 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
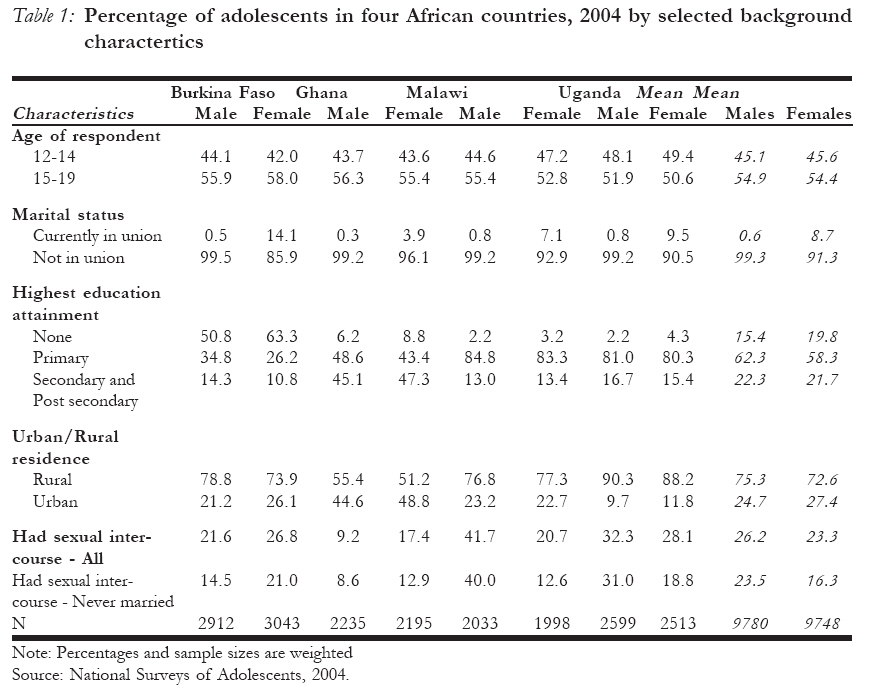
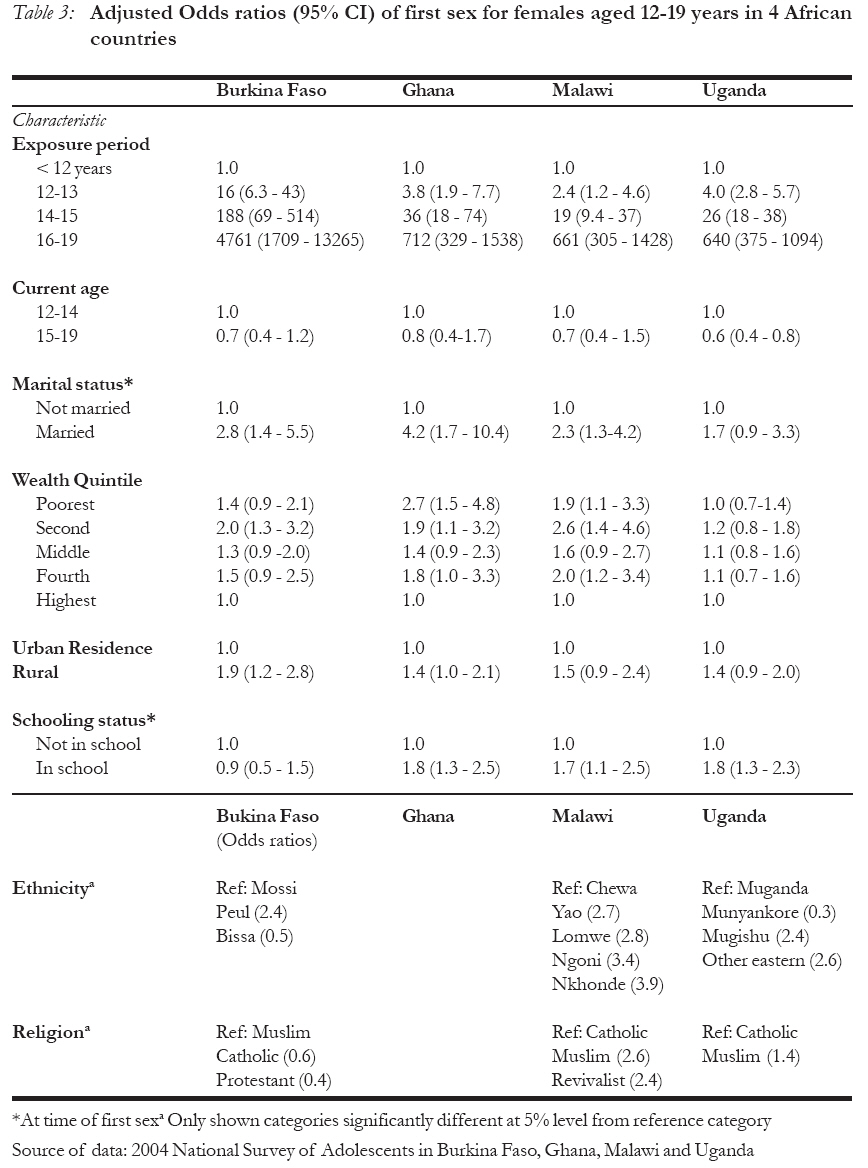
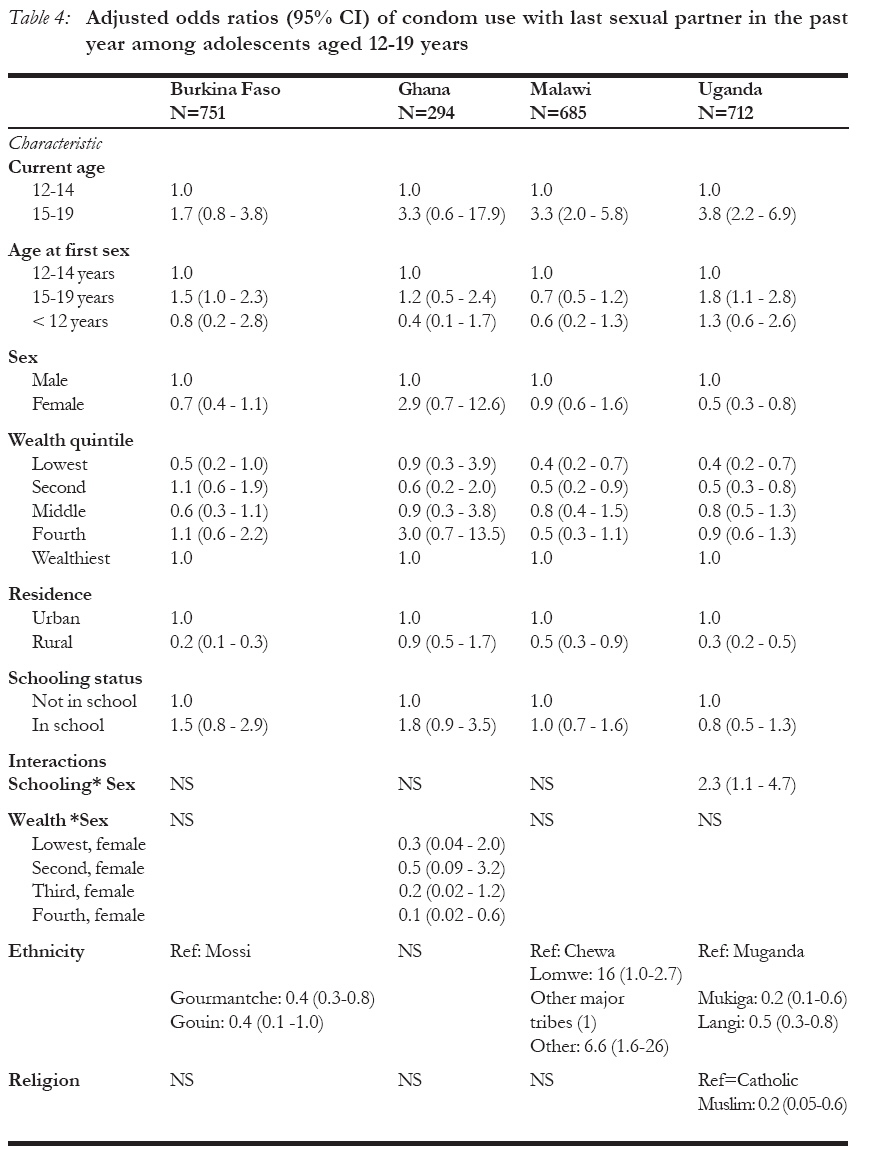
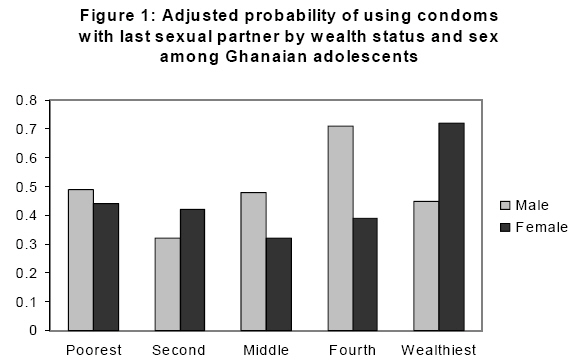
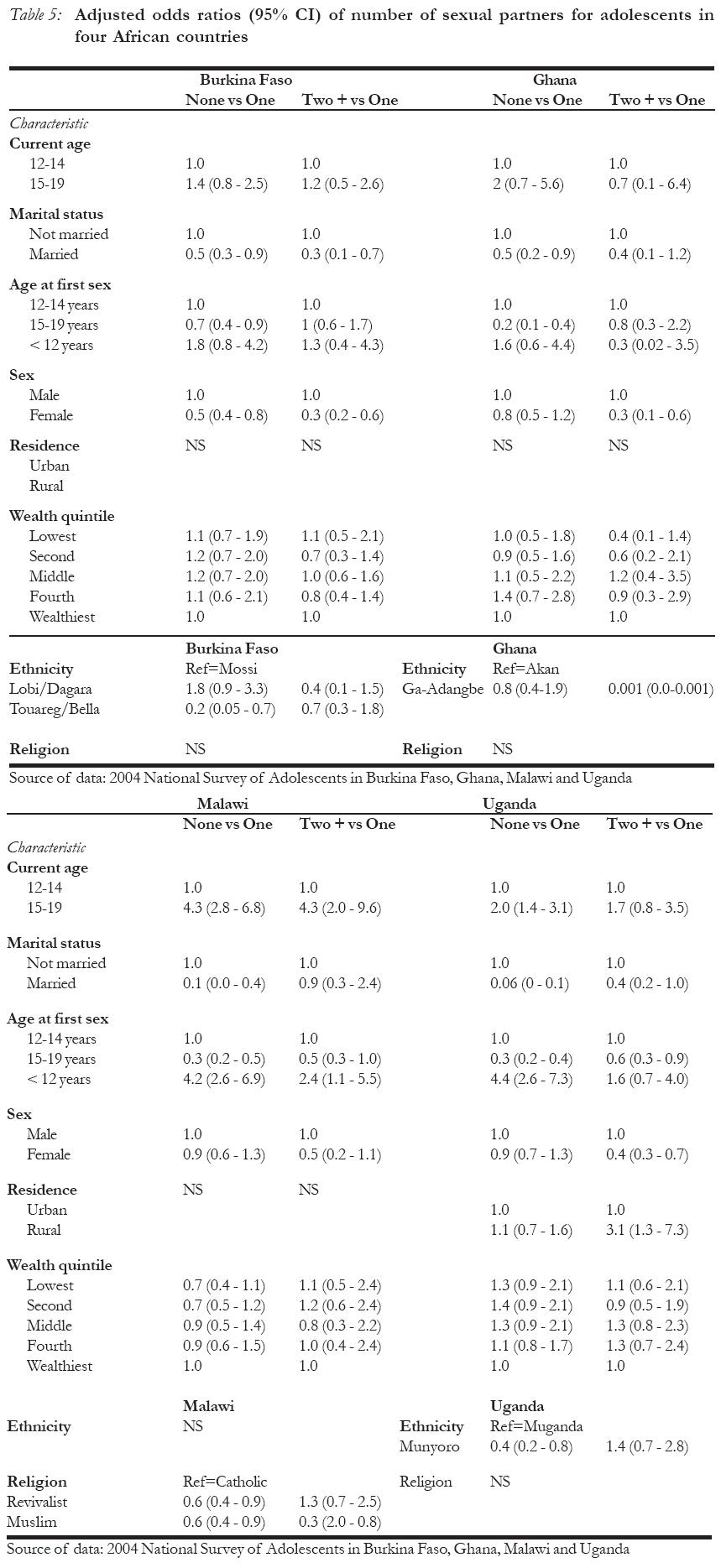
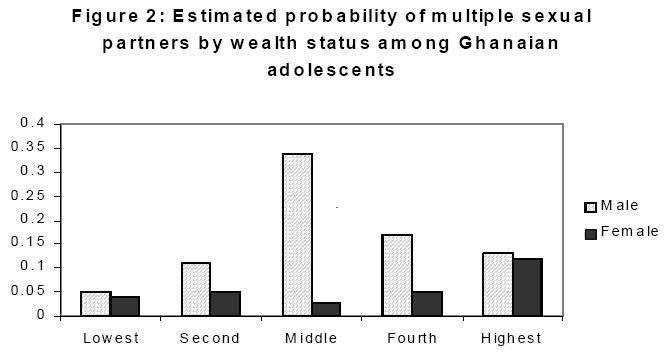
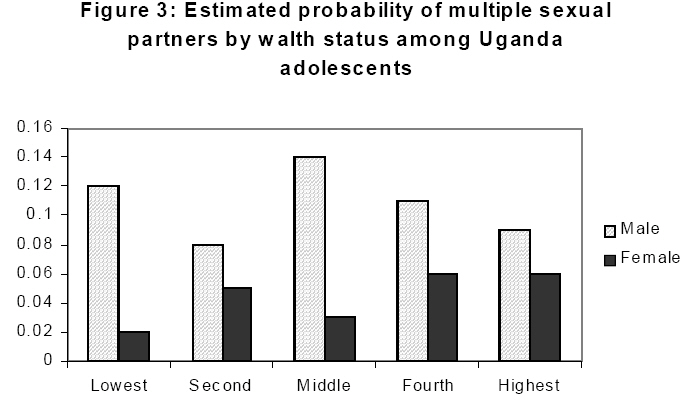
African Journal of Reproductive Health, Vol. 11, No. 3, December, 2007, pp. 83-98 Is Poverty a Driver for Risky Sexual Behaviour? Evidence from National Surveys of Adolescents in four African Countries Nyovani Madise1, Eliya Zulu2 and James Ciera3 Institutional Affiliation: Code Number: rh07036 Abstract This paper contributes to conflicting evidence on the link between poverty and risky sexual behaviour by examining the effect of wealth status on age at first sex, condom use, and multiple partners using nationally representative adolescents' data from Burkina Faso, Ghana, Malawi, and Uganda. The results show that the wealthiest girls in Burkina Faso, Ghana, and Malawi had later sexual debut compared with their poorer counterparts but this association was not significant for Uganda. Wealth status was weaker among males and significant only in Malawi, where those in the middle quintile had earlier sexual debut. Wealthier adolescents were most likely to use condoms at the last sexual act, but wealth status was not associated with number of sexual partners. Although the link between wealth status and sexual behaviour is not consistent, there is evidence that poor females are vulnerable to infection because of earlier sexual debut and non-use of condoms. Résumé Est-ce que la pauvreté est un moteur des comportements sexuels risqués? Evidence tirée de l'enquête nationale sur les adolescents dans quatre pays africains. Cet article contribue à l'évidence contradictoire sur le lien entre la pauvreté et le comportement sexuel risqué tout en examinant l'effet que la situation de richesse a sur l'âge au moment du premier acte sexuel, l'emploi du préservatif et les partenaires multiples; ceci à l'aide des données à représentation nationale auprès des adolescents au Burkina-Faso, au Ghana, au Malawi et en Ouganda. Les résultats ont montré que les filles les plus riches au Burkina-Faso, au Ghana et au Malawi ont eu leur premier acte sexuel plus tard par rapport à leur homologues moins riches, mais ce rapport n'était pas significatif pour l'Ougnada. La situation de richesse était plus faible chez les mâles et elle était significative seulement au Malawi où ceux de richesse moyenne ont eu un premier acte sexuel plus tôt. Les adolescents les plus riches avaient plus la possibilité d'utiliser le préservatif au cours du dernier acte sexuel, mais la situation de richesse n'était pas liée au nombre de partenaires sexuels. Bien que le lien entre la situation de richesse et le comportement sexuel ne soit pas coherent, il y a l'évidence que les femelles pauvres sont vulnérables à l'infection à cause d'un début sexuel antérieur et le non emploi des préservatifs. Key Words: Adolescents, Sub-Saharan Africa; Sexual and Reproductive Health; Poverty Introduction Before the advent of HIV and AIDS, adolescents were considered to have the lowest burden of disease compared to other age groups. However, HIV prevalence among young people has increased steadily especially in the poorer nations and prevention strategies aimed at this group must be anchored on evidence of the proximate and background risk factors that increase the vulnerability of young people. Adolescents' sexual behaviour is of public health importance since young people often lack adequate knowledge and skills of how to protect themselves from unplanned pregnancies and sexually transmitted infections. Furthermore, patterns of sexual behaviour formed during adolescence may influence behaviour in adult life and consequently affect long-term progress in the fight against HIV and AIDS. For example, data from population-based HIV surveys in Kenya, Ghana, Malawi, and Uganda, under the auspices of the Demographic and Health Survey programme (DHS) show