 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
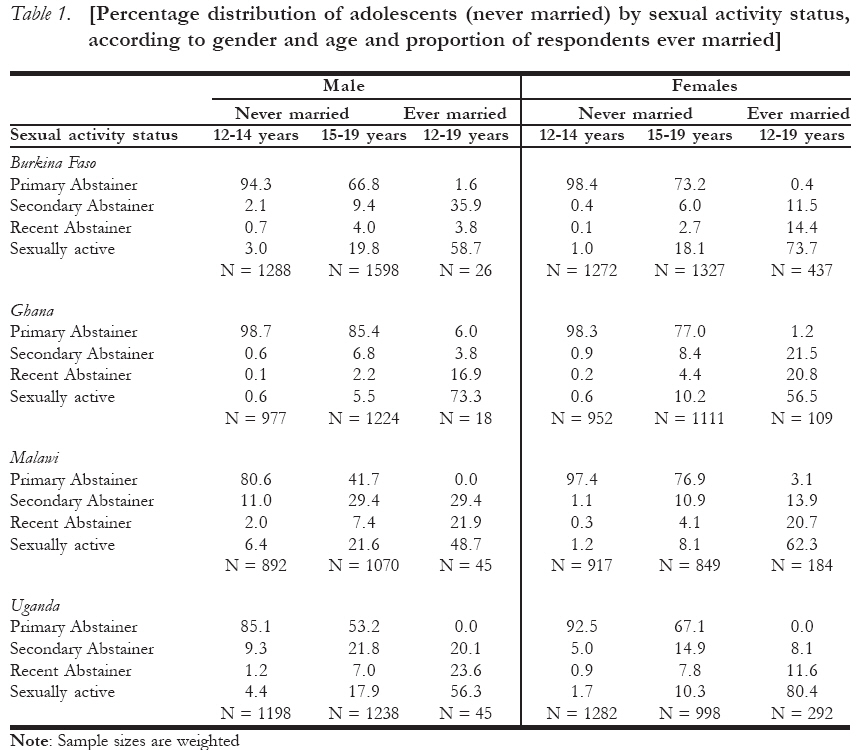
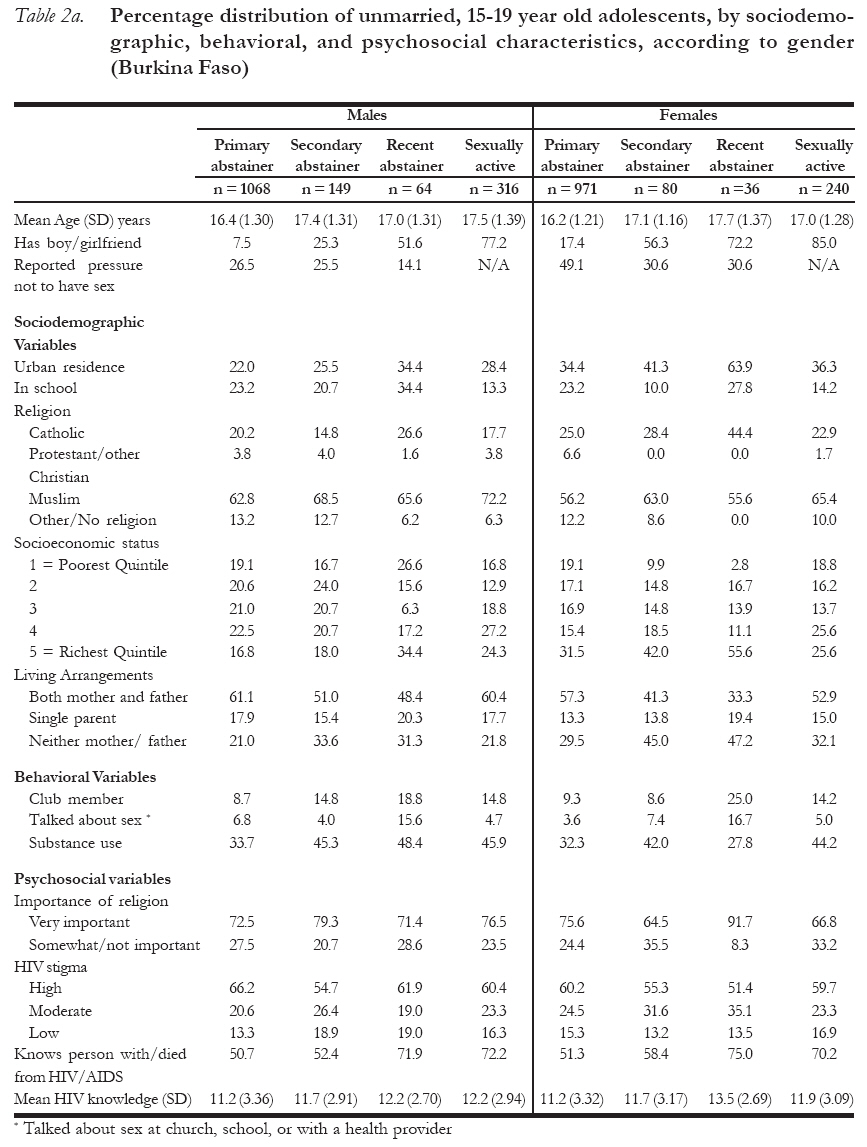
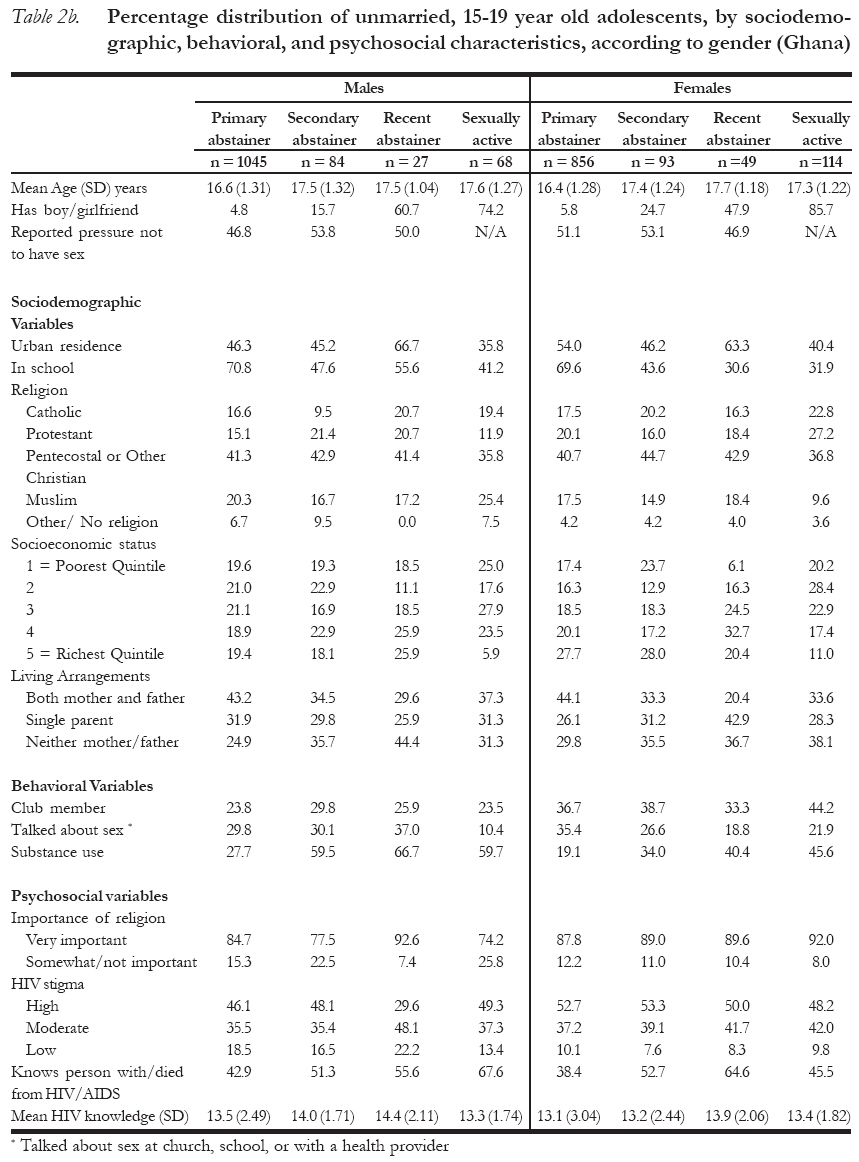
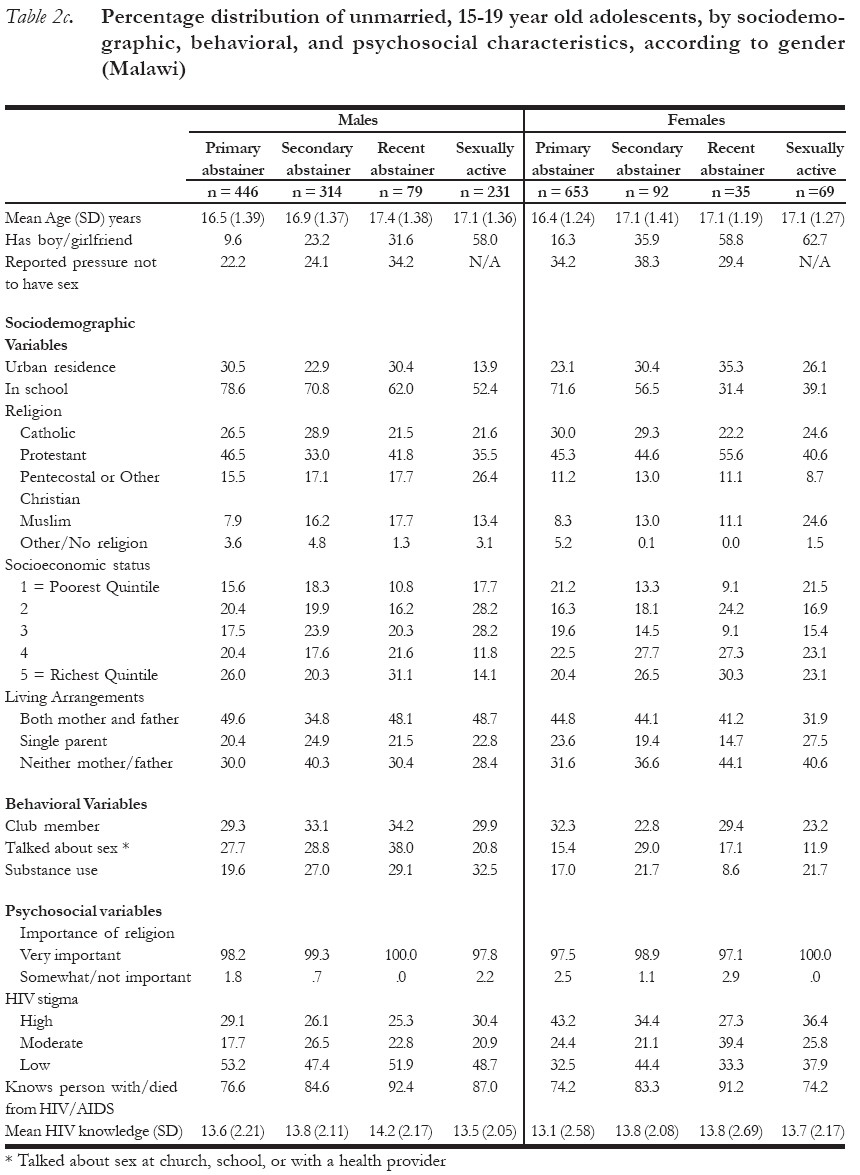
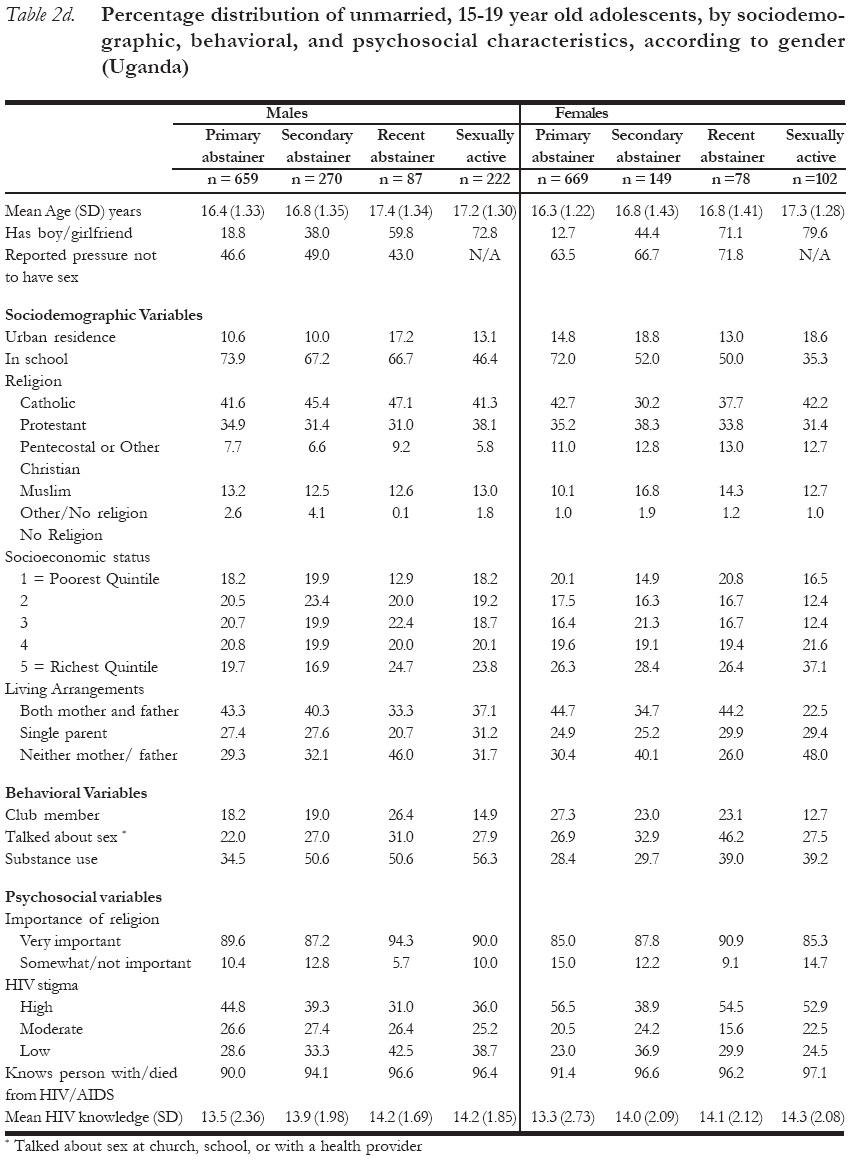
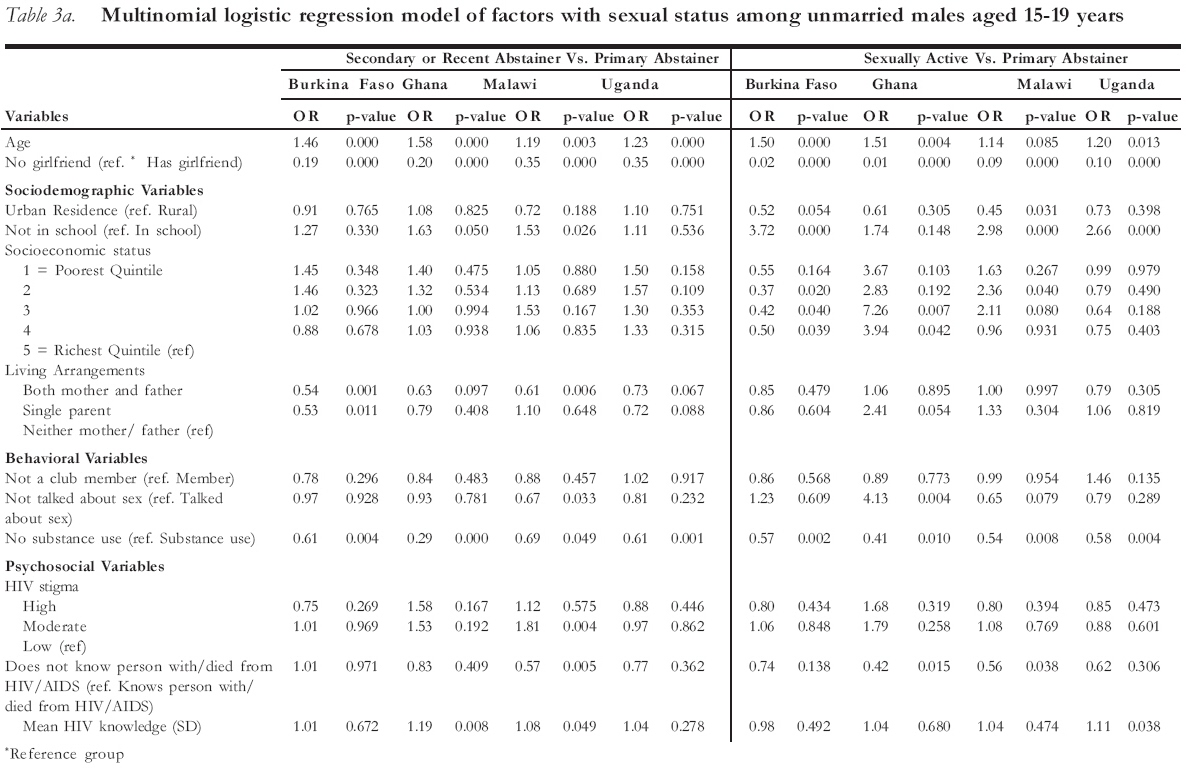
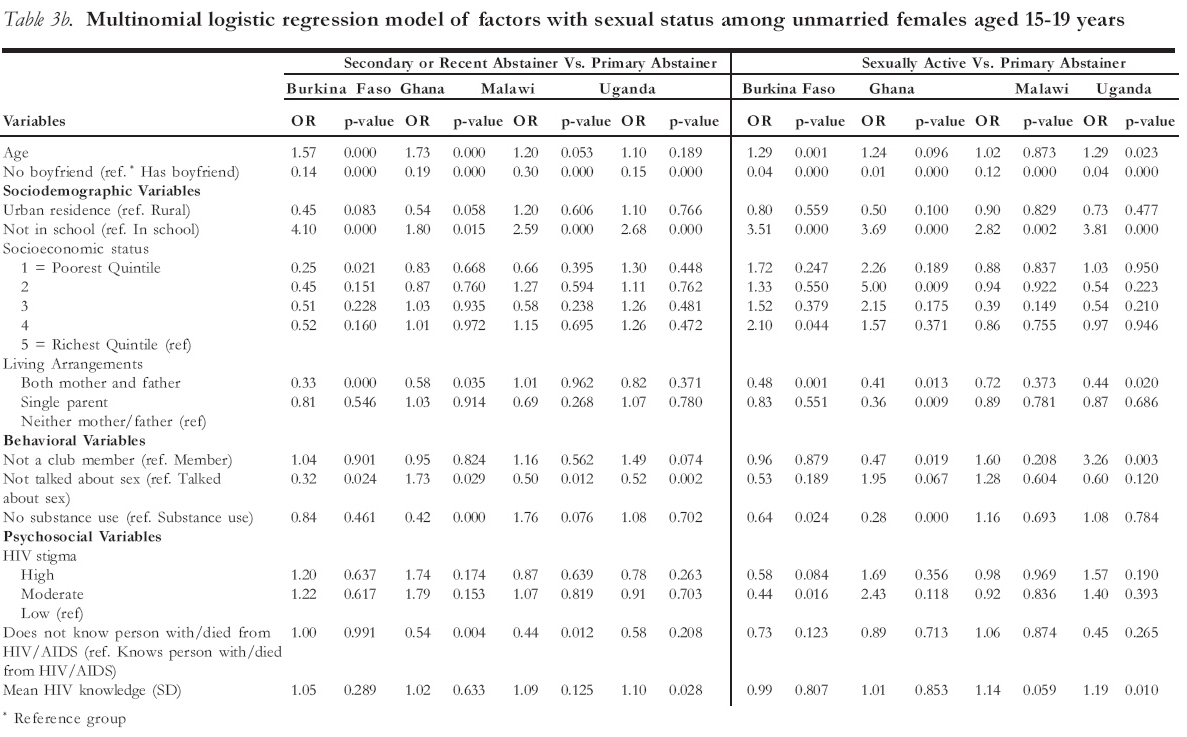
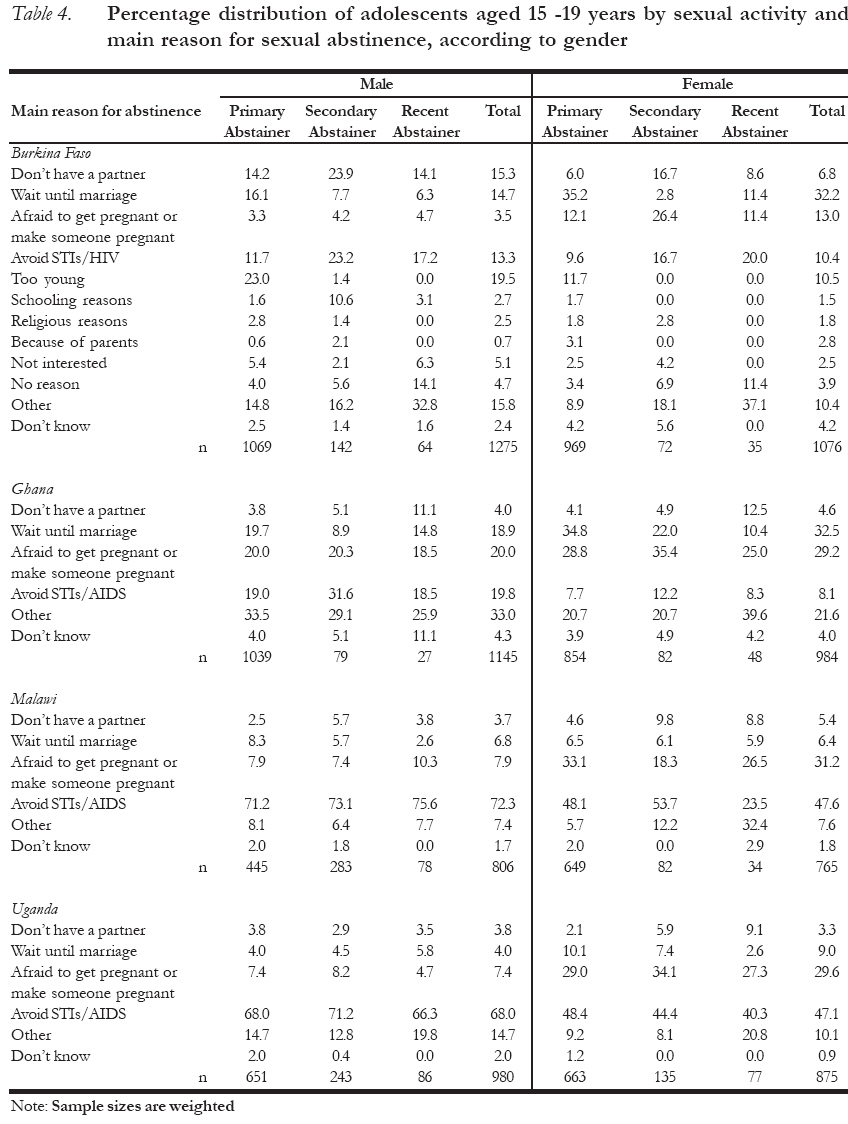
African Journal of Reproductive Health, Vol. 11, No. 3, December, 2007, pp. 111-132 Factors Associated with Sexual Abstinence among Adolescents in Four Sub-Saharan African Countries Caroline W. Kabiru1 and Alex Ezeh1 1African Population and Health Research Center. Shelter Afrique Center, 2nd Floor Longonot Road, Upper Hill. P. O. Box 10787, 00100 _ G.P.O. Nairobi, Kenya Telephone: +254-20-2720400/1/2 Code Number: rh07038 Abstract Drawing on nationally representative data collected from Burkinabé, Ghanaian, Malawian, and Ugandan adolescents, this study examines differences among four groups of never married, 15-19 year olds: primary abstainers (sexually inexperienced), secondary abstainers (last sex more than 12 months prior to the survey), recent abstainers (sexually active in last year but not in the last 3 months), and sexually active (had sexual intercourse in the last 3 months). The percentage of primary abstinent adolescents ranged from 42% (Malawian males) to 85% (Ghanaian males). In general, a greater proportion of females than males were primary abstainers. Primary abstainers were younger than sexually experienced adolescents. Current involvement in a romantic relationship was a significant predictor of sexual status with primary abstainers being the least likely to be romantically involved. Overall, findings suggest that adolescents' gender, prior sexual experiences and contextual circumstances, such as romantic partnerships, should be considered when designing abstinence promotion programs. Résumé Facteurs liés à l'abstinence sexuelle chez les adolescents dans quatre pays d'Afrique subsaharienne En se fondant sur les données à représentation nationale recueillies auprès des adolescents burkinabe, ghanéens, malawiens et ougandais, cette étude examine les différences entre quatre groupes d'adolescents qui n'ont pas été jamais mariés, âgés de 15-19 ans: les abstentionnistes primaires (sexuellement inexpérimentés), les abstentionnistes secondaires (le dernier rapport sexuel compte plus de 12 mois avant l'enquête), les abstentionnistes récents (sexuellement actifs au cours de l'année passée mais pas au cours de trois derniers mois) et sexuellement actifs (ont eu des rapports sexuels au cours de trois dernier mois). Le pourcentage des adolescents de la catégorie de l'abstinence primaire variait de 42% (les mâles malawiens) à 85% (les mâles ghanéens). En général, une plus grande proportion de femelles par rapport aux mâles étaient des abstentionnistes primaires. Les abstentionnistes primaires étaient plus jeunes que les adolescents sexuellement expérimentés. L'implication actuelle dans un rapport romantique est un indice significatif de la situation sexuelle chez les abstentionnistes primaires qui ont la moindre possibilité d'être impliqués romantiquement. Dans l'ensemble, les résultats montrent que le genre des adolescents, les expériences sexuelles antérieures et les circonstances contextuelles, telles les associations romantiques, doivent être prises en considération pour la conception des programmes de la promotion de l'abstinence. Key Words: Adolescents, Sexual abstinence, Sexual activity, Sub-Saharan Africa Introduction Adolescence, a transitional period of physical, emotional, and social maturation, is often characterized by the clarification of sexual values and experimentation with sexual behaviors 1. Early initiation of sexual activity among adolescents has been identified as a major risk factor for a number of negative reproductive health outcomes, including early childbearing and associated implications for maternal and child health outcomes, as well as increased risk for sexually transmitted infections (STIs) including HIV. The need to safeguard adolescent sexual health has fueled much research on factors that predispose adolescents to risky sexual behaviors including unprotected sexual intercourse, early sexual debut, and multiple sexual partnerships. At the same time, a number of programs have been designed to address adolescent sexual health with a focus on delaying sexual initiation, promoting secondary virginity, and increasing condom use among those who are sexually active2, 3. Abstinence, one of the key actions recom-mended for the prevention of sexually transmitted infections and early pregnancy among young people4, 5, has received much focus in HIV and reproductive health programs. In the United States, for example, sexual abstinence programs have received increased emphasis following the 1996 allocation of 250 million dollars by Congress for school-based abstinence education programs6, 7. In 2002, President George Bush also pushed for abstinence-based programs by requesting an additional 30 million dollars for these types of programs8. According to the federal legislation under which the funding is provided (the Personal Responsibility and Work Opportunity Recon-ciliation Act), there are eight principles underlying abstinence education in the United States: 1) abstinence yields social, psychological, and health benefits; 2) sexual abstinence is the expected standard for children in school; 3) sexual abstinence is the only 100% effective way to prevent pregnancies outside marriage, STDs, and other risks arising from sexual intercourse; 4) sexual activity should occur in a mutually monogamous relationship within marriage; 5) negative