 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 11, No. 3, December, 2007, pp. 99-110 Adolescents' views of and preferences for sexual and reproductive health services in Burkina Faso, Ghana, Malawi and Uganda Ann E. Biddlecom1 Alister Munthali2 Susheela Singh1 Vanessa Woog3 1Guttmacher Institute, New York, NY, United
States 2Centre for Social Research, University of Malawi, Zomba,
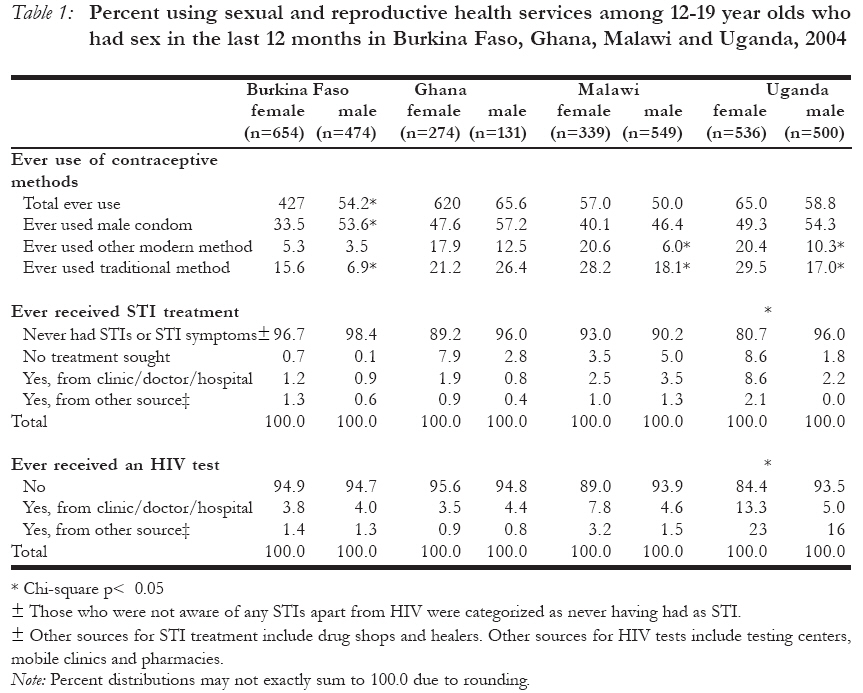
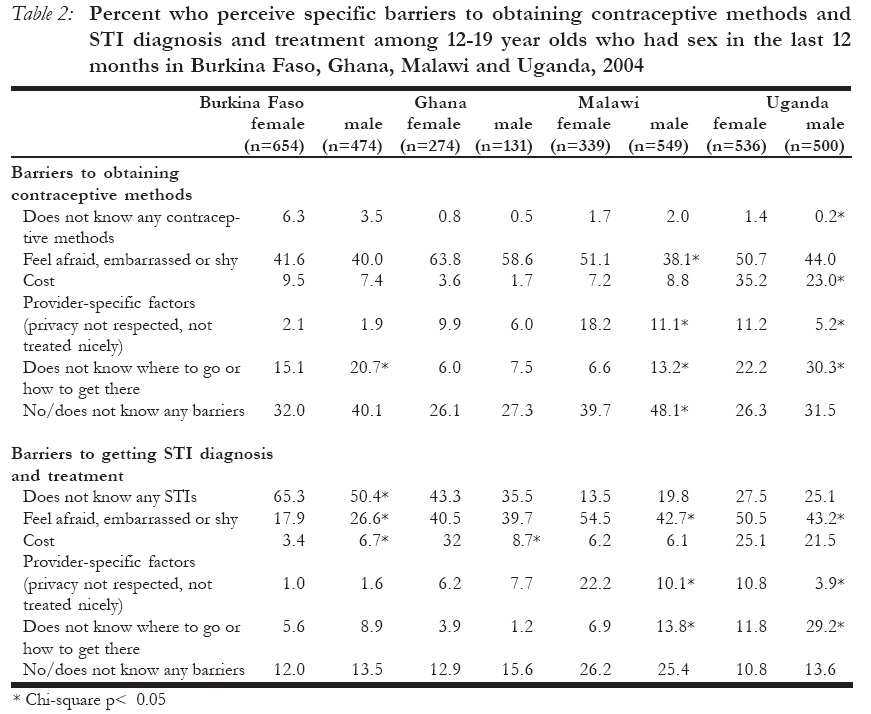
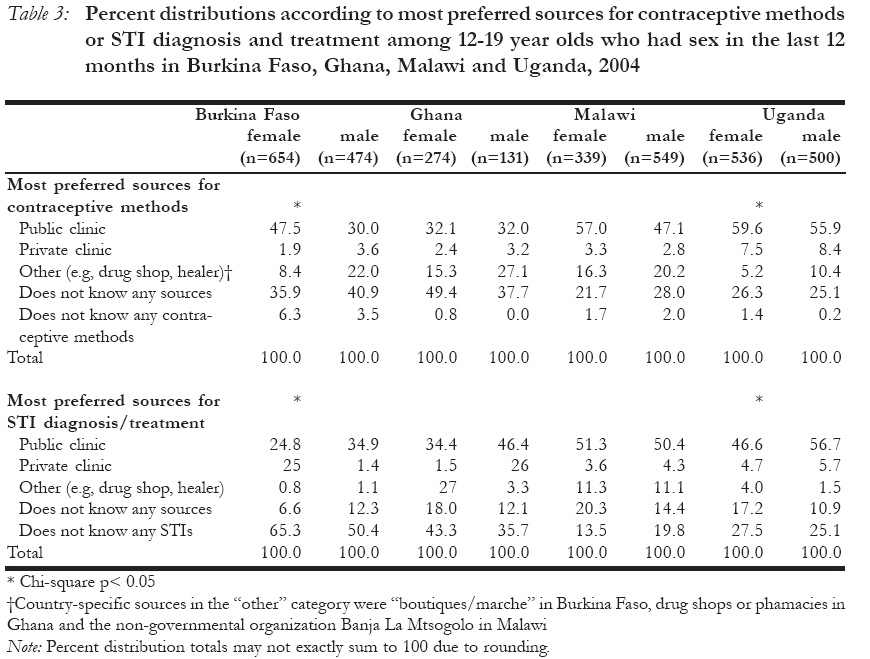
Malawi 3Consultant, New York, NY, United States Code Number: rh07037 Abstract Adolescents' views of and preferences for sexual and reproductive health services highlight promising directions and persistent challenges in preventing pregnancy and HIV and treating sexually-transmitted infections (STIs) in this population. Results from nationally-representative surveys of 12-19 year-olds in Burkina Faso, Ghana, Malawi and Uganda in 2004 show that contraceptive and STI services and HIV testing are still under-utilized. A substantial proportion of sexually-active adolescents do not know of any source to obtain contraception or get STI treatment, and social-psychological reasons (e.g., embarrassment or fear) and financial cost remain common barriers to getting services. Adolescents' preferences are overwhelmingly for public clinics, with strongly positive perceptions of confidentiality, accessibility and cost. Some gender and country differences exist, yet overall females and males' views are similar. Results highlight the need to inform youth about sources, increase availability of government health facilities and improve youth's access to them, especially by reducing social barriers. Résumé Opinions des adolescents sur, et leurs préférences pour, les services de la santé sexuelle et de reproduction au Burkina-Faso, au Ghana, au Malawi et en Ouganda. Les opinions des adolescents sur, et leurs préférences pour, les services de la santé sexuelle et de reproduction mettent l'accent sur les directions prometteuses et sur les défis persistants dans la prévention de la grossesse et du VIH et le traitement des infections sexuellement transmissibles (IST) dans cette population. Les résultats obtenus des enquêtes à represéntation nationale des adolescents âgés de 12 19 ans au Burkina-Faso, au Ghana, au Malawi et en Ouganda en 2004 montrent que les services des contraceptifs et des IST et le test de dépistage sont encore sous-utilisés. Une grande proportion des adolescents qui sont sexuellement actifs ne connaissent pas les sources pour obtenir la contraception ou le traitement pour les IST; ensuite, des raisons socio-psychologiques (l'embarras et la peur) et le coût financier demeurent des obstacles à l'obtention des services. Les préférences des adolescents sont largement pour des cliniques publiques avec leur fortes perceptions positives de la confidentialité, de l'accessibilité et du coût. Il existe aussi certaines différences au niveau des genres et des pays, pourtant, en général, les opinions des mâles et des femelles sont similaires. Les résultats mettent l'accent sur la nécessité de renseigner la jeunesse sur les sources, d'augmenter la disponibilité des établissements de santé et d'améliorer l'accès de la jeunesse à ces établissements, surtout par la réduction des obstacles sociaux. Key Words: Africa, Adolescent, Health Services Introduction Many young people in Sub-Saharan Africa face the risk of HIV, sexually-transmitted infections (STIs) and unintended pregnancy. Sub-Saharan Africa still remains the region with the highest percentage of people living with HIV (63%), and in 2005 an estimated 4.3% of 15-24 year old females and 1.5% of males in the region were HIV-positive.1 Incidence and prevalence data on STIs disaggregated by age and gender are limited, but a number of studies have shown higher prevalence of Chlamydia among younger than older girls and relatively high prevalence of herpes simplex virus-2 among adolescent girls in Tanzania and Uganda.2 Self-reported data from Demographic and Health surveys in Sub-Saharan Africa show that 1-11% of sexually-experienced 15-24 year old females and 2-16% of males in about 20 countries said they had an STI in the 12 months prior to the survey interview.3 In addition, unintended