 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 11, No. 3, December, 2007, pp. 28-43 Sexual Behavior, Knowledge and Information Sources of Very Young Adolescents in Four Sub-Saharan African Countries Akinrinola Bankole1, Ann Biddlecom1, Georges Guiella2, Susheela Singh1, Eliya Zulu3 1The Guttmacher Institute, New York, New York,
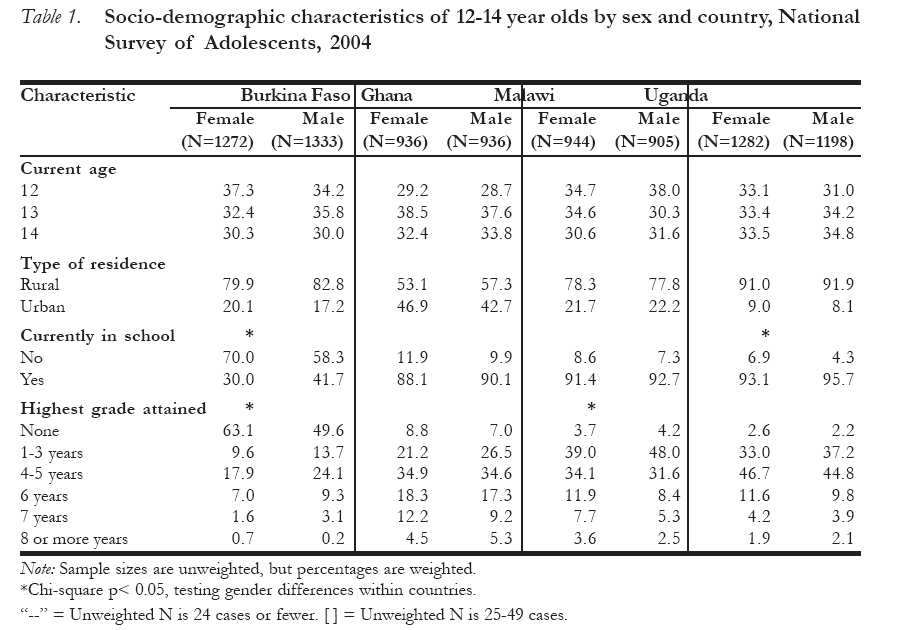
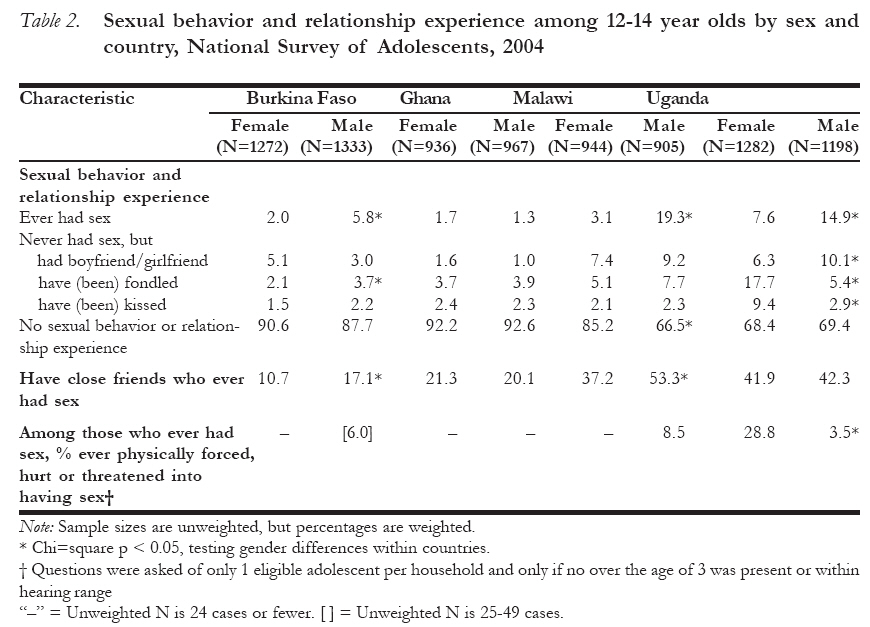
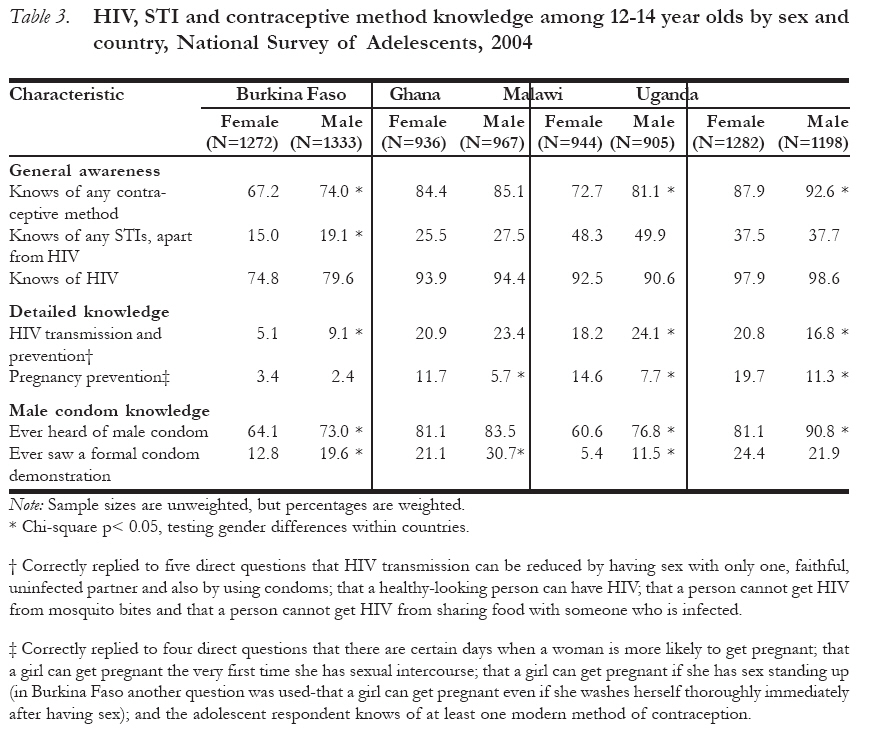
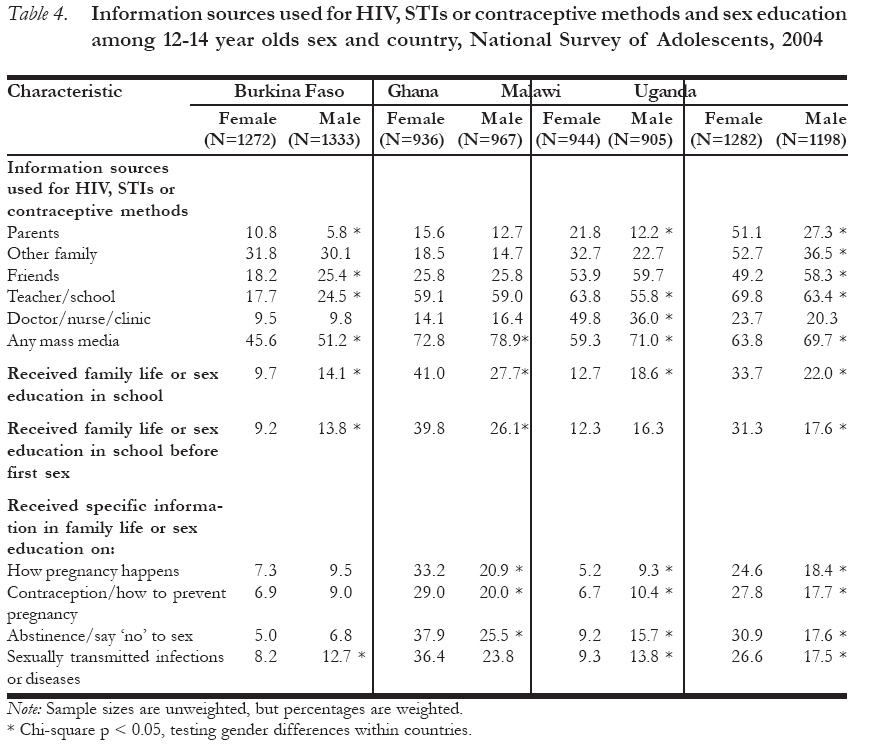
United States Code Number: rh07033 Abstract Adolescents are a key target group for HIV and pregnancy prevention efforts, yet very little is known about the youngest adolescents: those under age 15. New survey data from 12-14 year olds in Burkina Faso, Ghana, Malawi and Uganda are used to describe their sexual activity, knowledge about HIV, STIs and pregnancy prevention, and sources of sexual and reproductive health information, including sex education in schools. Results show that very young adolescents are already beginning to be sexually active and many believe their close friends are sexually active. They have high levels of awareness but little in-depth knowledge about pregnancy and HIV prevention. Multiple information sources are used and preferred by very young adolescents. Given their needs for HIV, STI and pregnancy prevention information that is specific and practical and considering that the large majority are attending school in most countries in Sub-Saharan Africa, school-based sex education is a particularly promising avenue for reaching adolescents under age 15. Résumé Comportement sexuel, sources de la connaissance et de l'information de très jeunes adolescents dans quatre pays subsahariens Les adolescents constituent un groupe cible clé pour les tentatives de la prévention du VIH et de la grossesse, pourtant on a très peu de renseignements concernant les plus jeunes adolescents: ceux qui n'ont pas encore quinze ans. De nouvelles données d'une enquête recueillies auprès des jeunes âgés de 12-14 ans au Burkina-Faso, au Ghana, au Malawi et en Ouganda ont été utilisées pour décrire leur activité sexuelle, leur connaissance au sujet du VIH, IST et la prévention de la grossesse, les sources des renseignements sur la santé sexuelle et de reproduction, y compris l'éducation sexuelle à l'école. Les résultats ont montré que les très jeunes adolescents commencent déjà à être sexuellement actifs et beaucoup d'entre eux croient que leurs amis proches sont sexuellement actifs. Leurs niveaux de conscience sont élevés, mais ils n'ont pas assez de connaissance en profondeur de la prévention de la grossesse et du VIH. De très jeunes adolescents se servent et préfèrent des sources multiples d'information. Vu leur besoin pour les renseignements spécifiques et pratiques sur la prévention du VIH, des IST et de la grossesse et si l'on considère que la grande majorité fréquentent encore l'école dans la plupart des pays en Afrique subsaharienne, l'éducation sexuelle qui est basée sur l'école constitue surtout une voie par laquelle on peut atteindre les adolescents âgés de moins de 15 ans. Key Words: Very young adolescents, sexual behaviour, reproductive health, sex education, sub-Saharan Africa Introduction Adolescent sexual and reproductive health is a critically important policy and programmatic issue in Sub-Saharan Africa given the generalized AIDS epidemic that has taken hold in many countries as well as a persistently high level of adolescent childbearing. An estimated 4.3% of young women and 1.5% of young men aged 15-24 years in Sub-Saharan Africa were living with HIV at the end of 20051 and 9-13% of young women had given birth by age 162. Clearly, young people need access to protective information and skills before they become sexually-active in order to reduce their risk of contracting HIV and other sexually transmitted infections (STIs), and of experiencing unintended pregnancies and very early childbearing. The key challenge is to determine what specific information to give very young adolescents, from what sources, at what ages and in what ways. One of the first steps in addressing these questions is to understand what are the current sexual and reproductive health behaviors and needs of very young adolescents. While the literature is replete with studies of the sexual and reproductive health of older adolescents and young adults—those age 15-24 years—the evidence on very young adolescents is quite sparse.3 The focus on the 15-24 age group has mostly been driven by availability of nationally representative data collected by the Demographic and Health Survey program, which typically collects sexual and reproductive health data for women aged 15-49 and men aged 15-59, but does not include very young adolescents. This study fills this gap by presenting new, national evidence on the sexual behavior, knowledge and information sources of very young adolescents (12-14 years old) in four countries across Sub-Saharan Africa: Burkina Faso, Ghana, Malawi and Uganda. Early adolescence is an important stage in which to intervene for several reasons, even if a majority of young people have not yet had sexual intercourse. First, sexual maturation begins at this time: 17-31% of 12-14 year old girls reported that they had experienced their first menstruation and the median age at first menstruation ranged between 14.6 and 15.3 years across the four countries (among 12-19 year olds).4-7 (Table 4.1) While boys do not experience a distinct event during puberty like menstruation, 17% of 12-14 year-olds in Burkina Faso, 30% in Ghana, 32% in Uganda and 37% in