psychological and physical effects are likely to occur as a result of sexual intercourse outside of wedlock; 6) having children outside marriage is likely to have negative effects for the child, parents, and society; 7) there is a need for the youth to be taught sexual refusal skills and to learn how drug use, including alcohol use, impairs judgment about sexual activity; and 8) young people should be self-reliant before being sexually active9, 10. These principles have been assumed to be universally applicable and have guided the development of similar programs in the developing world, including sub-Saharan Africa11. Abstinence, especially among unmarried youth, is a key component of the ABC (Abstain, Be faithful, and use Condoms) approach adopted by the President's Emergency Plan for AIDS Relief (PEPFAR)12, an international health program funded by the United States government to address the HIV/AIDS pandemic in severely affected countries including Ghana, Malawi, and Uganda. While there is much support for the promotion of sexual abstinence among the youth, there is a paucity of studies that examine characteristics of young people who choose to abstain from sexual intercourse. Thus, much less is known about the reasons why some adolescents decide to abstain from sexual intercourse than about factors that predispose the youth to risky sexual behaviors13, 14. Nonetheless, young people may choose to delay sexual intercourse due to individual, socio-cultural, and other contextual factors that, if better understood, can substantially inform HIV, STI, and early pregnancy prevention messages9. Abstinence in the ABC approach focuses on unmarried adolescents urging them to wait until marriage before engaging in sexual intercourse12. Many faith-based organizations with funding from PEPFAR advance this position. If their message is having an impact, one would expect many adolescents to reflect this impact as "pressure to abstain from sex". In addition, if the programs are effective in promoting abstinence, one would also expect those experiencing greater pressure to abstain to actually abstain, controlling for age and other covariates. However, it is also possible that adolescents who are perceived as being sexually active, especially in the face of strong normative control over non-marital sex, may receive more attention and pressure to abstain. Again, if abstinence interventions are effective, we would expect them to promote secondary abstinence among those who are sexually experienced. There are reasons to expect that primary, secondary and recent abstainers may be abstaining for different reasons. Primary abstainers may have strong moral or religious basis for their action and may believe sexual intercourse should only occur within the context of marriage. Secondary abstainers, however, may be driven more by a desire to avoid STIs, including HIV, or pregnancy while recent abstainers may simply be abstaining due to lack of opportunity to engage in sexual intercourse rather than as a conscious choice to abstain. There may also be differences between adolescent males and females. For instance, while female adolescents may be more motivated to abstain due to a desire to avoid pregnancy, male adolescents may desire to avoid STIs/HIV. Also, in countries with high HIV prevalence, fear of HIV infection may take center stage in adolescents' reasons for abstaining while such a reason may not be as important in a low prevalence setting. These differences, if they exist, may be powerful in designing relevant and appropriate programs and strategies for reaching different groups of adolescents. Using data collected from Burkinabé, Ghanaian, Malawian, and Ugandan adolescents, this study has two aims. First, the study examines differences in the profiles of unmarried adolescent males and females by their sexual status. We try to answer the following questions: 1) apart from age and gender which are known to influence adolescent sexuality, are there other factors that systematically differentiate primary abstainers from secondary and recent abstainers and currently sexually active adolescents? Are these factors related to key program efforts targeting adolescents? Second, for sexually abstinent adolescents, are the reasons for abstaining different for primary, secondary and recent abstainers and how can such differences inform strategies to reach different types of abstaining adolescents? Methods Country Contexts The study was conducted in four sub-Sahara African countries: Burkina Faso, Ghana, Malawi, and Uganda. Of the four countries, Malawi has the highest HIV/AIDS prevalence rate with an estimated 14% of 15-49 years olds reported to be living with HIV/AIDS in 200515. Adult (15-49 years) HIV prevalence rates are 2% in Burkina Faso and Ghana, and 7% in Uganda15. The vast majority of adolescents in these countries have engaged in sexual intercourse by the time they reach 20 years16-19 and are, therefore, greatly at risk for HIV infection as well as other negative reproductive and sexual health outcomes. All four countries have an extensive range of programs and services, offered by governmental and nongovernmental bodies, that are aimed at providing sexual and reproductive health information and services to young people16-19. Some of these programs advocate abstinence until marriage, such as the "National Catholic Committee to Fight AIDS" that is active in Burkina Faso17 and the "Why Wait?" educational program that was introduced in Malawian secondary schools in the 1990s and piloted in primary schools in the early 2000s18. Participants Data were collected from 5955 (2912 males, 3043 females) respondents in Burkina Faso, 4430 (2235 males, 2195 