pregnancy is not uncommon among young people. Among 20-24 year old women, 8% in West/Central Africa and 15% in South/East Africa have had a premarital birth by age 20.4 While data are very limited on abortion, estimates of unsafe abortions in Africa show that more than one-quarter were experienced by 15-19 year olds.5 With such statistics, the needs of adolescents for a range of sexual and reproductive information and services are clearly substantial. In order to meet these needs, it is imperative that data from young people themselves be used to inform changes to existing health care systems or to design new interventions. Prior studies in Sub-Saharan Africa have described young people's perceptions and use of health services, but they have a variety of limitations: some address one type of need (for example needs related to contraception but not STIs),2;6;7 cover a small geographic area, are based on selective samples, for example people who attend health facilities or who are students or are derived from qualitative methodologies that by their nature cannot be representative of the cross-section of adolescents.8-11 For example, facility-based information on family planning clients in African countries shows few clients are under age 20 (ranging from a low of 1% of clients in Nigerian sites to a high of 13% in Botswana, the latter a country where a relatively large percentage of clients were also not in marital or consensual unions).12 However, these statistics are based on individuals who have already shown up at a clinic for family planning, a sub-set of the larger population of adolescents who are sexually-active and want to delay or avoid pregnancy. A large part of the literature on adolescents and sexual and reproductive health services has focused on adolescents' perceived barriers to obtaining services. Major barriers that adolescents say they face are fear that others might get to know of their visit, shame about their needs, negative attitudes of providers, lack of privacy and confidentiality and age restrictions.11;13-16 National, comprehensive information on adolescents' views of and preferences for sexual and reproductive health services is much less common. Information from adolescents themselves on actual service utilization and about preferences and perceptions concerning sources is critical for helping determine the types of interventions and policies that could be implemented to improve adolescent sexual and reproductive health. For example, one approach to improving adolescent utilization of sexual and reproductive health services has focused on making services more youth-friendly in part through training of existing providers, facility-based changes (e.g., setting up a separate space for young clients) or incorpo-rating peer-based outreach or young workers on staff. A study based on data from 10-19 year olds in Kenya and Zimbabwe showed that adolescents considered youth-only services, youth involvement in services and young staff as the least important characteristics of services while characteristics generally applicable to the existing health care system—confidentiality, short waiting time, low cost and friendly staff—were rated as the most important.17 The authors suggest that some aspects of making services more youth-friendly—particularly separate facilities dedicated to young people or the involvement of young people in running a program—may perhaps not be as wise an investment as focusing on more structural changes. This article reports on findings from nationally-representative surveys of 12-19-year-olds in Burkina Faso, Ghana, Malawi and Uganda conducted in 2004, on adolescents' use of sexual and reproductive health services, the barriers they face in accessing such services, and their opinions and preferences regarding different sources of care. These surveys are comparable across countries, and notably include very young adolescents 12-14, as well as providing comparable information for male and female adolescents. Three major categories of sexual and reproductive health services are addressed—contraception, STI care, and HIV prevention—because they are highly interconnected: adolescents need to prevent unintended pregnancy, STIs and HIV, and facilities often offer a range of