the highest HIV prevalence among women who had first sexual intercourse at very young ages (below 16 years). There is also evidence of strong links between the age at first sexual intercourse and extra-marital sexual relationship1 Studies on the link between poverty and risky sexual behaviour have become particularly important in the wake of growing evidence, which has challenged the assumptions of links between poverty and HIV and AIDS.2,3 When examined from a global perspective, no one can argue with the fact that the HIV epidemic has had the most impact on the poorest regions of the world. However, at national level the picture becomes puzzling because some of the wealthiest countries in sub-Saharan Africa (such as South Africa and Botswana) have some of the highest HIV prevalence rates in the world.2 At individual level, HIV prevalence rates derived from DHS samples and other population-based HIV surveys in a number of African countries are showing positive relationship between wealth and HIV prevalence.3,4 This association appears more pronounced among females than males. There are many good explanations why wealth status and HIV should be linked. At macro level, poor nations often lack the resources to provide preventive and curative services, thus increasing their populations' susceptibility to HIV infection. At individual level, poverty is associated with illiteracy, gender inequality, and failure to negotiate for safer sex.5,6,7 On the other hand, the spread of HIV in Africa is linked historically to mobility particularly among wealthier people.8 People with mobile lifestyles interact sexually with other groups who may have higher (or lower) HIV prevalence, thus furthering the spread.. In addition, wealthier men may be at higher risk of infection because of multiple and concurrent sexual partnerships, which they are able to maintain because of their wealth.2,8 Another reason why wealthier people may have higher HIV prevalence is because they may live longer due to better nutrition and access to antiretroviral therapies.9 While the positive relationship between HIV prevalence and socioeconomic status appears to be common in most African countries where community-based HIV testing has been done, the evidence for the relationship between poverty and sexual risk-taking appears mixed. Booysen, who used South African DHS data to examine the link between poverty and risky sexual behaviour did not find a significant association between wealth status (measured by quintiles) and women's risky sexual behaviour.10 His definition of sexual behaviour included having sexual intercourse with a casual acquaintance and not using condoms, and having multiple sexual partners. On the other hand, Hallman who used different data from South Africa found a strong association of poverty and risky sexual behaviour among young men and women.11 A strong association of poverty and risky sexual behaviour has also been reported in other settings. Zulu et al. found that women living in Nairobi slums in Kenya had significantly higher levels of sexual risk-taking than other women.12 Another study using Kenya DHS data found similar results, but socioeconomic status (defined as `low'; `medium'; and `high' based on ownership of household assets) was not significantly associated with risky sexual behaviour among men.13 The lack of consistency in findings from different studies can be attributed in part to the different ways in which these concepts are defined. Clearly, if the link between HIV infection and poverty is to be understood research is needed to systematically examine the link between poverty and determinants of HIV infection, including sexual behaviour. In particular, cross-national comparisons using similar definitions of poverty and risky sexual behaviour can provide powerful evidence of the association. In this paper, we focus on relative poverty, which is measured by wealth quintiles within communities. Other forms of poverty such as absolute poverty, and lack of reproductive choices are also important for understanding