 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 11, No. 3, December, 2007, pp.197-220 Knowledge of correct condom use and consistency of use among adolescents in four countries in Sub-Saharan Africa Connaissance du bon mode d'emploi du préservatif et la consistence de son emploi chez les adolescents dans quatre pays d'Afrique subsaharienne Akinrinola Bankole1, Fatima H. Ahmed1, Stella Neema2, Christine Ouedraogo3,and Sidon Konyani4
1Akinrinola Bankole, The Guttmacher Institute 1Fatima
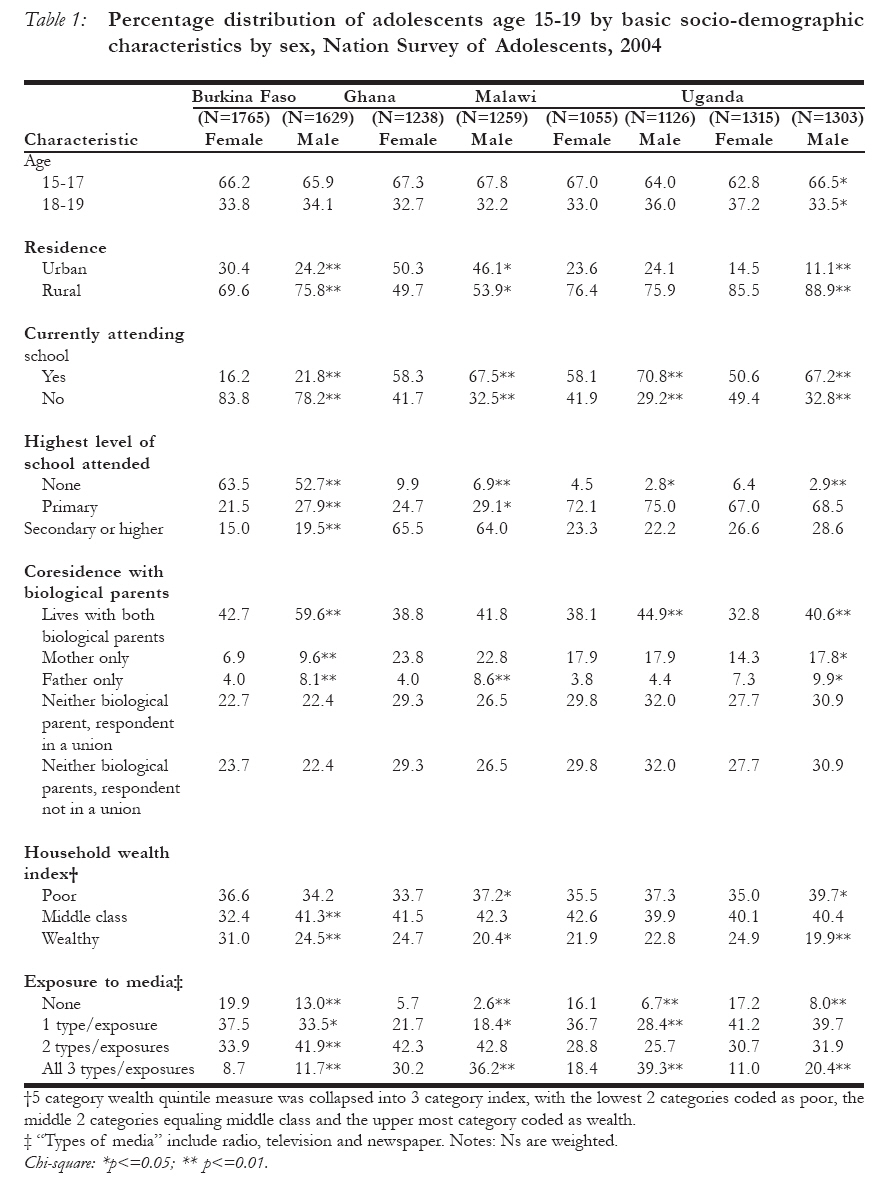
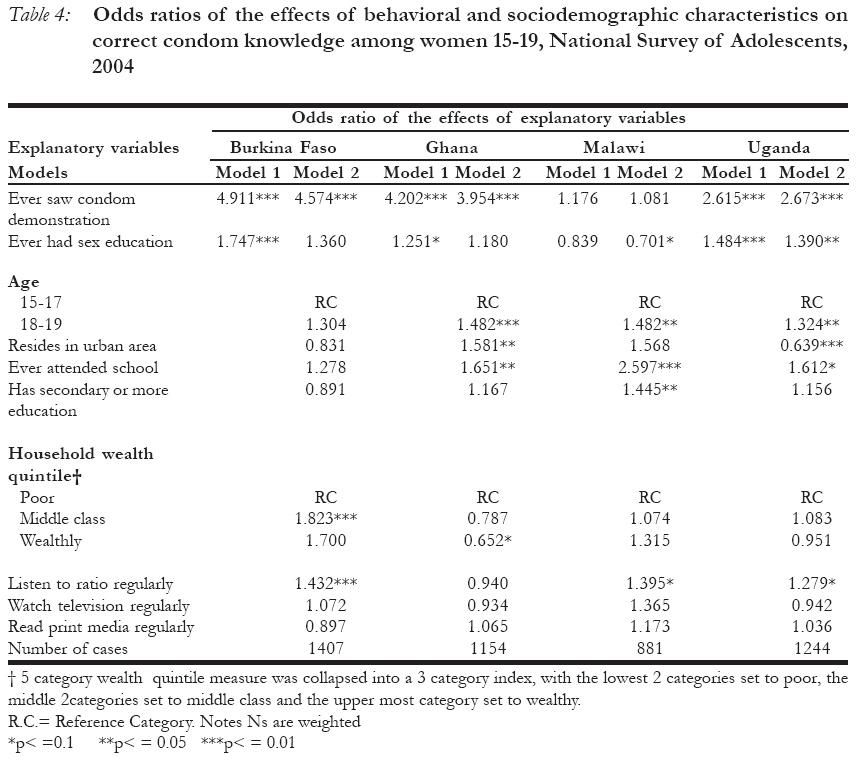