services, and may increasingly want to do so. The four countries reflect three different sub-regions of Sub-Saharan Africa, notably Southern Africa, East Africa and West Africa, both Anglophone and Francophone countries, and a range of HIV prevalence levels among young adults (e.g., in 2005 for Burkina Faso and Ghana an estimated 1.3-1.4% of young women (15-24 years old) were HIV-positive, rising to 5.0% in Uganda and 9.6% in Malawi).1 Given the variation in contexts represented by the four countries, the results increase understanding of these issues for these three sub-regions though they do not exhaustively represent the variation that may exist within each sub-region or across Sub-Saharan Africa as a whole. The analysis focuses on common patterns and differences across the four countries rather than addressing differences within countries. Gender differences will be highlighted in order to show the degree to which female and male adolescents may (or may not) need to be targeted differently in improving health service utilization. Methods Nationally-representative, household-based surveys of female and male 12-19-year-olds were conducted in early to mid-2004 in Burkina Faso, Ghana, Malawi and Uganda. Four districts in the Northern region of Uganda had to be dropped from the sample due to security concerns during fieldwork. A first-stage systematic selection of enumeration areas was made in each country, and a second stage selection of households per enumeration area was made from a household listing. All 12-19 year old de facto residents in each sampled household were eligible for inclusion in the survey. Informed consent was sought from 18-19-year-olds. Consent from a parent or caretaker was first obtained for adolescents aged 12-17 years before the eligible minor adolescent was then approached for assent to participate in the survey. Interviews were completed with 5,955 12-19-year-olds in Burkina Faso, 4,430 in Ghana, 4,031 in Malawi and 5,112 in Uganda. The overall individual response rate ranged between 86.6% (Uganda) and 95.2% (Burkina Faso). Detailed information about the survey samples and methodology is publicly available.18 19-21 Adolescents were asked separate questions about preventing pregnancy, STIs and HIV. Knowledge of specific contraceptive methods was obtained via standard, prompted questions used in Demographic and Health Surveys. For those who had heard of contraceptive methods, open-ended questions were asked about 1) barriers to getting methods, 2) whether the respondent knew of places where young people can get contraceptive methods and types of places known, and 3) where the respondent would most prefer to go to obtain contraceptive methods. A separate set of questions was asked about STIs: whether the respondent had heard of any infections (apart from HIV) people can get from sexual contact, had ever had an STI or STI symptoms and, if yes, what kind of treatment was last sought, if any. Respondents who said that they ever had an STI or who answered "yes" to at least one of two direct questions about common STI symptoms (ever had a bad-smelling, abnormal discharge; ever had a genital sore or ulcer) were categorized as having had an STI. Those who were not aware of any STIs apart from HIV were categorized as never having had an STI in order to describe all adolescents and not just those who ever heard of STIs. Questions about barriers to health services and service sources known and preferred for contraceptive methods were also asked regarding advice and treatment for STIs. Finally, questions were also asked about awareness of HIV, whether the respondent had heard that people can get tested for HIV, and questions about types of places they knew for testing and where they themselves have been tested. Adolescents who had not heard of HIV or a test for HIV were classified as having never received a test. All measures are shown for sexually-active male and female 12-19-year-olds, as they are arguably more in need of such services given their possible exposure to unplanned pregnancy, STIs and HIV than adolescents who are not currently sexually-active. Current sexual activity was defined as having had sexual intercourse in the 12 months prior to interview. Percentage distributions and Chi-square tests