females) respondents in Ghana, 4031 (2033 males, 1998 females) respondents in Malawi and 5112 (2513 males, 2599 females) respondents in Uganda. All respondents were aged between 12 and 19 years. Since the specific objective of this paper is to examine differences in the profile of adolescents by their sexual status, the analyses were restricted to those who completed the questionnaire in sufficient detail to be categorized by sexual status (i.e. primary abstainerFNA, secondary abstainer, recent abstainer, and sexually active) and to those who had never been married. Close to 100% (N = 5948) of Burkinabé, 99% (N = 4391) of Ghanaian, 98% (N = 3957) of Malawian, and 99% (N = 5053) of Ugandan respondents had adequate data for classification. After excluding respondents who were currently or formerly married (see Table 1), the eligible numbers of respondents were 5485, 4264, 3728, and 4716 for Burkina Faso, Ghana, Malawi, and Uganda, respectively. Table 1 also summarizes the percentage distribution of never married adolescents by sexual activity status, according to gender and age. The table shows substantial differences in adolescent sexuality across the four countries. Among males, 94-99% of Burkinabé and Ghanaian respondents aged 12-14 years had never had sexual intercourse compared to 81% and 85% of similarly aged Malawian and Ugandan respondents. Approximately 20% of Burkinabé, Malawian and Ugandan males aged 15-19 years were sexually active in the three months preceding the study compared to only 6% of similarly aged Ghanaian males. In all four countries, over 90% of females aged 12-14 years had never had sexual intercourse. Among 15-19 year old unmarried female adolescents, about 10% were currently sexually active except in Burkina Faso where this proportion reaches 18%. In all countries, with the exception of Ghana, a greater proportion of males compared to females were sexually experienced. Also, female adolescents were 4 to 16 times more likely to have ever been married than male adolescents across the four countries. Burkina Faso had the highest proportion of ever married adolescents at 1 and 16% for males and females respectively while Ghana had the lowest at 1 and 5% respectively for male and female adolescents. Age is a key determinant of sexual debut20, 21. With increasing age, there is a larger proportion of young people reporting sexual activity and the median age at first intercourse is usually in the mid to late teens22. Among males in the sample, the median age at first intercourse was highest in Burkina Faso and Ghana at 15 years and lowest in Malawi and Uganda at 12 and 13 years respectively. Similar differences are not observed among females where the median age at first intercourse was 15 years in Burkina Faso, Malawi and Uganda and 16 years in Ghana. Given the low proportion of sexually experienced males and females aged 12-14 years in all the countries (except for males in Malawi and Uganda where the median age at first sexual intercourse was less than 15), all subsequent analyses are limited to 15 - 19 year olds. Study Design The data reported here were collected as part of the multi-year Protecting the Next Generation: Understanding HIV Risk among Youth study conducted in four sub-Sahara African countries: Burkina Faso, Ghana, Malawi, and Uganda, by the Guttmacher Institute, the African Population and Health Research Center, and their partners in each of the four countries to raise awareness on the sexual and reproductive health needs of adolescents. The study involved focus group discussions and in-depth interviews conducted with adolescents, parents/guardians, educators, and health professionals, as well as national surveys of adolescents. This study draws on the nationally representative adolescent surveys conducted in 2004. In all countries, the sample was selected in two stages: initial systematic selections of enumeration areas (EAs) or regional clusters within each country and at a second stage, households were chosen from each selected EA or cluster using a household listing. All 12-19 year olds who were usual residents of each sampled household were eligible for inclusion in the survey. The overall individual response rate by country was 87% in Uganda, 90% in Malawi, 92% in Ghana, and 95% in Burkina Faso. Data were collected using structured interviews. On average, interviews took around one hour in Ghana, Malawi, and Uganda and around 45 minutes in Burkina Faso. Questionnaires were translated and back-translated into local languages. Informed consent was obtained from all eligible adolescents. In addition, parental or guardian consent was obtained for adolescents younger than 18 years. Due to the sensitivity of the information sought from respondents, interviewers were gender-matched to respondents whenever possible. Further, care was taken to ensure privacy during interviews. Detailed descriptions of the study design, sampling and field procedures are publicly available22-25. Measures The questionnaire elicited responses on a wide range of variables including sociodemographic characteristics, family and social group characteristics, sexual activity, alcohol and drug use, and HIV/AIDS-related information. Outcome variables: The primary outcome variable is sexual status. Respondents were classified into one of four categories of sexual status: primary abstainers, or those who had never had sexual intercourse; secondary abstainers, or those who were sexually experienced but reported no sexual activity in the preceding 12 months; recent abstainers, or those who were sexually active in the past year, but not within the 3 months preceding the survey; and sexually active, or those who reported sexual