, almost 400,000 young people received Life Planning Skills training, over 2,500,000 visits were made by young people to static clinics and outreach services. Table
I summarizes AYA's process results and reach of the programme.
II. AYA Outputs: What were the programme components and outputs achieved?
The AYA programme was made up of six components which were evaluated in 2005-2006. Evaluations show significant improvements in antecedents of behaviour changes as well as improved capacity to enable behaviour change[FNA]:
• Policy and Advocacy (P&A): was designed to improve the legal and policy environment by assuring implementation of supportive ASRH policies in order to successfully carry out AYA interventions. The longer-term objective was to create a sustainable, enabling environment for ongoing work in ASRH.
An evaluation of the P&A component found improved knowledge and supportive attitudes of stakeholders, an increase in commitments and actions supportive of ASRH by stakeholders, and increased resource allocation for ASRH.
• Behaviour Change Communication (BCC): aimed
to enable and sustain healthy behaviour adoption by building the necessary
skills of young people. The implementation of Life Planning Skills (LPS) training
with
both in- and out-of-school young people was a cornerstone of the component. Evaluations and process data from this component demonstrated improvements in ASRH knowledge, perceptions, attitudes and behaviours among students who received LPS training.
• Youth Friendly Services (YFS): made services youth-friendly and available to young people, and set the stage for scaling up. AYA worked with public health facilities, NGOs and FBOs to improve quality of services for young people, through both static clinic facilities and outreach. Component evaluations determined that the availability of YFS increased, the quality of and client satisfaction with YFS improved and utilization of YFS increased. In all AYA countries, ASRH/YFS was integrated in pre-service training.
• Integrating ASRH into Livelihood Programmes[FNB]: supported
the integration of ASRH activities into existing livelihood programmes for
young people, and advoca-ted for increased recognition and funding for livelihood
programming. And, importantly, LPS was mandated in the Zanzibar Vocational Education Policy in Tanzania.
• Institutional Capacity Building (ICB): provided technical or material assistance to strengthen one or more elements of organi-zational effectiveness, with the aim of overall sustainability. The evaluation showed improvements by Implementing Partners in each country, and several have secured funding to sustain ASRH programming.
• Coordination and Dissemination (C&D): ensured effective implementation and integration of programme components within AYA, as well as externally within government and other important programmes. Government structures were supported to ultimately assume this coordination. The
evaluation determined that improvements were made in each country: IP work plans were shared, networking and collaboration among implementing partners and district coordination offices occurred at all levels through various channels, and youth participation increased.
III. AYA's Impact: Did programme objectives collectively achieve Behaviour Change?:
In 2005, John Snow, Inc. was engaged by The Bill and Melinda Gates Foundation to conduct an independent impact evaluation of the effect of exposure to AYA programmes on ASRH behaviours. The essential research question was:
Among sexually active 17 to 22 year olds, are those who report exposure to AYA more likely to:
- use condoms
- have fewer sexual partners
- use modern contraceptives,
- abstain from sex or delay first intercourse than those not exposed
to AYA? 2-4
The evaluation was post-test only, and combined case-control
and self-reported exposure design. Data was collected from early March through
the beginning of June 2006 by local research organizations, using a one-stage
(Tanzania) or two-stage (Ghana, Uganda) cluster sampling (cases and controls
(purposive), random selection of segments, and random selection (or census)
of households within segments)2. Household, individual and community questionnaires were applied. Case-control design data were analyzed using Propensity Score Matching (PSM), and the Self-Reported Exposure design data were analyzed using PSM and Instrumental Variable (two-stage regression) (IV).