of gender differences were calculated using STATA 9 for each measure by country with adjustment for the stratified, cluster sample design. Results Use of sexual and reproductive health services Table 1 shows that among 12-19-year-olds who had sex in the last 12 months, ever use of any contraceptive method ranged from 43-65% among females and 50-66% among males. The vast majority of contraceptive method use reported by both females and males was the male condom. Use of modern methods apart from the male condom was much less common, and in all four countries it was lower than use of traditional methods (mainly rhythm and withdrawal): 16-30% of sexually-active females and 7-26% of males had ever used traditional methods. Females in all countries but Ghana were significantly more likely than males to report having ever used a traditional method. The majority of sexually-active adolescents reported never experiencing an STI or STI symptom1 (ranging from 81% in Uganda to 97% in Burkina Faso for females and from 90% in Malawi to 98% in Burkina Faso for males). Among sexually-active adolescents with STIs, the proportion not seeking any care was quite large _ more than two-thirds in Ghana, about half in Malawi and just under half in Uganda; in Burkina Faso, the proportion reporting ever having an STI was smallest (2-3%) but most of these youth obtained some care. In Ghana, Malawi and Uganda, among those who obtained treatment, clinics, hospitals or doctors were much more likely to be the source contacted rather than other types of providers (including traditional healers). For example, in Uganda of the 11% of sexually-active females who ever had an STI or STI symptom and obtained some care, 9% last sought care from a doctor, clinic or hospital while 2% sought care from another source such as a drug shop or traditional healer. Of course, health care seeking can involve many steps and multiple types of providers may have been contacted, which would not have been captured by these survey questions.22 For example, focus group discussions with 14-19-year-olds in the four countries about STI-related health services found that traditional healers and herbalists were as commonly mentioned as hospitals and public clinics because they were believed by some to provide confidential services, fast and effective treatment and to allow patients to pay in installments.8 Overall, there were no significant differences between females and males in their experience of STIs or STI symptoms and health-seeking behavior in all the countries except Uganda. The last panel of Table 1 shows that between 4-16% of sexually-active female 12-19-year-olds and 5-7% of males have ever been tested for HIV. As with STI treatment, when they did get tested the majority went to a public clinic or hospital rather than other sources, such as mobile clinics or stand-alone testing centers. HIV testing was higher in Malawi and Uganda—mirroring the longer history of high HIV prevalence rates—16% of sexually-active girls in Uganda and 11% in Malawi ever received an HIV test compared to no more than 5% of sexually-active girls in Burkina Faso and Ghana. Differences were not as large among sexually-active boys in the four countries. There are also significant gender differences in Uganda: more females have received an HIV test than males, probably related to testing in the context of pregnancy-related care. Barriers to using sexual and reproductive health services Sexually-active adolescents reported very similar perceptions of barriers to getting contraceptive methods as they do for STI diagnosis and treatment (note that adolescents in the survey could name more than one barrier). Table 2 shows that feeling afraid, embarrassed or shy to seek such services—a barrier rooted in the social context surrounding adolescent sexuality—was one of the most common barriers named among sexually-active adolescents for obtaining contraceptive methods: 42-64% of sexually-active females and 38-59% of sexually-active males mentioned this as a barrier. More females than males reported feeling afraid, embarrassed or shy about obtaining either contraceptive services or STI treatment, but this difference was only statistically significant in Malawi and Uganda and the reverse pattern was true in