HIV and AIDS but these are not the focus of this paper. We examine the link between wealth status and sexual behaviour of young people aged 12-19 years, using unique nationally-representative data from four African countries. These surveys used census enumeration areas or Demographic and Health Survey (DHS) sampling frames to draw nationally representative samples of households as we describe below. Most nationally representative studies that have examined the link between poverty and sexual behaviour have concentrated on females only. Furthermore, most studies use DHS data, which do not include adolescents aged less than 15 years and which have small samples of adolescents to enable multivariate analyses. Adolescents are an important group to study because they may become sexually active at times when they are not ready to take full responsibility of the consequences of such behaviour. Initiation of sex may stem from desires to experiment, unwarranted trust of the sexual partner, expectation of gifts or money and young people's tendency to minimise the risks of unplanned pregnancies or HIV infection.14,15,16 If poverty is an important driving factor for unsafe sexual practices, we should expect higher proportions of adolescents from poorer families to exhibit such behaviours. In particular, because the flow of exchange of money and gifts in Africa is predominantly from males to females, poorer females and wealthier males would exhibit higher risky sexual behaviours. If, on the other hand, curiosity and experimentation are the most important drivers for initiating sexual activity, we would expect a weaker or no association between wealth status and sexual behaviour. Furthermore, if access and cost are important factors in the use of condoms among young people in Africa, we should see a strong positive relationship between wealth status and use of condoms. Data and Methods Under the auspices of a five-year study titled "Understanding HIV Risks among Youth: Protecting the Next Generation", nationally representative surveys of adolescents were conducted in 2004 in four African countries namely Burkina Faso, Ghana, Malawi, and Uganda.18 The four countries were chosen to represent different levels and contexts of HIV prevalence. According to the 2006 UNAIDS global report on AIDS epidemic, the adult HIV prevalence rates in the four countries in 2003, which are almost the same as the rates for 2005, were: Burkina Faso 2.1 percent, Ghana, 2.1 percent, Malawi, 14 percent, and Uganda 6.8 percent.17 Approximately 19,500 male and female adolescents aged 12-19 years were interviewed in the four countries to gather information on their sexual experiences together with a range of information on their socioeconomic status, schooling, childbearing, contraception, HIV knowledge, and other information. Macro International, who has vast experience of implementing comparable nationally represen-tative demographic and health surveys around the developing world, conducted the surveys together with local institutions in the four countries. In all four countries, multi-stage cluster sampling was used to select enumeration areas from strata (defined by region and rural/urban residence), then households were selected, and finally adolescents aged 12-19 years were picked from the selected households. Similar questionnaires were used in all four countries, thus enabling the same definitions of risky sexual behaviour and wealth status to be used. Much of the demographic data have already been published with greater detail than given here.18 We define risky sexual behaviour using three characteristics: age at first sexual intercourse (where sexual debut before the age of 16 years is regarded as `risky'); non-use of condoms at last sexual act for those who had sexual activity in the 12 months before the survey; and the number of multiple sexual partners within the previous 12-month period. Wealth status was determined using wealth quintiles derived from information on the presence or absence of household assets and amenities as proposed by