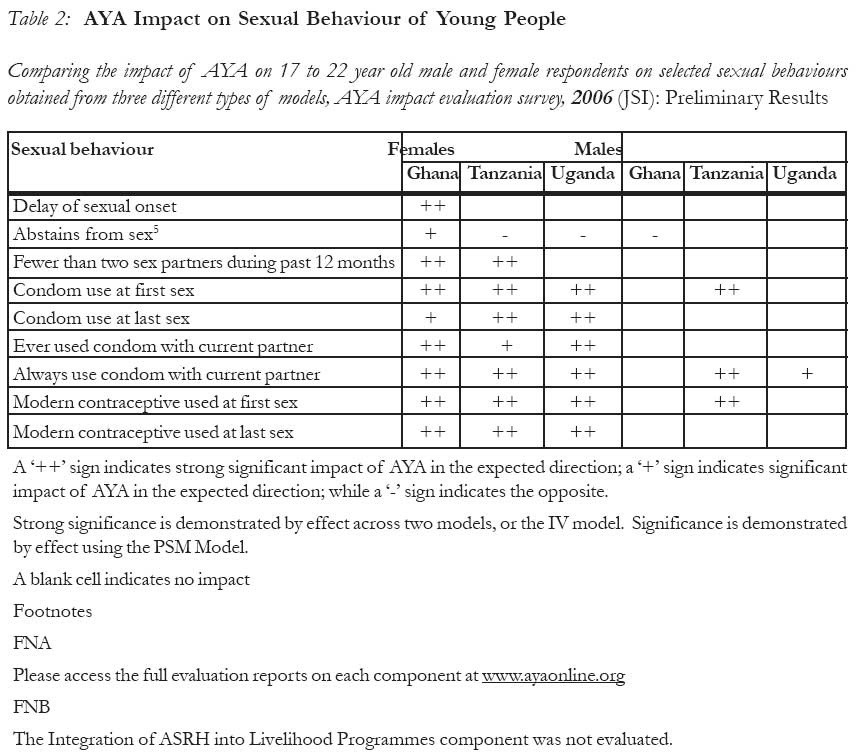
Results of the impact evaluation (Table
2) indicate evidence of significant, positive AYA treatment effects on sexual knowledge, attitudes, and behaviours. Across all three AYA countries evaluated, there were more treatment effects for females; and, among sexually active females, there were significant positive effects on: condom use at first sex, always use condom with current partner, and modern contraceptive use at first and last sex.
JSI concludes that the research suggests a comprehensive, multi-component approach such as AYA's can be effective in improving some key ASRH variables.
IV. Implications: Why are these results important?:
AYA as a programme was an unprecedented innovation to implement a multi-sectoral model and build the capacity required for government and her development partners to sustain and scale up SRH and HIV prevention programmes for young people. These results demonstrate the model's success at achieving behaviour change among young people reached by the programme and that the model has contributed to an enabling and sustainable programme environment that will continue to support ASRH programming.
Therefore these outcomes are significant for a number of reasons:
- Given youth demographics and the epidemiology of HIV in sub-Saharan
Africa where young people constitute 30% of the population but represent
50% of new infections, evidence of successful approaches are vital. No other
programme in the region has been able to demonstrate efficacy at a similar
scale.
- These results validate the level of investment in a
programme for young people. In 2000, AYA represented the biggest investment
ever made in ASRH programming.
- These results, and documentation on pro-gramme strategies and experiences
are valuable resources to achieve high impact programming (particularly amongst
females) as well as areas for improvement.
- Developing a good quality, cost effective evaluation methodology for multi-country, multi-component, multi-partner pro-grammes, can be a major challenge. In such programmes, there is often great variability from site to site, the problem of identifying controls with so many other similar or related programmes ongoing as well as data from baseline surveys conducted at the beginning of the programme that are no longer applicable by the time of the endline survey. The evaluation of AYA has provided the field with a methodology for evaluation that responds to the practical challenges of programming in the "real world".
- The results provide evidence to support advocacy and resource mobilization
for SRH and HIV prevention programmes for young people. A lack of evidence
has been a real stumbling block in raising the visibility of the SRH needs
and rights of young people.
IV. Challenges
- The impressive impact of AYA on females was not equally demonstrated
in males. A review of the process data has shown that overall males and females
were reached equally by the programme, though there is some variance by strategy,
and that programme messages did not specifically target females at the expense
of males. Further qualitative research is necessary to better understand
the social context of behavior change in young males. Anecdotal evidence
seems to indicate that the duration, intensity, content and approach of programme
interventions to achieve behavioral change in males and females varies greatly.
- Establishing a partnership first at the international level and
then at the national level with over sixty partners required significant
time and investment in the development of systems and procedures.
- The initial expectation was that the pro-gramme could immediately
go to scale, but this was based on the assumption that effective models and
capacity were available. The reality proved otherwise, and significant investment
had to be made to build and strengthen the capacity required to support replication
and expansion.
- AYA did not address the issue of costing until midway into the programme.
At that point, the emphasis was reaching young people and scaling up given
the significant amount of time that had already been devoted to establishing
the partnership and building the capacity for scale up of interventions.
Unavailability of costing data has hampered advocacy for scale up.
- During the programme, shortage of RH supplies (e.g., condoms, VCT
kits) was a constant challenge. Once young people and their communities had
been mobilized and demand generated, the resulting increase in clientele
often led to stock outs. Commodity supply and logistics are often not a component
of ASRH programmes.