Malawi said they had experienced pubic hair growth, deepening of the voice or nocturnal emissions ("wet dreams").4-7 Second, early adolescence is one of the easier stages in life in which to reach a large number of young people given that many are still in school. Among those aged 10-14 years, 66% of boys and 58% of girls in Western/Middle Africa and 74% of boys and 71% of girls in Eastern/Southern Africa were currently attending school: these high levels of attendance mean that the school is well placed to provide information on sexual and reproductive health to young adolescents, and as the gender gap in school participation has been narrowing over time, it is a good avenue to reach both boys and girls.2(Table 3.1 p.73) Given that there are few other ways to efficiently reach a large number of very young adolescents about health-related issues, school-based programs—especially those at the primary school level—are promising.8 [FN A] Even in countries where school attendance is relatively low (e.g. in Burkina Faso where half of boys and nearly two thirds of girls aged 12-14 had never been to school)5 (Table 3.4) or where there is a significant drop in school attendance in the later teen years, a substantial proportion of young adolescents can still be reached in the school system at the primary level. In addition, school attendance is likely to continue to increase over time. Finally, though only a minority of young adolescents has initiated sexual intercourse, their sexual curiosity and intimate relationships have likely begun. In addition, in Sub-Saharan Africa, most young adolescents will make this transition during their teenage years: the initiation of sexual activity increases steadily between ages 15 and 19, with about three-quarters of women and close to two-thirds of men initiating intercourse before age 20.2(Table 4.5) Given the importance of intervening before adolescents are at risk of unwanted pregnancy, STIs or HIV,9 policy makers and program designers need to understand young adolescents' behaviors, what they know and do not know in regard to sexual matters, and what their level of access is to sources of sexual and reproductive health information and services. This article fills some of these information gaps, presenting recent information for four Sub-Saharan countries on what very young adolescents are doing sexually, what they know about HIV, STI and pregnancy prevention and from whom they currently get information. Data and methods We use data from nationally-representative household-based surveys of male and female 12-19 year olds. The surveys were conducted in 2004 by the Guttmacher Institute in collaboration with Macro International Inc. and organizations in Burkina Faso (Institut National de la Statistique et de la Démographie), Ghana (Institute of Statistical, Social and Economic Research, University of Ghana), Malawi (National Statistical Office) and Uganda (Uganda Bureau of Statistics). A first-stage systematic selection of enumeration areas was made in each country, and a second stage selection of households within the selected enumeration areas was made from a household listing. All 12-19 year old de facto residents in each sampled household were eligible for inclusion in the survey. Consent from a parent or caretaker was obtained for adolescents aged 12-17 years before the eligible adolescent was approached to participate in the survey. Once the parent or caretaker gave consent, separate informed consent was then sought from the eligible under-age adolescent. For those aged 18-19, consent was obtained directly. This paper analyzes data for the infrequently studied group of very young adolescents aged 12-14. Interviews were completed with 2605 12-14 year olds in Burkina Faso, 1903 in Ghana, 1849 in Malawi and 2480 in Uganda. The eligible adolescent response rate ranged between 91.2% (Malawi) and 96.8% (Burkina Faso) for 12-14 year old females and between 88.3% (Uganda) and 95.5% (Burkina Faso) for 12-14 year old males. Interviews with 12-14 year olds lasted on average 54 minutes across the four countries and followed a protocol of matching the sex of the interviewers to the sex of the respondent. One concern prior to the survey fieldwork was whether 12-14 year olds would not understand or be comfortable with some of the questions asked of them. Item-missing rates and levels of "don't know" responses for behavior questions were relatively low (though generally higher than those for 15-19 year olds).4-7 Interviewers were also asked to rate adolescent respondents' understanding of survey questions, and the percentage of 12-14-year-old respondents rated as understanding questions "not very well" was 11% or less for females and 16% or less for males in all four countries. 4-7 (Table 2.1) Three issues are examined in this paper: sexual behavior; knowledge about pregnancy formation, contraception, and STIs, including HIV; and sources of sexual and reproductive health information. On sexual behavior, sexual intercourse remains one of the most important experiences to document given its direct link to risk of both unwanted pregnancy and HIV and STI infection. In the case of very young adolescents, it is also relevant to assess whether they have experienced sexual behaviors apart from intercourse that may signify the start of sexual interest or curiosity. In the survey, unmarried young adolescents were asked questions about their awareness of specific sexual activities (kissing, fondling and sexual intercourse), whether they knew of any close friends who had experienced these sexual activities, and whether