Burkina Faso (though this was related to the fact that a larger proportion of female adolescents do not know about STIs, compared to males). The cost of services and not knowing where to go were also important barriers to obtaining contraceptive methods in some countries, especially in Uganda, though still not as formidable as the social-psychological barriers. Compared to females, significantly more males in all countries but Ghana reported that they did not know where to go for either STI or contraceptive services. In regard to contraceptive services, factors directly related to providers—an adolescent's privacy not being respected or not being treated nicely by staff—were mentioned by a minority of sexually-active 12-19 year olds in three of the four countries: 10-18% of females and 5-11% of males in Ghana, Malawi, and Uganda. In Uganda and Malawi, females were more likely than males to perceive provider-specific barriers in terms of both STI and contraceptive services. Although about at least half, and as much as three in four sexually-active 12-19-year-olds in these four countries reported that they perceived having one or more barriers, one-quarter or more reported that they either did not have or did not know of any barriers to obtaining contraceptive services. Barriers to STI diagnosis and treatment were very similar to those for obtaining contraceptive services with one exception: while awareness of contraceptive methods per se was not a problem, a substantial proportion of sexually-active young people said they were not aware of other infections apart from HIV that people can get from sexual contact. The proportion of sexually-active 12-19-year-olds who have not heard of an STI was highest in Burkina Faso (65% of females and 50% of males), moderate in Ghana and Uganda and lowest in Malawi (14% of females and 20% of males). Where there were notable associations between awareness and gender, it was typically the case that fewer sexually-active females were aware of contraceptive methods or STIs than males. Preferences for different sources The most preferred sources of contraceptive methods among both female and male adolescents were public health facilities (clinics or hospitals) over other types of services (Table 3). Other sources such as drug shops were more preferred by males than females, though clinics were still the most commonly preferred among all adolescents. Similar patterns were found for sources for the diagnosis and treatment of STIs: overwhelmingly, public facilities were the most preferred sources of STI services in all four countries. In all four countries, very few adolescents said that they preferred private clinics for either contraceptives or STI treatment (8% or less), most likely because of cost. Table 3 also shows that a substantial proportion of sexually-active young people did not know of any source to obtain contraceptive methods, ranging between 22% of sexually-active females in Malawi and 49% in Ghana and between 25% of sexually-active males in Uganda and 41% in Burkina Faso. This group overlaps somewhat with the group in Table 2 who said they did not know about or did not think there were barriers to obtaining contraceptives (e.g., ranging from about one-quarter in Ghana to two-thirds in Malawi, data not shown), a particular sub-group who may not be very motivated to seek contraceptives for other reasons. In the case of STI services, in addition to the large proportion who have never heard of STIs (especially large in Burkina Faso and Ghana), another 7-20% of sexually-active adolescents in all four countries said they do not know of a place to go for such services. Only in Burkina Faso and Uganda were there significant gender differences in awareness and preferences for contraceptive and STI sources. Perceptions of government clinics and hospitals Adolescents who knew of a government clinic or hospital for contraceptive methods or STI treatment were asked their opinion of the quality of services from this type of provider. Clinics and hospitals were evaluated on their confiden-tiality, physical accessibility, level of respect with which they treat their patients and cost. Overall, a very large majority of adolescents viewed the formal health system in positive ways. For example, in