Filmer and Pritchett (1998)19. These amenities and assets included source of drinking water, type of toilet facility, source of cooking fuel, type of building material, electricity, ownership of a car, TV, refrigerator, radio, lamp, oxcart, plough and other assets. Preliminary examination of the data showed that the wealth index was favourably biased towards urban households, hence analyses to generate wealth quintiles were done separately for rural and urban households. Thus, the variable measures the relative wealth status of individuals to others in their community (urban or rural) and all the analyses control for urban or rural residence. Other variables that were included in the analyses are: current age of the respondent, whether or not in school, orphan status, religion, ethnicity, and region of residence. For the analysis of age at first sexual intercourse we used schooling status at the time of first sex. For the age at first sexual intercourse, discrete-time hazard models using logistic regression were used to estimate the likelihood that an adolescent who has not yet had sexual intercourse will have it at the following ages: less than 12 years; 12-13; 14-15; and 16 years or older. For these analyses, separate statistical models for males and females were conducted in each of the four countries after preliminary analyses showed the presence of several significant interactions involving the sex variable. Since the surveys were complex, we specified the survey designs in STATA (i.e. defined the strata, clusters, and unequal sampling weights) and we used the SVY logistic commands.20 For condom use, logistic regression analysis was restricted to unmarried adolescents who had sexual intercourse in the 12 months before the survey. Whether or not condoms were used during the last sexual act was the dependent variable. Four models, one for each country, were fitted, pooling together the female and male data. For multiple sexual partnerships, we considered only adolescents who were sexually active and examined the number of partners in the 12 months before the survey, i.e. `none', `one' and `two or more ' sexual partners. Married adolescents were included in the multinomial logistic models and a dummy variable for marital status was included. Results Table 1 presents some background characteristics of the adolescents who participated in the national surveys. Slightly over half of the adolescents were aged 15-19 years and very few were married; the highest percentage of females who were married was in Burkina Faso (14%) while the lowest was in Ghana (4%). Roughly, about a quarter of unmarried adolescent males were sexually experienced compared with about 16% of females. In Ghana and Burkina Faso, more females than males were sexually experienced while in Malawi and Uganda more males than females were sexually experienced. Age at First Sexual Intercourse Table 2 and 3 present the odds ratios of having sexual intercourse, separately for males and females. As expected, the likelihood of adolescents becoming sexually experienced increases rapidly with age with the majority of adolescents becoming sexually active by the time they reach 19 years of age. For example, the odds of having first sex between the ages of 12 and 13 are about 7 among Burkina males, rising to 502 for those aged between 16 and 19 years. The corresponding odds ratios for Burkinabe females are 16 for 12-13 year-olds and 4,761 for those aged 16-19 years. The large odds ratio for the oldest adolescent females reflects the certainty that those who are yet to experience first sex will do so within this age-range. Examining age at first sexual debut by current age, we found that younger adolescents aged 15-19 years were less likely to report that they were sexually experienced, when they were aged 12-14 years, compared with the younger cohort (currently aged 12-14 years). This association was stronger among males and was significant in three countries (OR=0.5 for those aged 15-19 in Burkina Faso; OR=0.6 for Malawi and Uganda). Although the same