they themselves had ever experienced them. Questions about personal experiences were asked only if respondents reported that they had heard of the relevant sexual activity. The specific question wording in English—though the questionnaire was translated into the major languages of each country—was "Have you ever heard of sexual intercourse? By this I mean a penis in a vagina." Fondling was defined as "By this I mean someone's private parts, breasts or other parts of the body being touched in a sexual way." Kissing was not defined. Questions about whether close friends had experienced each type of sexual activity were asked for two main reasons. First, this measure provides a likely upper estimate of the level of sexual activity among this group, because it is more likely that young adolescents will report about their friends' sexual behavior than about their own. Second, what peers are doing (or at least perceived to be doing) has been shown to be positively associated with what adolescents themselves report because adolescents feel normative pressure to do what they think their friends are doing.10 Relationship experience for those who have never been married was ascertained by a question about whether the respondent had ever had a boyfriend or girlfriend (regardless of sexual intercourse experience). Questions about coercive sex were asked of only one, randomly-chosen eligible adolescent per household in order to further ensure confidentiality of responses since no other interviewed adolescent in household would be aware of the questions asked. The proportion of sexually-experienced 12-14 year-olds who reported that they had been ever physically forced, hurt or threatened into having sex is presented as an indicator of the degree to which self-reported early sexual experience overlaps with coercive sexual experiences. Given the social stigma surrounding sexual activity for very young adolescents, particularly for girls, and given that studies of older adolescents suggest that males tend to over-report sexual experience,11 we do not place much emphasis on gender differences in the self-reports of sexual behavior. Three groups of measures of knowledge among very young adolescents are examined: 1) general awareness of any contraceptive methods, HIV/AIDS, and any STIs apart from HIV; 2) knowledge of the male condom (ever heard of it and whether the respondent had ever seen a condom demonstration); and 3) composite measures of pregnancy and HIV prevention knowledge that combine responses across several items to indicate the depth of adolescents' knowledge. The composite measure of HIV knowledge is a recommended indicator for monitoring and evaluating HIV prevention programs for youth and is based on correct responses to three direct questions about HIV transmission (HIV transmission can be reduced by having sex with only one, faithful, uninfected partner; HIV can be reduced by using condoms; and that a healthy-looking person can have HIV) and rejection of two common misperceptions about HIV (a person can get HIV from mosquito bites and a person can get HIV from sharing food with someone who is infected).10 The composite measure for pregnancy prevention similarly reflects different dimensions of knowledge: knowledge of pregnancy risk and prevention (there are certain days when a woman is more likely to get pregnant and awareness of at least one modern method of contraception), and rejection of two common misperceptions (a girl cannot get pregnant the very first time she has sexual intercourse and she cannot become pregnant if she has sex standing up). Finally, adolescents were also asked questions (without probing) about where they received information about each of the following: methods to prevent pregnancy, HIV/AIDS and STIs. The data are aggregated across all three topics for ease of presentation and because information sources did not vary substantially by topic. A series of questions about sex education or family life education (the phrase used was specific to the country context) were also asked to track adolescents' self-reported exposure to these school-based programs, what major topics were covered and the age when the adolescent first attended such classes or talks. The latter question is used to determine the proportion of adolescents who received sex education prior to becoming sexually-active. A strength of these data is that they provide a much-needed picture of what is taking place "on the ground" with respect to sex education. A weakness is that these are adolescents' self-reports and are susceptible to recall error and bias. All tables show weighted percentages, and data are not shown when denominators are less than 25 unweighted cases. A Pearson ×2 statistic was calculated using STATA 9 (taking into account the stratified, cluster sample design) to test for the association between gender and the relevant measure in order to determine the knowledge areas where either gender is at a particular disadvantage and if there are specific information sources that are more commonly used by either gender category. P values less than .05 are considered statistically significant and are indicated in each table. Results Characteristics of respondents In all four countries, the distributions of very young adolescents are highly similar for males and females, with respect to age, residence, school attendance and highest grade attained (Table 1). In all four countries, there are no significant gender differences in the distribution of very young adolescents aged 12-14; they are almost equally distributed by single year of age. In