activity in the preceding 3 months. Explanatory variables: Our main explanatory variables for sexual status are whether or not an adolescent has a boy or girl friend and whether they experienced any pressure from other people to abstain from sex. We expect that adolescents who are in romantic relationships will be more likely to be currently sexually active than abstaining, more likely to be a recent than secondary abstainer, and more likely to be a secondary than a primary abstainer. Also, adolescents who experience pressure to abstain will be more likely to be primary abstainers than secondary abstainers, more likely to be secondary abstainers than recent abstainers, and more likely to be abstaining than currently sexually active. We assess these associations controlling for a number of socio-demographic, behavioral, and psychosocial or cognitive factors known to influence adolescent sexuality21, 26, 27. The sociodemographic characteristics include respondent's age, schooling status at the time of interview, religious affiliation, and living arrangements. Socioeconomic status was measured using an asset index comprising the following: household assets and amenities (e.g. electricity, television, bicycle, car); household source of drinking water; type of toilet facility; type of cooking fuel; type of floor; ownership of home; and ownership of land. Principal components analysis was used to generate standardized weight scores which were summed to produce the household index score. Household scores were subsequently ranked to generate wealth quintiles. Behavioral variables include respondent's membership in a club or social group; whether they had ever talked about sex with a teacher/school, religious leader/church, or health provider; and whether they had ever consumed alcohol and/or used other mind-altering substances. Psychosocial or cognitive variables include perceived importance of religion in respondents' lives, HIV stigma, knowledge of someone living with or who died from HIV/AIDS, and HIV/AIDS knowledge. HIV stigma was assessed using a two-item scale (If a female teacher has the AIDS virus, should she be allowed to continue teaching in school? and If you know that a shopkeeper or food seller had the AIDS virus, would you buy fresh vegetables from him or her?). Respondents were then grouped into one of three groups representing low to high stigma. The internal reliability of the stigma scale using Cronbach's alpha ranged from 0.41 to 0.70 across the four countries. HIV/AIDS knowledge, on the other hand, was assessed using a 17-item scale (sample item: Can people get the AIDS virus from having sex with persons who are infected with the AIDS virus?). The internal reliability of the HIV/AIDS knowledge scale using Cronbach's alpha ranged from 0.62 to 0.77 across the four countries. Reasons for abstinence: All sexually inexperienced respondents and sexually experienced respondents who did not report sexual activity in the 3-months preceding the survey were asked to state reasons why they had not engaged in sexual intercourse. In a separate question, respondents were also asked to state the main reason why they were abstinent. Responses to this question were used to examine differences in reasons for sexual abstinence among adolescents in different sexual abstinence categories. Analyses Basic univariate statistics (means, standard deviations, and frequency counts) were computed for all variables. Cross tabulations (for categorical explanatory variables) and analysis of variance (ANOVA) (for continuous explanatory variables) were computed to examine differences across respondents based on sexual status. The criterion for statistical significance was 0.05. Multinomial logistic regression models were employed to examine the net effects of our key explanatory variables on sexual status controlling for all the sociodemographic, behavioral, and psychosocial or cognitive variables discussed above. Primary abstainers was the reference group in the multinomial regression models All analyses were conducted separately for males and females using SPSS software, Version 14.028. Results Participants' Characteristics Table 2a, b, c, and d summarize the profiles of the respondents in each of the four sexual status categories for Burkina Faso, Ghana, Malawi, and Uganda respectively. Again, analyses are limited to never-married 15-19 year olds and are presented separately for males and females. On average, primary abstainers were about a year younger than those who had ever been sexually active. Except in Ghana where no substantial gender difference was observed in mean ages, male respondents were on average older than females. Across all four countries, having a boy or girl friend increased the risk of being a secondary abstainer versus primary abstainer, recent abstainer versus secondary abstainer, and currently sexually active versus recent abstainer. In Ghana, for instance, currently sexually active adolescent males and females were 15 times as likely as primary abstainers to report having a boy or girl friend. This relative risk drops with increasing duration since last sex among sexually experienced adolescents. Information on pressure to abstain from sex was not collected for currently sexually active adolescents. Results on this variable (Table 2a, b, c, and d) show substantial variations across countries and between males and females in the same country. With the exception of Ghana where almost equal proportions of males and females reported pressure not to have sex, more females than males, in general, had experienced pressure to abstain from sexual intercourse. The proportion of females reporting pressure to abstain from sex was