Ghana 85% of sexually-active female adolescents (who knew of clinics or hospitals for contraceptive methods) felt they were a confidential source and 80% felt that young people were likely to be respected there. Seventy-nine percent thought they would be able to easily reach a clinic or hospital and 66% thought they could pay for the cost. Among all four dimensions, ability to pay for services (either for contraceptive methods or STI advice/treatment) was the dimension with the fewest female and male adolescents holding a favorable view. But even on this aspect of care, 60-86% felt that they would be able to pay for services (varying across gender and country). Even though there may be some bias towards adolescents providing positive responses in the survey interview, these proportions are so high that the results point toward the conclusion that adolescents generally have positive expectations of government health facilities. There were no consistent, significant gender differences in adolescents' views of government clinics and hospitals across the four countries on any of these dimensions. Discussion This paper presents new, nationally-representative evidence of 12-19-year-olds' use of, barriers to and preferred sources of sexual and reproductive health services in Burkina Faso, Ghana, Malawi and Uganda. The data show that pregnancy and STI prevention and treatment services and HIV testing are all under-utilized among sexually-active adolescents. Many sexually-active youth are not well prepared to prevent pregnancy as evidenced by the large proportion of sexually-active young people who never used a contraceptive method (either modern or traditional). In addition, overall, a large proportion of those who ever experienced an STI or STI symptoms did not seek treatment, whether from a traditional or modern source. Other studies on the health-seeking behavior of adolescents for STIs have indicated that young people tend to delay treatment because of the lack of perceived seriousness of the symptoms or because they prefer to resort to self-treatment.2;6 Nonetheless, the findings presented here suggest that many sexually-active young people do not use contraception or seek treatment for an STI because of lack of knowledge about places for getting methods or STI treatment, lack of awareness of STIs themselves or because of perceived barriers in accessing health services. The evidence on lack of knowledge shows that there is great need for more widespread provision of information on STIs and their symptoms, and on sources from which relevant services for either STIs or contraceptives may be obtained. While increasing the provision, quality and coverage of sex education within schools is one important means of improving adolescent's knowledge of prevention of unintended pregnancy and HIV, other avenues must be pursued to reach those who drop out of school or never attend school, to deepen and reinforce the information that is provided within schools and to link adolescents who need services with the places that provide them. The results from the present study show that the most common barrier for young people to obtaining either contraceptive methods or STI diagnosis and treatment is social stigma (e.g., fear or embarrassment) and to a significant but lesser degree, cost, provider characteristics and lack of knowledge about service sources. These barriers are echoed in a number of other studies2;8;9;14 and highlight the need to better address the obstacles that continue to persist over time and context across all types of sexual and reproductive health services. In particular, the social stigma attached to service utilization may partly explain why young people's needs to access reproductive health services are not being optimally met. For example, a recent analysis of in-depth interviews with adults in Burkina Faso about their perceptions of adolescent sexual and reproductive health problems found that although adults were very supportive of young people accessing reproductive and sexual health information, they were less accepting of young people accessing reproductive health services.23 Evaluations of interventions to make clinical services youth-friendly generally show that this on its own does not bring about increased