- Delivering the multi-sectoral response requires simultaneous implementation
of a compre-hensive range of interventions. Achieving integration (across
components) is a major challenge as the natural inclination is for partners
to focus on their specific components.
- While there was improved data collection and reporting (especially
by service organizations), consistent and comprehensive data collection and
reporting were constant challenges.
- It is important to recognize that monitoring and evaluating
the AYA model was an intensive effort that included designing and conducting
baseline data collection; conducting Participatory Learning Activities; developing
a comprehensive M&E Plan to monitor goals, programme objectives, crosscutting objectives and processes; constituting and convening an M&E Technical Advisory Committee; developing monitoring tools and guidelines; building capacity to implement the M&E
Plan; conducting a Mid-term Assessment; conducting evaluation of programme
components; assessing crosscutting objectives; designing and implementing
an evaluation strategy; and documenting and disseminating results. To compound
these processes further, there was also the need to build consensus and implement
these activities with a broad spectrum of partners. These activities were
neither
planned nor budgeted for at the design phase and the level of effort required
was grossly underestimated.
- Though sustainability was an AYA cross-cutting objective and a strategy
was developed to ensure sustainability of interventions, actually operationalizing
this concept was difficult. It was necessary to develop an exit strategy
and ensure participatory and coordinated close out of programme interventions.
However AYA only started this in the fourth year of the programme when there
were also many other competing interests that equally had to be addressed
as the programme was drawing to a close. At the same time, AYA was facing
staff attrition as staff secured other positions.
IV. Lessons Learned and Recommenda-tions: How can we improve our programmes?
Given AYA's achievements, challenges faced, and insights gained in designing and implementing a complex, multi-sectoral programme, there were common lessons learned across countries. The following recommendations are offered for consideration:
Planning
- Defining the structure, relationships, operating procedures and
a plan for integration for a large, multi-sectoral programme are important
key, early tasks to lay a firm programme foundation. It is critical that
roles, responsibilities, systems and procedures are detailed, well understood
and accepted. It is necessary to clearly designate oversight and accountability
for individual programme components as well as their integration. Strong
coordinating mechanisms and networking are needed for large partnerships.
- Do not underestimate the significant amount of time needed to deploy
a multi-sectoral partnership in which multiple stakeholders are involved,
ownership is encouraged, and capacities built before effective outcomes can
be expected. This is especially true if sustainability and scaling up are
to be achieved.
- At programme inception, plan for and prepare at programme inception
good evaluation design as part of an overall results-based management strategy,
then assure adequate funding and human resources upfront.
- Plan for the end at the beginning: sustainability should be addressed
for as early as possible, including building programme activities into ongoing
institutions, so that an effective transfer of programme responsibilities
can occur when a time-funded programme is scheduled to terminate support.
- Ensure that the phasing out of the programme is well planned, effectively
communicated and participatory. Engage stakeholders and partners in strategic
planning for a comprehensive exit strategy and for future efforts beyond
the life of the programme.
Implementation
- Integration is key to increasing programme impact:
AYA improved health-seeking behaviour: Percentages of young people who in the
past 12 months went to a health facility to receive information and services
increased in all countries. Integration of the P&A, BCC and YFS components
improved knowledge, skills and attitudes of young people as well as the availability
and quality of health services. Advocacy work improved knowledge and attitudes
of community members. Ultimately, utilization of services by both males and
females increased. Determine which components can be integrated from the
start, recognizing that not all components can be integrated before they
are operational.
- Quality data for trend analysis and evaluation remain difficult
to obtain from clinic staff and outreach volunteers. Standardized collection
instruments must be implemented and data collectors must be recruited and
trained: lack of dependable data can compromise use of data for planned expansion
and scaling up.
- Focus must be maintained at both the national level to ensure sustained
commitment and support, and at the district/village level to ensure implementation.
Promote national government structures that address ASRH at the district
and community level to facilitate comprehensive and complementary approaches
that districts and communities can sustain and own.
Programme Components
- In AYA, condom messages effectively resulted in increased use (ever
and at last sex) and intent to use. Given their ease of use, that they are
the identified method of preference by adolescents, their effectiveness for
both pregnancy and HIV/STI prevention, and recognizing mixed results with
abstinence messages, condoms should be a fundamental element of SRH services
for young people. AYA's experience reaffirms this lesson consistently learned
in ASRH programmes.