particularly high in Uganda where over 60% of abstinent respondents stated that they had experienced pressure from others to abstain from sex. Among Burkinabé males, recent abstainers were least likely to report pressure to abstain. In contrast, recent abstainers in Malawi were most likely to do so. For females, pressure was highest among recent abstainers in Uganda while primary abstainers were most likely to report pressure to abstain in Burkina Faso. Among the control variables, ever use of alcohol/drugs was lowest among male and female primary abstainers and highest among recent abstainers or those currently sexually active. However, among Malawian females only 9% of recent abstainers had ever used alcohol/drugs compared to 17% or higher of respondents in the other sexual status categories. For male adolescents, recent abstainers were more likely to report that a teacher, health worker or religious leader spoke to them about sex. This is also true for Burkinabé and Ugandan females while in Ghana, primary abstinent females were most likely to have spoken with someone about sex. Recent abstainers were more likely to be found in urban areas except among females in Uganda. Primary abstainers were more likely to be living with both of their parents. They were also more likely to be currently in school with 70% or more of them enrolled in school in all countries except Burkina Faso where the level of school participation among 15-19 year olds is substantially low. Indeed, currently sexually active adolescents are least likely to be currently enrolled in school followed by recent abstainers. Recent abstainers are more likely to report membership in a club or social group. Most other characteristics do not differ systematically by adolescent sexual status. Multivariate Analyses Multinomial logistic regression models were used to examine the association between the independent variables and sexual status. Due to computational errors in some of the models including religiosity and religion, these variables were dropped from the regression models in all four countries. Eliminating these variables did not have a substantial effect on the retained variables' coefficients. Secondary and recent abstainers were combined into a single group. Table 3a and b summarize the results for males and females, respectively. In each table, we present the final model with controls for all other sociodemo-graphic, behavioral, and psychosocial variables mentioned earlier. Results of the multivariate analyses generally confirm the bivariate results. Among male adolescents, having a girl friend was significantly and positively associated with greater odds of being a secondary or recent abstainer than a primary abstainer in all four countries. It was also associated with increased odds of being currently sexually active than being either a primary, secondary, or recent abstainer. The question on perceived pressure not to have sex was not asked of currently sexually active adolescents and was therefore not included in the multinomial analyses. In a simple logistic regression (not shown) excluding currently sexually active adolescents and including perceived pressure not to engage in sex, the results, which are similar to the multinomial results for secondary or recent abstainers versus primary abstainers, show that perceived pressure not to have sex does not predict sexual status. In Malawi, however, the association was marginally significant and pointed towards those perceiving pressure not to engage in sexual intercourse having lower odds of being primary abstainers versus secondary or recent abstainers. Among the control variables, age and ever use of alcohol were associated with increased odds of being sexually experienced and of being currently sexually active among adolescents who have ever had sex. Being out of school increased the odds of being currently sexually active than being a primary abstainer by a factor of 2 to 4. These effects persisted when primary abstainers were compared to secondary or recent abstainers but the differences were statistically significant only in Ghana and Malawi. Compared to adolescent males who lived with neither of their parents, those who lived with both parents were significantly less likely to be secondary or recent abstainers than primary abstainers. Schools, health care providers, churches and other faith-based organizations are important sources of reproductive and sexual health information for adolescents. Thus, we examined the effect of talking to a teacher, religious leader, or health care provider about sexual matters. Talking to someone about sex had different effects in Ghana and Malawi but had no effect, whatsoever, in Burkina Faso and Uganda. In Malawi, those who had not talked to someone about sex were significantly less likely to be secondary or recent abstainers than primary abstainers. On the other hand, Ghanaian males who had not talked to someone about sex-related matters were 4 times more likely to be sexually active than primary abstinent. The results for adolescent females are similar to those of males. Having a boyfriend is perhaps the most important predictor for sexual activity. A simple logistic regression (not shown) excluding currently sexually active adolescents and including perceived pressure not to engage in sex produced results that were similar to the multinomial results for secondary or recent abstainers versus primary abstainers. Perceived pressure not to engage in sex was not a significant predictor of sexual status except among Burkinabé females with those perceiving pressure not to engage in sexual intercourse being 4.6 times more likely to be primary than secondary or recent