utilization by young people, although one study found that satisfied clients tended to return for ongoing care.24;25 Facility-based or provider-based improvements alone are likely to be insufficient since social stigma is common and not solely limited to the clinic setting. For example, an intervention of youth-friendly clinic services in Zambia concluded that positive changes in social and community-level factors played an important role in improving adolescents' use of reproductive information and services as did making the services more youth-friendly.15 Moreover, a systematic review of interventions to improve adolescent health care utilization showed that interventions that combined training of clinic staff, facility-based improvements and community-based activities to inform and mobilize support among the general population had a sufficient level of evidence of effectiveness to be recommended for widespread implementation.25 This study found that sexually-active adolescents strongly prefer public health facilities as the source of contraceptive methods and STI treatment. In addition, adolescents view these facilities favorably in terms of confidentiality, physical accessibility, being treated with respect and, to a lesser degree, financial affordability. A few other studies have addressed the service preferences of sexually-active young people and have found that some young people prefer and rely on the informal sector (such as a traditional healer) because of the lower costs, assured confidentiality and privacy and quick service delivery while others turn to self-medication for STIs.2;7;9;10;15 These findings are seemingly inconsistent with the new survey evidence presented here showing that a larger proportion obtain and prefer to obtain services from modern sources than from traditional sources. However, it is possible that young people may be using both "modern" and "traditional" health care sources following the same patterns of health-seeking behavior as their other family members, though they may prefer modern sources. Adolescents may also try several means at once or go through sequential steps to treating a health problem through self-medication and visits to the informal and formal health sector. For example, a study in southern Malawi showed western medicines, especially antibiotics, were widely used as a preventive measure for STIs in order to avoid visible signs and symptoms of a sex-related disease and, as a consequence, the shame and gossip that ensues from having an STI.26 The use of traditional medicines or medicines purchased from shops may actually cause delays in seeking appropriate care from a clinic or hospital until the condition has worsened. While the evidence presented describes the national situation for sexually-active female and male 12-19 year olds in four different countries, and reveals important differences between male and female adolescents, the gap between needs and access may vary even more widely among specific population groups within countries, such as by rural or urban residence or being in or out of school. Additional research that examines differences in service use, barriers and preferences among key socio-demographic groups can inform resource prioritization and help direct program efforts to reach especially neglected sub-groups of adolescents. 1Those who had never heard of STIs are classified as never having received treatment. Acknowledgements We are grateful for comments by Nyovani Madise, editorial assistance by Kate Patterson and contributions to the overall study from colleagues at the Guttmacher Institute (United States), University of Cape Coast (Ghana), Institut Supérieur des Sciences de la Population (Burkina Faso), African Population and Health Research Center (Kenya), Centre for Social Research (Malawi) and the Makerere Institute of Social Research (Uganda). Authorship is alphabetical. This study was supported by The Bill & Melinda Gates Foundation, The Rockefeller Foundation and the National Institute of Child Health and Human Development (Grant # 5 R24 HD043610). Reference
© Copyright 2007 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh07037t3.jpg] [rh07037t4.jpg] [rh07037t1.jpg] [rh07037t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}