Burkina Faso, Malawi and Uganda, most very young adolescents reside in rural areas, irrespective of sex: 78% in Malawi, 80-83% in Burkina Faso and 91-92% in Uganda. In Ghana the proportion in urban areas is much higher: 43-47% of very young adolescents. There are no statistically significant differences in type of residence by gender. There are gender differences in school attendance and highest grade attained but not consistently so across all four countries. Most adolescents aged 12-14 (88-96%) were currently in school in Ghana, Malawi and Uganda. In Burkina Faso, the reverse is the case as 70% of females and 58% of males are not currently in school and this difference is statistically significant. There is also a smaller but statistically significant gender difference in Uganda as well where males are more likely to be in school than females. In all four countries, a substantial proportion of 12-14-year-old adolescents have fewer years of schooling than would be expected (based on a typical age of starting school at age six and progressing steadily through primary school). In Ghana, Malawi and Uganda, where the majority of 12-14 year olds have ever attended school, 20% or more have only 1-3 years of schooling, much less than the expected level of exposure to schooling given their age. Those who have 4-5 years of schooling are also somewhat below expectation, and this is a substantial group as well — an additional 32-47% across Ghana, Malawi and Uganda. Only a minority of 12-14 year olds has attained six or more years of school, and there are statistically significant gender differences in the level of schooling attained in Burkina Faso and Malawi. Sexual activity Contrary to what might be generally thought, very young adolescents in these four Sub-Saharan African countries are not all sexually naïve. Almost one-third of 12-14 year old girls and boys in Uganda and boys in Malawi have either experienced some form of intimate sexual activity (sexual intercourse, kissing, fondling or they have had a boyfriend or girlfriend) (Table 2). This proportion is much lower in Burkina Faso and Ghana, but even in these two countries about 1 in 10 very young adolescents have had some sort of intimate sexual activity (ranging between 7-12%). No consistent pattern emerges in terms of a progression from kissing to fondling to sexual intercourse among very young adolescents, but the proportion who have kissed or been kissed is consistently somewhat lower than the proportion who have fondled/been fondled. Very few adolescents reported having ever kissed (ranging from 2% of females in Burkina Faso to 9% among females in Uganda). Slightly higher proportions of adolescents have fondled (ranging from 2% among girls in Burkina Faso to 18% among females in Uganda). Few 12-14 year old females reported that they have ever had sexual intercourse (highest percentage being 8% in Uganda), which is to be expected, given their age and the social stigma attached to sexual intercourse for young, unmarried adolescents. There was more variation among 12-14 year old males, with only 1% in Ghana saying they ever had sex compared to 6% in Burkina Faso, 15% in Uganda and 19% in Malawi. It is important to understand the context within which very young adolescents are becoming sexually active, and to assess the extent to which they are adequately prepared to protect their sexual health. Some studies have shown that initiating sex at a younger age is positively associated with increased lifetime number of sexual partners and, consequently, increased chances of infection with HIV and STIs.12 With the exception of Ghana, more 12-14 year old males than females reported having had sex. Perhaps more indicative of the actual levels of sexual activity and the social context in which very young adolescents live, is the proportion who think their close friends have had sexual intercourse. At least one in 10 of very young adolescents say they have close friends who have had sexual intercourse (ranging between 11-42% of females and 17-53% of males). Very young adolescents in Malawi and Uganda—both girls and boys—report close friends being sexually-experienced at least twice the level that 12-14 year olds are reporting in Burkina Faso and Ghana. For example, 21% of 12-14 year old girls in Ghana say close friends have had sex compared to 42% of their peers in Uganda. While some evidence suggests that people often think their friends are engaging in stigmatized behaviors to a higher degree than they actually are, the reports of what close friends are doing could be considered a rough upper estimate of the behavior.13,14 In Burkina Faso and Malawi, considerably more males than females reported that their close friends were sexually active, while the reporting was about the same for boys and girls in Ghana and Uganda. Table 2 also shows the percentage of sexually-experienced 12-14 year olds who said they had ever been coerced into sex. While small sample sizes preclude analysis across all countries, the Uganda data show that 29% of sexually-experienced girls reported ever being sexually coerced compared to only 4% of sexually-experienced boys. In Malawi, 9% of boys reported having ever been sexually coerced (there were too few cases of sexually-experienced girls to show comparable information). While sexual experience among the majority of 12-14 year olds is not coerced, the data from Uganda show that girls this age who have initiated sexual activity have a much greater risk of experiencing sexual coercion compared to their male peers. Knowledge of Sexual and Reproductive Health Issues As