abstainers. Among the control variables, being in school strongly predicted sexual abstinence. The odds of being a secondary or recent abstainer or currently sexually active versus a primary abstainer is 2 to 4 times higher among adolescent females who were not in school compared to those in school across the four countries. Compared to females living with neither parent, those living with both parents are less likely to be sexually active than primary abstinent in all countries except Malawi. In Ghana, even the presence of one parent had a strong protective effect on adolescent sexual behavior. Belonging to a social group or club increased the odds of current sexual activity by more than three folds in Uganda but reduced it by two folds in Ghana. In Burkina Faso, Malawi, and Uganda talking to someone reduced the odds of being a secondary or recent abstainer versus primary abstainer. Conversely, in Malawi, talking to someone about sex increased the odds of being a secondary or recent abstainer by a factor of about 2. Knowing someone infected with HIV can heighten one's awareness of their own risk of infection. In Ghana and Malawi, females who reported that they knew someone who was either living with HIV/AIDS or who had died from the disease were about 2 times more likely to be secondary abstainers than primary abstainers. Except in Uganda, where increasing HIV/AIDS knowledge was associated with greater odds of being sexually experienced, HIV/AIDS knowledge was not a significant predictor of sexual status. Reasons for abstinence All sexually inexperienced respondents and sexually experienced respondents who did not report sexual activity in the 3 months preceding the survey were asked to state the main reason why they were abstinent. Reasons given for not having intercourse included, among others: the lack of a partner, postponement of sex until marriage, fear of pregnancy, avoiding STIs, and young age. Table 4 summarizes the respondents' main reasons for not engaging in sexual intercourse by sexual status and gender. Close to 70% of Malawian and Ugandan males stated that their main reason for not engaging in sexual intercourse was to avoid STIs and HIV and this did not differ much by sexual status. Among Burkinabé and Ghanaian males, this proportion was much lower at 13% and 20% respectively, with secondary abstainers being about twice as likely as primary abstainers to give this reason. Twenty four percent of secondary abstainers from Burkina Faso reported that they were abstaining from sexual intercourse because they lacked a partner. In all countries, except Malawi, female adolescents were about 2 times more likely than males to report a desire to wait until marriage before being sexually active. Burkinabé, Malawian, and Ugandan females were also 4 times more likely than their male counterparts to report fear of pregnancy as a key reason for being abstinent. Across all countries and for both males and females, primary abstainers were more likely to report a desire to wait for marriage than secondary and recent abstainers except in Uganda where similar proportions of abstinent males reported this reason. Nearly a quarter of primary abstinent Burkinabé males reported that they were too young as their main reason for being sexually abstinent. Discussion Choosing to be sexually abstinent may be one of the major challenges facing young people given the widespread exposure to sexually explicit material9 that to some extent "glorifies" risky sexual behavior, including multiple sexual partnerships. Further, the erosion of traditional value systems that dictate acceptable sexual conduct among young people imply that adolescents have to deal with contradictory values and fewer guidelines regarding sexuality3. Concerns about adolescent sexual health, especially in the face of the HIV/AIDS pandemic, have led to a proliferation of studies examining the correlates of sexual activity; yet, there is a relative paucity of studies that assess the characteristics of young people who chose to abstain from sexual intercourse. Thus, in this study we examined differences across never-married primary, secondary, and recent abstainers as well as sexually active adolescents aged 15-19 years in four sub-Sahara African countries. We noted a difference in the proportion of abstinent adolescents who had never had sexual intercourse across the four countries. Whereas over 67% of Burkinabé and 85% of Ghanaian male respondents aged 15-19 years reported no prior sexual activity, only 42 % of Malawian and 53% of Ugandan respondents in the same age group had never had sexual intercourse. Findings from focus group discussions conducted as part of the larger study show that the sentiment that abstinence is an ideal that is difficult to achieve was more often mentioned by Malawian and Ugandan males. Further, more Malawian and Ugandan than Burkinabé or Ghanaian respondents viewed abstinence as a practice adopted once someone had been tested for HIV. Conversely, Burkinabé and Ghanaian focus group participants endorsed abstinence until marriage more than those in Malawi and Uganda29. The results of our study corroborate the focus group discussion findings. These cross-country disparities may reflect differences in socio-cultural practices regarding sexuality. For example, among the Lomwe in Malawi young males who have undergone initiation rites are encouraged by their peers to have sex in order to gain adult status through a practice termed kuchotsa fumbi (removing the dust)30, 31. The likelihood of reporting sexual activity increases with increasing age20, 21. Not surprisingly, therefore, adolescents who had never had sexual intercourse were significantly younger than