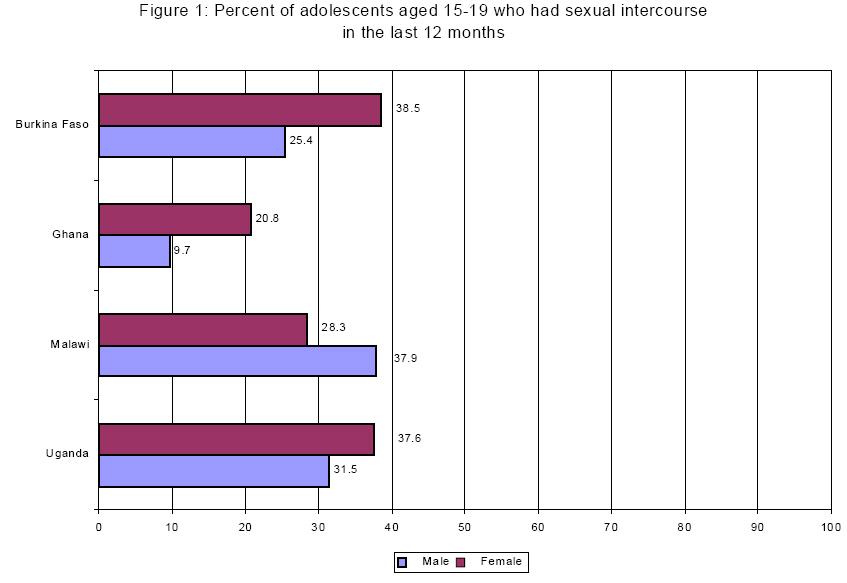
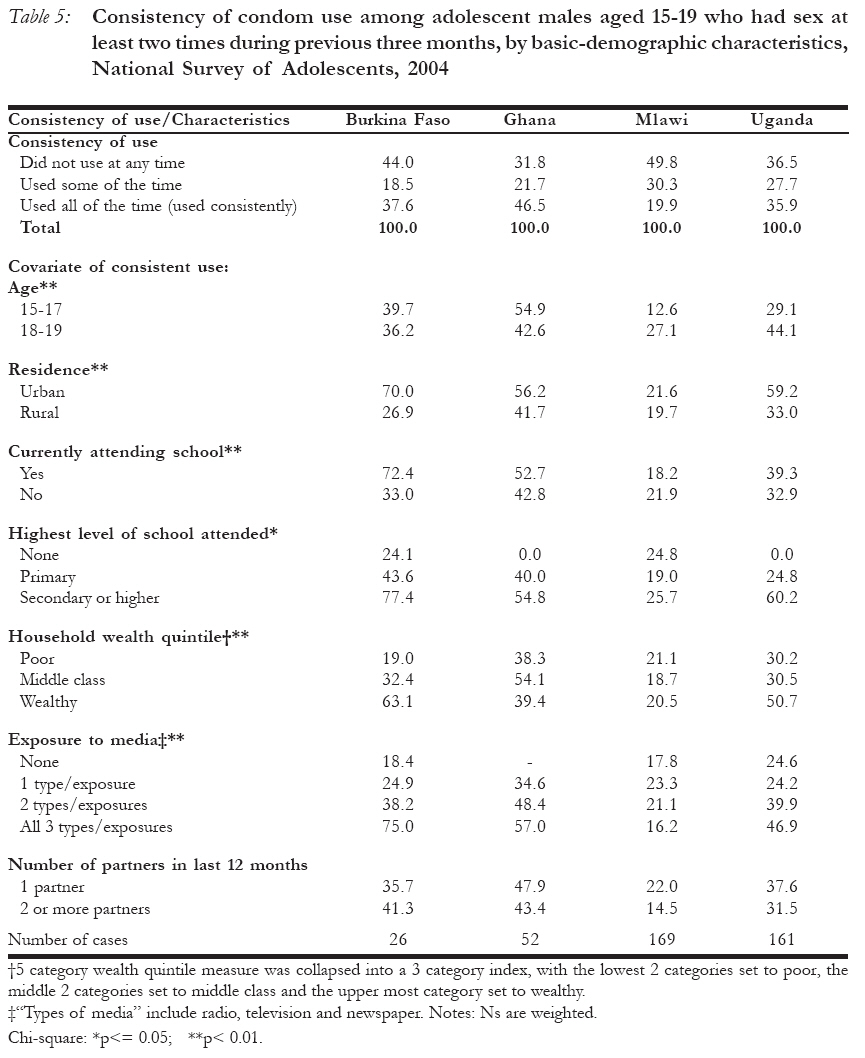
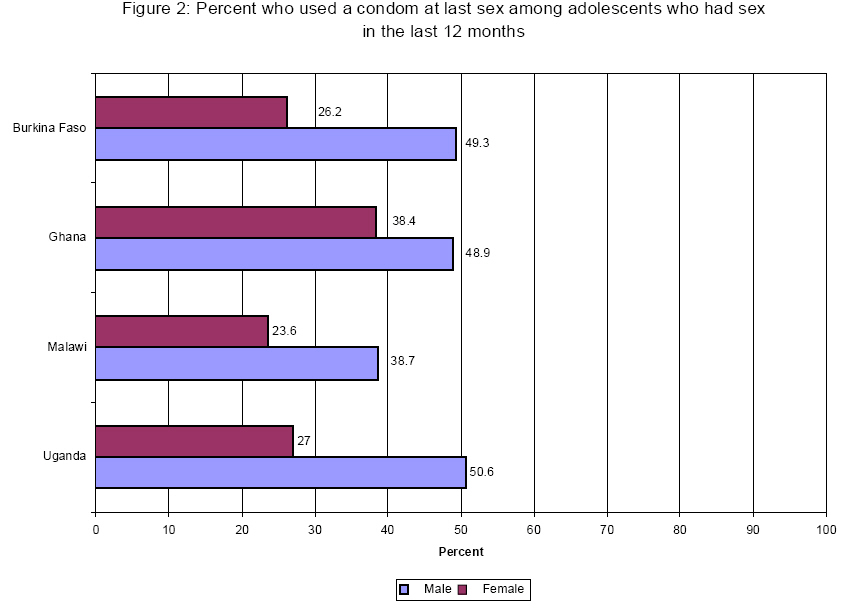
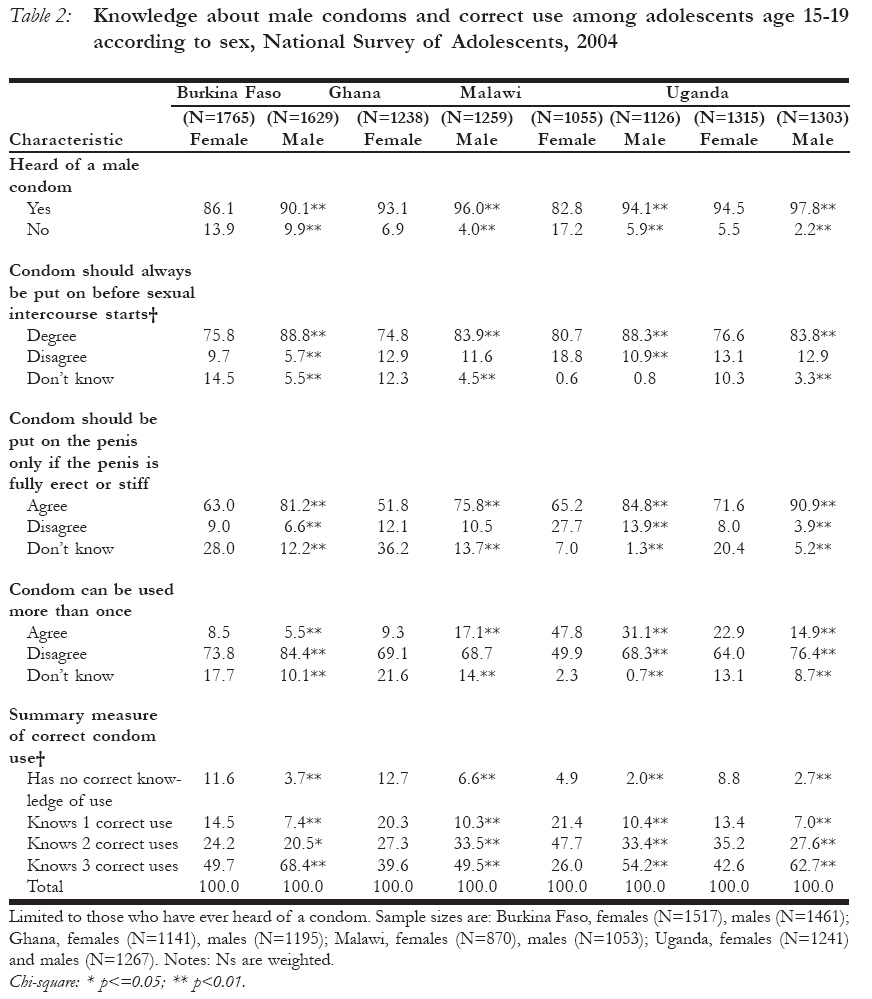