noted by Kofi Annan, "Knowledge is power. Information is liberating. Education is the premise of progress, in every society, in every family."15 With respect to protecting sexual and reproduc-tive health, this is particularly relevant for the very young adolescents, many of whom are yet to become sexually active, so that they make informed and responsible decisions when they eventually initiate sexual activity. In order to effectively equip young adolescents with the information they need to protect themselves from the risk of unintended pregnancy and STIs, including HIV, it is important to have a good understanding of the level and depth of knowledge that they currently have about contraception and STIs. Awareness of contraceptive methods is generally high among young adolescents (Table 3). With the exception of Burkinabé males and females and Malawian females, at least 8 in 10 young female and male adolescents had heard of at least one contraceptive method. In Burkina Faso, Malawi, and Uganda more males reported awareness of contraceptives than their female counterparts. Awareness about HIV is even higher: Again, with the exception of Burkina Faso where 75% of girls and 80% of boys were aware of HIV, this proportion is at least 90% in the other three countries. In Burkina Faso, young adolescent males tend to show greater awareness about HIV than their female counterparts, while there is little or no gender difference in the other countries. Compared to contraception and HIV, awareness about STIs other than HIV among very young adolescents is relatively low _ lowest in Burkina Faso (less than 1 in 5), 1 in 4 in Ghana, almost 4 in 10 in Uganda and about 1 in 2 in Malawi. Only in Burkina Faso is there a significant difference between girls and boys in the proportions who report knowing about STIs other than HIV. While it is good news that awareness about contraception and HIV is high among young people, most of whom have yet to become sexually active, it must be acknowledged that awareness is a rough measure of knowledge because it provides no indication of depth of knowledge. It is possible for the level of awareness to be high while actual knowledge may be superficial.16,17 Evidence from this study shows that although awareness of HIV is very high among young adolescents in all four countries, in-depth knowledge about HIV transmission and prevention is very low (Table 3). This is particularly true in Burkina Faso where only 5% of young adolescent females and 9% of their male counterparts demonstrated in-depth knowledge about HIV; that is, they correctly answered five questions that constitute an indicator of HIV prevention knowledge recommended by the World Health Organization for monitoring HIV/AIDS prevention programs for young people. In the remaining three countries, the proportions of females and males with detailed knowledge range from 17% among males in Uganda to 24% among males in Malawi. In Burkina Faso and Malawi, boys have greater knowledge about how HIV can be transmitted and prevented than girls, and in Uganda it is girls who have somewhat better knowledge than boys (there is no significant gender difference in Ghana). The composite measure of knowledge of pregnancy prevention (that includes four questions) shows that young adolescents have an even lower level of detailed knowledge about pregnancy prevention, than they do about HIV. The proportion of adolescents who have adequate knowledge about pregnancy prevention is lowest among boys and girls in Burkina Faso (2-3%), followed by Ghana and Malawi (6-12% and 8-15%, respectively) and somewhat higher in Uganda (11-20%). Knowledge of pregnancy prevention is higher among girls than boys in three of the four countries (Ghana, Malawi and Uganda), and there is no significant gender difference in Burkina Faso. For a variety of reasons, the condom is a very important method for safeguarding young people's sexual and reproductive health. Among sexually active people, it is the only known method that provides simultaneous protection against HIV and unintended pregnancy,18,19 and for unmarried young people who often have sex sporadically, it is a very appropriate method because it is coital dependent, and because it is more accessible than methods that need a medical visit or a prescription. Because of the importance of condoms for this group, it is pertinent that young people have good knowledge about the method. In general, condom awareness among young adolescents is as high as awareness of any method of contraception discussed above. However, the levels of awareness are variable across countries and differ by sex in some of the countries. For example, in Burkina Faso, Malawi and Uganda, young male adolescents are more likely to report knowing about the condom than their female counterparts (73% vs. 64%, 77% vs. 61% and 91% vs. 81%, respectively). The difference is not statistically significant in Ghana. To gauge young adolescents' depth of knowledge about the condom, including how to use the method, we asked those who indicated they have heard of the male condom whether they had seen a demonstration on how to use condoms. There is a large gap between those who know of the male condom versus those who have actually seen how a condom demonstration. Young Malawian adolescents are the least likely to have seen demonstrations of condom use, although boys are more likely to have done so than girls (12% vs. 5%). This result should be a major concern for sexual and reproductive health programs in Malawi, given that the country's HIV prevalence rate is not only the highest of the