pattern was observed among females, the association was significant in Uganda only. Among the females, marriage was strongly associated with sexual experience, as one would expect. The lack of significance of this variable for Uganda was surprising. Wealth status was significantly associated with the age at first sex at a five percent level in Burkina Faso (females), Ghana (females), and Malawi. In Burkina Faso, Ghana, and Malawi, adolescent females in the wealthiest quintiles were least likely to initiate first sex at each age interval. In Burkina Faso and Malawi, female adolescents in the second poorest quintile were most likely to have had sex (OR=2 and 2.6, respectively), and in Ghana the highest odds of having first sex were among the poorest female adolescents (OR=2.7). Wealth status was not significantly associated with the age at first sexual intercourse among Ugandan females. However, Ugandan female adolescents were more likely to report being sexually active than females in other countries. Overall, Malawian males had the highest pro-bability of initiating first sex when compared with the other countries. When wealth status was examined, it appears that Malawian male adolescents in the fourth, wealthiest, and lowest quintiles were less likely to be sexually experienced compared with other adolescents. Those in the middle quintile had the highest probability of having first sex. Wealth differences among male adolescents in the other three countries were negligible. The surveys collected information on schooling status and the ages when adolescents who had left school had dropped out. Thus, we were able to examine the schooling status at the time of first sexual debut among those sexually experienced. Surprisingly, all the results except for Burkina Faso females (OR=0.9), show that those in school were more likely to report having had first sex compared to those who had dropped out or those who never attended (OR between 1.7 and 3.3). Ethnicity is an important determinant of the age at first sexual intercourse except in Ghana where only region of residence was significant. Muslim girls in Burkina Faso, Malawi, and Uganda have higher probability of initiating first sex compared with Catholic girls in general. Condom Use at last Sexual Intercourse Overall, about 43 percent of males and females who were sexually active in the 12 months before the survey stated that they had used condoms with the last sexual partner. Older adolescents were more likely to report that they used condoms with the last sexual partner but this association was significant only in Malawi and Uganda (OR=3.3 and 3.8, respectively). Condom use was not strongly associated with the age when an adolescent started having sexual intercourse. Wealth status was significantly associated with condom use at 5 percent level in Ghana, Malawi, and Uganda. In Malawi and Uganda, the poorest adolescents had the lowest odds of using condoms (OR=0.4) compared with the wealthiest. In Ghana, there was a significant interaction with the sex variable (see Table 4). From the interaction, we were able to compute adjusted probabilities, which showed that approximately 72 percent of the wealthiest females used a condom, compared with 44 percent of the poorest and 32 percent of the middle quintile. Among the males, the highest condom use at last sexual act was among those in the fourth quintile (71 percent) and lowest among those in the second quintile (32 percent) (see Figure 1). Generally, condom use was lower in rural than in urban areas (OR=0.2 in Burkina Faso, 0.5 in Malawi, and 0.3 in Uganda). In Ghana, this variable was not significant. The interaction between schooling status and sex in Uganda indicates that being in school is significantly associated with higher condom use among females (47 percent compared with 41 percent of those not in school). Among males however, about 55 percent who were not in school reported to have used a condom compared with 41 percent of those in school. Multiple Sexual Partnerships Multinomial logistic regression models were