abstinent respondents reporting prior sexual activity. Similarly, Paradise and colleagues32, in a survey of young female adolescents in the United States, found that primary abstainers were significantly younger than sexually active adolescents. The association between age and primary abstinence, has led to arguments for abstinence-based interventions among prepubertal girls and boys whose sexual identity is still in the formative stages33. More than 60% of Malawian and Ugandan males stated that they were abstinent mainly to avoid STIs/AIDS. On the other hand, only 20% of Ghanaian and 13% of Burkinabé males endorsed the same reason. Country-specific HIV/AIDS prevalence rates may explain this difference. At the end of 2005, Uganda had an adult HIV/AIDS prevalence rate of approxi-mately 6.7%15, down from an estimated prevalence of approximately 20% in the early 1990s2. Malawi, on the other hand, had an adult prevalence rate of 14.1% at the end of 2005. In contrast, Ghana and Burkina Faso had relatively low prevalence rates of 2.3% and 2.0% respectively, at the end of 200515. Cross country disparities in HIV prevalence rates may also be reflected in the observed differences in the proportions of adolescents reporting knowledge of someone living with or who has died from HIV/AIDS. Consequently, for youth in Malawi and Uganda, the risks of acquiring HIV through sexual intercourse may be more salient. In addition, since ABC campaigns are often implemented in the context of HIV and AIDS prevention, a consequence of such a program emphasis may be increased knowledge of HIV and AIDS and consequently, an increased role of the fear of HIV and AIDS as a factor in sexual abstinence. One would expect the role of such a factor to be more pronounced in countries such as Uganda, where such programs are common11 and where HIV prevalence has historically been high. The data supported expected male-female differences in motivations to be abstinent. In general, more females endorsed fear of pregnancy or waiting until marriage as key motivators to delay sexual involvement. This is consistent with previous research examining gendered differences in adolescent sexuality13. Differences in socializa-tion may partly explain the differences between males and females. For example, sexuality among females may be more closely associated with marriage and procreation34. Further, the greater percentage of females choosing sexual abstinence for fear of pregnancy may also reflect the more severe repercussions of teenage pregnancy borne by females. In general, a greater proportion of primary abstainers than sexually experienced adolescents endorsed waiting for marriage as a principal reason for abstinence. Greater endorsement of more value-based reasons for abstinence, such as waiting for marriage, among virgins compared to sexually experienced, but currently abstinent youth have been observed in several studies13, 32. As such, reinforcing sexual abstinence among adolescents who have never had sexual intercourse may take a more value-based approach. However, for adolescents who have had sexual intercourse, emphasis on abstinence as a protective strategy against the adverse consequences of sexual activity, such as pregnancy or sexually transmitted infections, may be more relevant. Young people enrolled in school may be less likely to engage in risky sexual behavior than out-of-school youth4, 26. Except in Burkina Faso where less than 25% of both male and female respondents were enrolled in school, more primary abstainers than sexually experienced respondents were students. Further, when controlling for other covariates, females who were not currently enrolled in school were significantly more likely than those in school to be sexually experienced. The protective effect of being in school may partially explain why Burkinabé females aged 15-19 years were about 2 times more likely to be currently sexually active than similarly aged Ghanaian, Malawian, and Ugandan females. Educating women has been identified as an important tool for ensuring women's health and studies show that women who are educated are more likely to be aware of HIV preventive actions, to delay sexual intercourse, as well as to adopt other preventive measures35. Alcohol consumption and drug use were important predictors of sexual status, particularly among males, with primary abstainers being the least likely to report ever using drugs and/or alcohol. The co-occurrence of sexual activity and substance use has been reported in several studies36-39. Thus, reproductive and sexual health programs targeting adolescents may benefit from including educational components on other risk behavior, such as drug and alcohol abuse. For both males and females, being in a romantic relationship was associated with a greater likelihood of being a sexually experienced abstainer or being sexually active than being a primary abstainer. Recent abstainers may, therefore, not have engaged in sexual intercourse for relationship-specific reasons, such as partner absence, rather than as a result of a conscious decision to avoid sexual intercourse. This has important implications for abstinence promotion interventions targeted towards those currently involved in romantic relationships because these adolescents may be facing greater pressure to engage in sexual intercourse. As such, this group may benefit from educational programs that provide adolescents with the necessary communication and refusal skills. Given the limited use of condoms among adolescents2, 3, 30, condom use promotion may be another strategy to prevent pregnancy and STIs, including HIV among adolescents involved in romantic relationships who may still be