four countries in this study, but one of the highest in Africa. In Burkina Faso, Ghana and Malawi, young male adolescents are more likely to report having seen condom demonstrations than their female counterparts. In Uganda, girls and boys are equally likely to have seen the method demonstrated (22-24%). Despite these variations, levels are low in all four countries, and only a minority of 12-14 year olds has seen a condom demonstration - less than a third of boys and less than one in five of girls. Sources of information on sexual and reproductive matters The sensitive issue of the need for information on HIV and pregnancy prevention among young adolescents in Sub-Saharan Africa has led to policy and political debates about what information to give adolescents and the age at which to start such interventions.20 Various stakeholders (particularly religions leaders) have argued that teaching adolescents about sex and reproductive health would encourage them to indulge in sexual activities. And yet, despite the sensitivity of the issue, there is increasing consensus and acknowledgement that it is important to institute effective sex education programs to equip young people with information as well as skills to help them make informed and responsible decisions on sexual and reproductive health matters. The low levels of in-depth knowledge of HIV/AIDS and pregnancy (discussed above) underscore the need to avoid "looking the other way" and to instead re-examine current educational strategies in the light of the information needs of young adolescents. In this section we examine the range of sources of information on sexual and reproductive health issues that young adolescents report using and explore the extent to which school-based family life or sex education programs are reaching this group in the four countries. Table 4 shows that young adolescents get information about HIV, STIs and contraceptives from a wide range of sources and that they often do so from more than one source. Mass media is the most commonly used source of informa-tion for these three topics combined for young male adolescents in all four countries and for females as well in Burkina Faso and Ghana. Among Malawian and Ugandan young adolescent females, however, schools and teachers were a slightly more common source of information than mass media. In all four countries, young male adolescents are more likely to report having received information from mass media than young females. While close to 6 in 10 young adolescents accessed information on sexual and reproductive health from schools in Ghana, Malawi, and Uganda, less than 25% did so in Burkina Faso (a result of the low levels of school attendance). Friends are a key source of sexual and reproductive health information for young adolescents, especially in Malawi and Uganda where at least half of both male and female young adolescents mentioned this source. Health facilities and professionals are not a major source of information for young adolescents; with the exception of Malawi where 50% of girls and 36% of boys reported having gotten information from this source. Parents are a significant source of information among young Ugandan girls (51%) as well as boys (27%) and much less so in the other three countries. Other relatives play a bigger role than parents in all three countries (not Ghana) though not near the level of the mass media in all four countries or, in Ghana, Malawi and Uganda, teachers and schools. The results for the level of exposure to sex education in school show that the majority of 12-14 year olds did not receive family life or sex education. Less than 20% of all young adolescents in Burkina Faso and Malawi received sex education in schools while a larger proportion did so in Ghana (41% of girls and 28% of boys) and Uganda (34% of girls and 22% of boys). There is no consistent pattern in gender differences across the four countries; more girls than boys reported that they were exposed to sex education in schools in Ghana and Uganda, while the opposite pattern (though not significant) prevailed in Burkina Faso and Malawi. For family life and sex education programs to be effective, it is important that information is conveyed to young people before they become sexually active and begin to be exposed to sexual and reproductive health risks. In order to assess the extent to which school-based sex education programs are reaching adolescents before they start having sex, we examined data about the age when sexually experienced adolescents said they first received sex education in school and the age they were when they first had sex. The results show that in all four countries, among young people who receive sex education, almost all did so before first sex. For instance, among the few adolescents who have received family life or sex education in school in Burkina Faso (14% of males and 10% of females) almost all received it before first sex (Table 4). In Malawi, the observed gender difference in the proportion that received sex education in school disappears when it comes to whether sex education was received before first sex. Young adolescents who received sex education in schools were also asked whether they had received information on each of four specific topics (how pregnancy happens; contraception/how to prevent pregnancy; abstinence/say "no" to sex; and sexually transmitted infections or diseases). These results show that there is a good balance in coverage of issues relating to pregnancy and sexually transmitted infections, and that most adolescents who received sex education did so for all