fitted for each country data where the dependent variable was the number of sexual partners in the 12 months before the survey (`none', `one', `two or more'). These analyses were restricted to adolescents who were sexually experienced and thus we interpret those who reported to have had no sexual partner is that of secondary abstinence. For married adolescents who reported one partner, this was the spouse. Overall, about 20 and 34 percent of sexually experienced female and male adolescents, respectively, did not have a sexual partner in the 12 months before the survey. However, 12 percent of boys as opposed to about 5 percent of girls report that they had two or more sexual partners during the year before the survey. The variable measuring wealth status was not statistically significant in any of the four models (see Table 5). Generally, a higher proportion of older adolescents (aged 15-19 years) reported to have had no sexual partner in the 12 months before the survey but the estimates were not statistically significant except in Malawi (OR = 4.3, p-value < 0.05) and Uganda (OR = 2.0, p-value < 0.05). In Malawi, a higher proportion of older adolescents who were sexually active in the 12 months before the survey also reported to have had two or more partners as opposed to just one partner (OR = 4.3). This association was not statistically significant in the other countries. The age at first sex was not significantly associated with the number of sexually partners in Burkina Faso and Ghana. In Malawi the odds of having two or more sexual partners for those who first had sex before the age of 12 were 2.4 times higher than those who had first sex between the ages of 12 and 14. As expected, married adolescents were less likely to be abstinent (OR=0.06 in Uganda; 0.0 in Malawi; 0.5 in Burkina Faso and Ghana). Although the odds of two or more sexual partners (as opposed to just one) were lower for married adolescents, this association was not statistically significant in any of the four countries. Religion was significant in Malawi, showing lower likelihood of reporting abstinence in the 12 months before the survey among sexually experienced revivalists (i.e. charismatics or evangelists) and Muslims (OR=0.6), and significantly lower likelihood of multiple partners among Muslim youths. In the other three countries, there were ethnic differences in the number of sexual partners. Additionally in Uganda, the odds of reporting multiple sexual partners (as opposed to one partner) for rural adolescents were three times those of urban adolescents. Since "sticking to one partner" is considered protective behaviour, we carried out binary logistic regression to assess the effect of wealth status on whether the adolescents had multiple sexual partners (2 or more) or not (0 or 1). The results of this analysis show that wealth status (when interacted with gender) has a significant association with multiple sexual partnerships in Ghana and Uganda, but not in the other two countries. The results for Ghana and Uganda (Figure 2 and 3), show that the effect is more pronounced for boys where those in the middle wealth status group exhibit the highest risk of having multiple sexual partners compared to the other wealth categories. Discussion HIV prevalence in sub-Saharan Africa is very high and is transmitted mainly through heterosexual acts. Hence, the risks of infection as adolescents become sexually active are quite high. The focus on young people's sexual behaviour is warranted because sexual practices and norms developed during this period affect behaviour and health in adult life.1,21 Several researchers have suggested that poverty may be a motivation for young people to engage in early sexual activity and to have multiple partners, and this assertion has stemmed mainly from adolescents' reports of exchange of gifts and money in sexual partnerships.16,22,23,24,25 Our findings find some support of an association between wealth status and age at first sexual intercourse among female adolescents. The observed higher likelihood of initiating first sex among poorer females is consistent with the assumption of disadvantaged women having earlier sexual debut in order to have access to cash and gifts.8,11,26 Poverty can also contribute to early sexual debut through early exposure and socialization into sexual activity. This has been observed of children living in slum areas where accommodation is very cramped and where it is very common for children to sleep in the same room as their parents. 