inexperienced sexually. As stated previously, abstinence in the ABC approach focuses on unmarried adolescents, urging them to wait until marriage before engaging in sexual intercourse12 and many organizations with funding from PEPFAR advance this position11. We suggested earlier that if messages advocating abstinence have an impact, many adolescents would reflect this impact as pressure from family members, relatives, and others to abstain from sex and that those experiencing greater pressure to abstain would actually be abstinent. Further, tradition in many parts of Africa dictates that young people should avoid premarital sex and childbearing, which bring dishonor to the family40. Görgen and colleagues41, for example, found that schoolgirls in a small town in Burkina Faso who had premarital pregnancies reported that the pregnancies had created a rift between them and their families. Moral norms prohibiting premarital sexual relationships may explain why the greatest proportion of Burkinabé adolescents reporting pressure from others not to have sexual intercourse was among those who have never had sex. We, however, also acknowledge that adolescents who are perceived to be sexually active may receive more attention and pressure to abstain, particularly in contexts where the risks of STIs and other negative sequelae are more pronounced, such as in areas of high HIV prevalence. For example, in Uganda, which has historically had a high HIV prevalence and where there has been strong political support of the fight against HIV42, pressure to abstain from sex was reported by close to 50% of males and over 60% of females, irrespective of sexual status. Indeed, among Ugandan females, recent abstainers are most likely to report such pressure with nearly three quarters reporting pressure to abstain compared to less than two thirds of primary abstainers. In all countries, with the exception of Ghana, a greater proportion of females than males reported pressure not to engage in sexual intercourse. In much of Africa, men are socialized to have control over sexuality and reproduction43 and it is widely accepted that men have a higher biological need for sexual intimacy44, 45. In a context characterized by such double standards in sexual-cultural norms for males and females, it is not surprising that a greater proportion of females than males would report pressure not to have sexual intercourse. Limitations This study was exploratory and has several limitations. First, the study utilized cross-sectional data; therefore, causality cannot be inferred. The effect of sociodemographic, behavioral, and psychosocial or cognitive characteristics on the delay of sexual activity can be determined through a longitudinal study design. Second, because of the sensitivity of the information sought, participants may have provided socially-desirable responses despite measures taken during data collection to ensure privacy and confidentiality of the information shared by respondents. Third, analyses were restricted to older adolescents. Accordingly, findings may not be generalizeable to younger adolescents for whom the decision to be abstinent may be driven more by moral beliefs46 than by societal and contextual factors that play an increasingly important role in decision making in adulthood47. Lastly, capturing the main reasons why adolescents chose to be abstinent was restricted by the available response options provided in the survey. Other reasons that may be important, but were not provided as responses for the main reasons for abstinence in the Ghanaian, Malawian, and Ugandan surveys include: waiting until one is older, religious beliefs about having sex outside of marriage, or fear of parents' reactions to sexual activity. Conclusions Motivations to be sexually abstinent may be driven by a wide variety of factors ranging from value or moral-based reasons, such as waiting for marriage, to avoidance of negative consequences such as sexually transmitted infections and pregnancy. The effectiveness of abstinence promotion interventions may be heightened by incorporating messages that take into account both the various reasons adolescents give for not engaging in sexual intercourse13 and the demo-graphic, behavioral, and psychosocial characteristics of young people. Gender, contextual circumstances and prior sexual experience may also influence current sexual behavior and should be considered when designing abstinence promotion programs. Acknowledgements This research uses data from Protecting the Next Generation: Understanding HIV Risk Among Youth, a project designed by The Guttmacher Institute (United States) in collaboration with the University of Cape Coast (Ghana), Institut Supérieur des Sciences de la Population (Burkina Faso), Makerere Institute of Social Research (Uganda), Centre for Social Research (Malawi) and the African Population and Health Research Center (Kenya). Funding for this project was provided by The Bill & Melinda Gates Foundation, the Rockefeller Foundation and the National Institute of Child Health and Human Development (Grant 5 R24 HD043610). Footnotes FNA Participants aged 12-14 years were asked whether they had ever heard of sexual intercourse. Those who responded "no" or "don't know" were skipped on questions on sexual behavior and classified here as primary abstainers. About 15-25% of 12-14 year olds in the four countries reported that they had never heard of sexual intercourse.
References
© Copyright 2007 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh07038t2d.jpg] [rh07038t2a.jpg] [rh07038t3b.jpg] [rh07038t4.jpg] [rh07038t2b.jpg] [rh07038t1.jpg] [rh07038t3a.jpg] [rh07038t2c.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}