four topics. Although the absolute differences are not large, more boys than girls report having received sex education on all topics in Malawi and on one topic (sexually transmitted infections or diseases) in Burkina Faso. In contrast, in Ghana and Uganda, more girls than boys reported receiving information on all topics. Discussion The period of adolescence generates considerable anxiety among adults as well as among adolescents themselves because of the challenges and risks that young people face as they experience sexual maturation and start interacting with the opposite sex. It is a period when, for the first time in their lives, young people have to make decisions on whether to be in a romantic relationship, what sort of person to be in a relationship with, whether to start having sex, and (if they are sexually active) whether and how to protect themselves against pregnancy, HIV and STIs. Adults providing care to adolescents in various capacities ranging from parents, guardians, teachers, health providers, religious leaders, relatives, and program managers also grapple with similar challenges as they consider how to best assist adolescents make voluntary, informed and responsible decisions. Adults have to consider the most appropriate age to provide adolescents with information about sexual health, the most effective means of doing so, and how to deal with the challenges associated with adolescents' initiation of sexual behavior. The emerging evidence demonstrating the unique vulnerability of young people, especially females, to HIV infection and unplanned pregnancies has highlighted the need to develop effective intervention programs to protect the next generation of productive and reproductive adults in Sub-Saharan Africa. Schools are generally considered to be one of the most important avenues for providing sex education to young people because most of them attend school at one time or another.2 School-based sex education programs have evolved and increasingly gone beyond just the provision of information. Some programs now aim to build life skills, including negotiation and communication with partners, self-efficacy, and to empower young people to resist peer pressure and to understand their right to information and services to protect their sexual health.20,21,22 One of the major obstacles that such programs face is inadequate understanding about what adolescents already know, how accurate, practical and adequate is their knowledge, where they get the information from and what are the best ways of reaching adolescents, some of whom are not in school. This study contributes to filling some of these knowledge gaps by providing nationally-representative evidence from four countries on the sexual behaviors and related information needs of very young adolescents aged 12-14, a group about which very little is known. The urgency for equipping young adolescents with adequate and correct knowledge on how to protect themselves from STIs and pregnancy is warranted by the finding that 12-14 year olds are not as naïve on sexual matters as one may think. For instance, at least 3 in 10 of 12-14 year old girls in Uganda and boys in both Uganda and Malawi say they have experienced some form of intimate sexual activity (sexual intercourse, kissing, fondling, or they have had a boyfriend or girlfriend). The concern is also applicable to Ghana and Burkina Faso, where, even if the proportion of young people who report that they have experienced some type of intimate sexual activity is much lower, many will soon begin to do so. In all four countries, a much higher proportion of very young adolescents say they have close friends who have had intercourse than the proportion who say they themselves have initiated sex. It is likely that the true level lies somewhere between these two indicators: if so, based on the midpoint between the two values, and reflecting the range across the four countries, approximately 5-10% of 12-14 year old girls and 10-30% of boys this age may have already initiated sexual intercourse. The relatively high percentages of 12-14 year old boys in Malawi (19%) and Uganda (15%) and Burkina Faso (6%) who reported that they had ever had sexual intercourse suggests that boys in these countries may be facing heightened vulnerabilities that may propel the spread of sexual and reproductive health risks to the general population as they grow up. While some studies have shown that boys tend to over-report sexual activity and girls tend to under-report,23,11 the large size of the reported gender differences (and the fact that we do not observe the same pattern in Ghana) suggests that higher proportions of boys 12-14 than girls this age have likely initiated sex, particularly in Uganda and Malawi. This should be a major concern and call for further investigation to identify drivers of this behavior and ways to address it. Our results also demonstrate areas where young adolescent girls appear to be more disadvantaged than their male counterparts. For instance, the Uganda data that allow us to compare the extent of sexual coercion between boys and girls show that girls are far more disadvantaged in this area. The analysis of young adolescents' sources of information on sexual matters shows that even if some sources are more dominant in some countries than others, young adolescents use many information sources in all four countries. Mass media is by far the most dominant source of information for young adolescents (both girls and boys) in Ghana and Burkina Faso, but the second most important source is teachers and schools in Ghana and other family members in Burkina Faso. In Malawi and Uganda, the mass media, schools and friends are the leading sources of information, but while health services are the fourth most important source in Malawi, other family members are fourth in Uganda. The results also show that despite increasing recognition of the importance of reaching adolescents through sex education programs in schools, relatively few young adolescents have accessed such programs.