12,27 The association between wealth status and initiation of first sexual intercourse among Malawian males is inconsistent with the wealthiest (or the poorest) exhibiting the highest risky sexual behaviour since it is those in the middle and second quintiles who initiated sex earlier. A plausible explanation for a weaker association between wealth status and the age at first sexual intercourse among males is that the main motivation for first sex may be curiosity or experimentation. This assertion is supported by information collected from the adolescents who participated in these surveys on why they had first sexual intercourse. Roughly about 63% of girls and 80% of boys said they had first sex because they felt like it or wanted to experiment. About 9% of girls mentioned expectation of gifts or money as the reason for having sex and another 19% of girls reported that their first sexual intercourse was forced or that their partner had insisted. Although the use of condoms among young people in sub-Saharan Africa is still very low, there are indications that their use is increasing especially among those not married.28 From the adolescent surveys that we used, condom use with the last sexual partner was about 43 percent. Generally, the poorest adolescents were less likely to have used condoms with their last sexual partner compared with the wealthiest. In spite of efforts by national HIV prevention programmes to reduce or eliminate the cost of condoms in many African countries, adolescents still report affordability as a reason for non-use and our findings appear to support this. For females, the ability to negotiate for use of condoms may be harder if they have received gifts or money.14 Generally, lower use of condoms was observed among rural adolescents, which may indicate poorer access to condoms in rural areas compared with urban areas. Other reasons have been cited for non-use of condoms among adolescents in other studies. These include dislike of condoms, and embarrassment to purchase or ask for condoms from adult providers, which stems from disapproving attitudes from health providers.29 The proportion of adolescents who reported multiple sexual partners in the four countries was low, which can be explained by the short exposure period between initiation of first sex and the survey date. From our study, there was a weak, but significant association between wealth status and having multiple sexual partners (as opposed to one or none) in two of the countries. Boys in the middle wealth quintiles were significantly more likely to have multiple sexual partners than those in the other wealth groups and it was not clear why this particular sub-group showed this tendency.. Other researchers have also reported weak or no association between socioeconomic status and multiple sexual partnership among young people.8 However, higher rates of multiple sexual partnerships have been reported among poorer women aged 15-49 years in Kenya12,13,27 as well as among younger women aged 15-24.12 The context of two of the Kenyan studies was among very poor slum women, who sometimes give sexual favours for subsistence. Our other findings show that higher proportions of younger adolescents reported to be sexually experienced at ages 12-14 years compared with the cohort now aged 15-19 years. This is contrary to findings by Wellings et al.30, who did not find that the age at first sexual intercourse was declining in Africa. A plausible interpretation for our finding may be that of reporting, where older adolescents could be reporting older ages at sexual debut than was