- ASRH interventions must be customized for
distinct groups of adolescents. Evidence from all the evaluations consistently
underscores the heterogeneity of youth—programme interventions affected
segments of the target population differently. Data across all countries
showed that more females visited clinics for counselling, more males obtained
condoms
through outreach. In-school evaluations of the LPS curriculum found that
for young people in primary school the most significant change was in condom
knowledge
and intent to use, whereas for those in secondary school the most significant
change was in building healthy relationships, confidence to refuse sex
and negotiating condom use. The JSI impact evaluations demonstrated more
positive
effects on outcomes for females. Lack of impact on 17-22 year olds with
regard to abstinence, underscores the importance of targeting abstinence
messages
to 10-14 year olds who are still forming behaviours.
Crosscutting Objectives
- There are two significant components to scaling up programmes: establishing
the capacity to support a large-scale programme and replication of effective
models. AYA found many talented organizations committed to implementing ASRH
interventions; however, in order for the organizations to reach large numbers
of youth, substantial capacity building was necessary.
- Scaling up requires that fundamentals must be addressed before actual
expansion occurs; these include identification of effective models, formation
of enabling policies, preparation of a capable infrastructure and capacity
to implement, and institutionalization of tools and strategies. Be prepared
to devote required resources to first achieve this and to sustain it.
- Youth participation, sustainability, scaling up,
partnerships, community involvement and gender sensitivity are typical principles
of ASRH programmes. Success at achieving these requires operational modalities
to ensure effective implementation as well as measurement systems to demonstrate
the contribution to programme outcomes.
The AYA Legacy: Conclusions and Opportunities
AYA's legacy is both behaviour change in the young people reached directly by the programme and the enabling and sustainable programme environment that continues to support sexual and reproductive health programming for young people in the four AYA countries.
The AYA experience benefits the larger sexual and reproductive health field; demonstrates efficacy of the model for donors and pro-grammers; provides best practices that ASRH programmers can collectively address; provides a tested methodology for evaluation; and affords specific lessons learned for both technical programme components and for managing each stage of the programming process.
Scaling up the multi-sectoral approach would include:
- Replication of the model to improve determinants and achieve behaviour
change, maintaining a strong gender focus on girls' empowerment and increasing
emphasis on male responsibility and involvement;
- Further study of the context of and motivation for behaviour change
among young people, particularly males;
- Study of the impact on abstinence; delay of sexual debut and negotiation
skills and very young adolescents (10-14 year olds);
- Support to national and district governments to improve institutional
and technical capacity to deliver and sustain good quality progra-mmes for
young people;
- Advocacy to both national governments and district councils, as
well as community-based advocacy to guarantee implementation of national
policies at the district, local government and community level;
- Dissemination and capacity building for programme staff to ensure
integration of the approach and improve the quality and effectiveness of
the programmes.
AYA's contribution will continue to benefit the lives of young people in Africa for many years to come. As civil society and government work to eradicate poverty and hunger, improvements in the health of young people will remain a fundamental strategy for youth empowerment, well-being and overall development. The effort and experience of the African Youth Alliance will help to position ASRH as a key strategy in the achievement of Millennium Goals, the corner-stone of collective global development efforts.
1 Please access the programme component evaluation
reports for full details on the data including disaggregation by age and sex
at www.ayaonline.org.
2Botswana was not included in the evaluation due to budget constraints.
3Time periods for activity implementation vary
and in some cases are as short as 1.5 years; in addition, not all programme
sites (e.g. schools, clinics, group events) reported consistently or completely.
Results should be viewed for a general sense of scope rather than as specific
numerical achievements under standardized conditions.
4The government of Ghana had already developed
and adopted an in-service training curriculum on adolescent health prior to
AYA.
Reference
- World Health Organization, UNAIDS Inter-Agency Task Team on Young Peo. Steady... Ready...Go! The Talloires consultation to review the evidence for policies and programmes to achieve the global goals on young people and HIV/AIDS 2004.
- JSI Research & Training Institute. Results of an Evaluation of the African Youth Alliance program in Ghana: Impact on Youth People's Sexual and Reproductive Health.
Arlington, VA: JSI Research & Training Institute, 2007.
- JSI Research & Training Institute. Results of an Evaluation of the African Youth Alliance program in Tanzania: Impact on Youth People's Sexual and Reproductive Health.
Arlington, VA: JSI Research & Training Institute, 2007.
- JSI Research & Training Institute. Results of an Evaluation of the African Youth Alliance program in Uganda: Impact on Youth People's Sexual and Reproductive Health.
Arlington, VA: JSI Research & Training Institute, 2007.
© Copyright 2007 - Women's Health and Action Research Centre
The following images related to this document are available:
Photo images
[rh07032t2.jpg]
[rh07032t1.jpg]
|

{kind=link}
{kind=link}