[FNB] This represents a critical missed opportunity since the majority of adolescents attend school at one time or another. Another important consideration is the age at which sex education is introduced: at a minimum, basic information should be provided before adolescents become sexually experienced in order to ensure that they are able to protect themselves from sexual and reproductive risks at this formative stage in their lives. In this regard, the results are positive — almost all adolescents who reported receiving sex education are getting it before they become sexually experienced. However, more detailed information is needed on the timing of teaching different topics and skills to young adolescents, to assess if young adolescents are receiving sufficiently comprehen-sive information, appropriately targeted to their age. Our results show impressively high levels of awareness of HIV/AIDS, condoms, and contraceptive methods among very young adolescents, similar to levels of knowledge among older adolescents (as well as adults) shown in other studies. However, we also find that the vast majority of adolescents lack the in-depth knowledge they need to effectively protect themselves against HIV and unplanned pregnancy. While at least 3 in 4 adolescents have heard about HIV/AIDS and at least 2 in 3 have heard about contraception, at most 1 in 4 had in-depth knowledge about HIV prevention and at most 1 in 5 had detailed knowledge about pregnancy prevention. A major challenge for programs is how to increase detailed knowledge about these issues among this young age group. These findings suggest that in order to improve the quality of information that adolescents receive on sexual health issues in schools, it is necessary to make sex education curricula, comprehensive, advocate use of more effective teaching approaches and improve training of teachers. A key reason that many young adolescents have not received sex education is that it is not offered in their schools. Of 12-14 year-olds who ever attended school, about half in Ghana and Uganda, and two thirds in Burkina Faso and Malawi report that no sex education classes were offered in their schools4-7(Table 9.2) The implication is that policymakers need to address the constraints within school systems that account for the absence of this subject in the school curricula. An added need is to document the extent to which sex education is offered in both the primary and secondary school levels; in government schools, as well as schools in the private sector (which is rapidly expanding in urban areas around the continent) and reasons why it is not offered in a high proportion of schools. A further implication of the findings is that there is a great need for development of programs and approaches to reach out of school adolescents, given the high rates of school dropout in many countries in Africa, and given the situation in countries like Burkina Faso where the proportion who have ever been to school is still low. Programs that provide sexual health information to young adolescents who are not attending school may be channeled through multiple sources—such as the media, public campaigns, sports and other types of activities in which young people engage, religious institutions and health providers. The wide range of sources of information that adolescents report using demonstrates that the multi-pronged approach is working quite well in reaching adolescents. What is further needed is attention to streng- thening and improving these sources, particularly in regard to the content of the information, its accuracy and comprehensiveness. Such efforts would help to ensure that adolescents in all circumstances and contexts obtain the sexual health information they need. Acknowledgements We are grateful for contributions to the overall study from colleagues at the Guttmacher Institute (United States), University of Cape Coast (Ghana), Institut Supérieur des Sciences de la Population (Burkina Faso), African Population and Health Research Center (Kenya), Centre for Social Research (Malawi) and the Makerere Institute of Social Research (Uganda). Authorship is alphabetical. This study was supported by The Bill & Melinda Gates Foundation, The Rockefeller Foundation and the National Institute of Child Health and Human Development (Grant # 5 R24 HD043610). Footnotes FN A School-based programs are also promising for administering the recently developed cervical cancer vaccine, which has to be administered to girls before they become sexually-active. FN B Even if at least 6 in 10 adolescents in Ghana, Malawi and Uganda indicated that they accessed sexual and reproductive health information from teachers and schools, considerably fewer adolescents indicated that they actually attended the formal sex education programs in schools, suggesting that some of this information could have been obtained through biology classes on physical anatomy and other related classes. References
© Copyright 2007 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh07033t1.jpg] [rh07033t2.jpg] [rh07033t3.jpg] [rh07033t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}