the case. Younger males may have exaggerated their sexual experience also. Across the four countries, there were strong ethnic and religion differentials in the age at first intercourse, suggesting that cultural factors may influence sexual behaviour much more than economic factors. Muslim girls in three of the four countries were more likely to start sexual activity earlier than other girls, reflecting the phenomenon of early marriage among this group. Additional analyses (not shown), which excluded married adolescents showed that the significance of religion as a variable was weakened and remained only in Burkina Faso. Adolescents who were in school were more likely to start sexual activity earlier than those not in school. This finding is opposite to what other studies have reported.31,32 Others have reported that schooling did not appear to make a difference as to whether rural boys engaged in sex or not, but that girls in schools that were supportive were more likely to delay sexual initiation.32 With universal free primary education, school participation has increased, but age at first sexual debut appears not to have changed much. Thus, it is expected that initial sexual experience will take place in the school environment. School is also a place where greater interaction and socialization may take place, away from the prying eyes of parents. Thus those in school may have greater freedom. In this study, we extracted information on whether or not the adolescent was in school at the time of first sex indirectly i.e. from the information that adolescents gave on when they started and stopped school. Studies that ask direct questions about schooling at the time of first sex may get biased information especially if adolescents try to rationalize their behaviour after the event (e.g. reporting to have been out of school at the time they became pregnant). Conclusion Adolescents' sexual behaviour is of major public health interest because adolescents often are not equipped to cope with the consequences of early and unprotected sexual activity. In sub-Saharan Africa, where HIV prevalence is very high, risky sexual behaviour of adolescents has even more severe consequences. Thus understanding patterns and motivations of early sexual debut, non-use of condoms, and multiple partnerships is an important contribution to HIV prevention strategies. From this study, which used data from more than 19,000 adolescents in four African countries, poverty appears to influence early sexual debut, especially among females, and the poor are less likely to be using condoms. Therefore, poverty, by influencing sexual behaviour and access to services, can influence the transmission of HIV infection. Ethnicity is an important variable indicating that social and cultural factors do influence young people's sexual behaviour. HIV prevention programmes must identify ways of making the poor less vulnerable to risky sexual behaviour and devise strategies for improving condom usage among the poorest. Such programmes need to take account of strong social and cultural contexts that influence young people's sexual behaviour. Acknowledgements All three authors were funded by a sub-contract from a National Institutes of Health (NIH-NICHD Sub-Contract R.24 HD43610-01) to the African Population and Health Research Center through the Guttmacher Institute. In addition, Nyovani Madise was funded by the University of Southampton during the conceptualization of the project. The paper was written when all the three authors were employed at the African Population and Health Research Center. The authors are grateful to all partners involved in the Protecting the Next Generation Project and colleagues at the African Population and health Research Center for their comments on earlier versions of this paper. References
© Copyright 2007 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh07036t5.jpg] [rh07036t4.jpg] [rh07036t2.jpg] [rh07036t3.jpg] [rh07036t1.jpg] [rh07036f3.jpg] [rh07036f1.jpg] [rh07036f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}