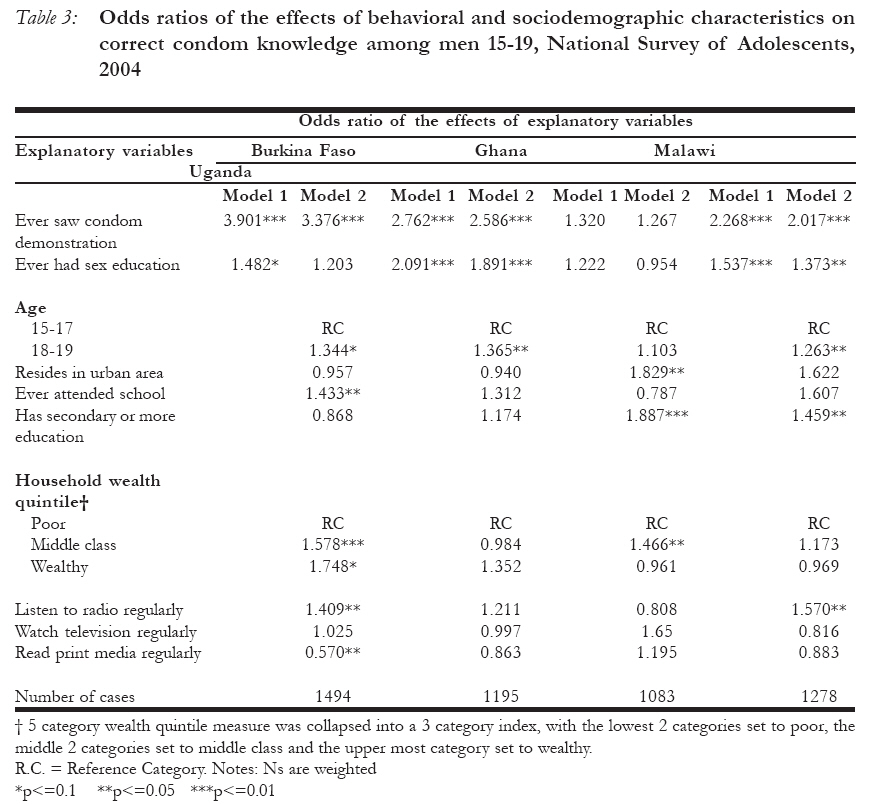
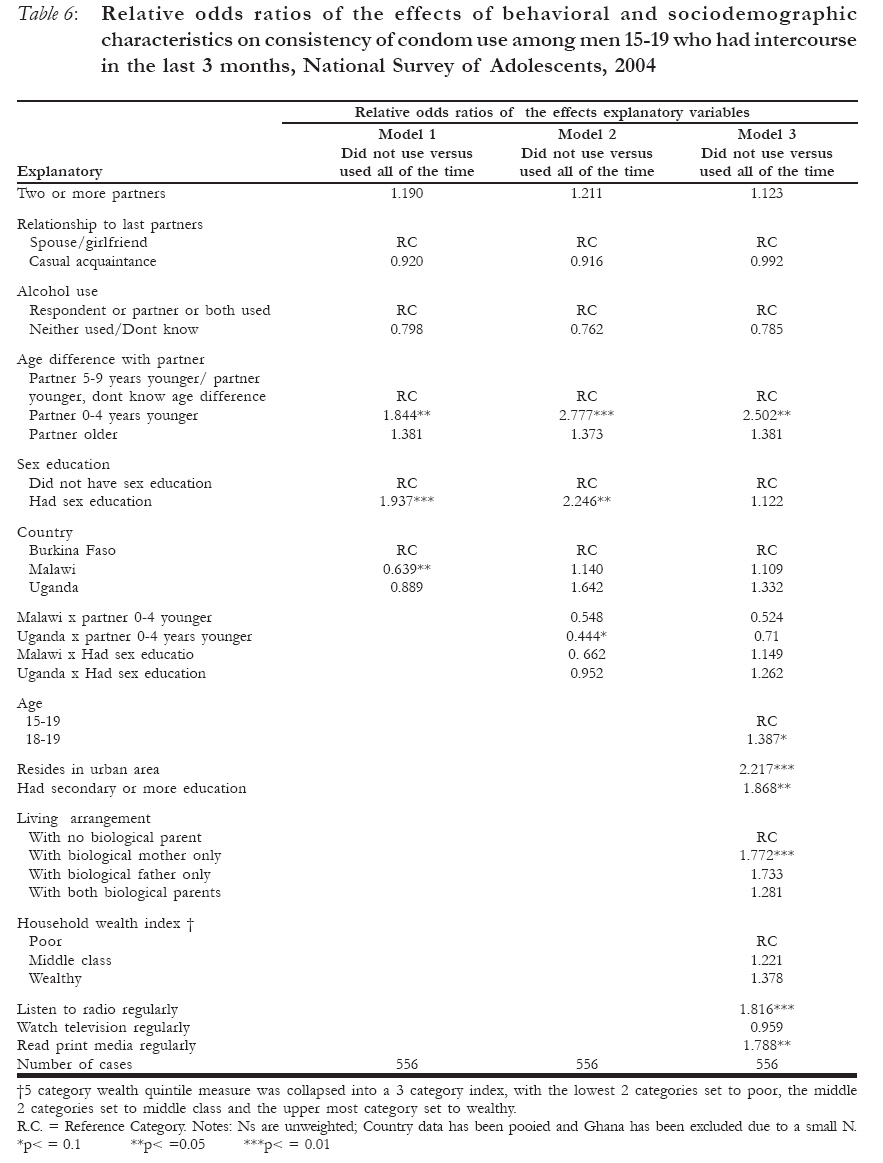
H. Ahmed, The Guttmacher Institute Code Number: rh07043 Abstract Using data from the 2004 National Adolescent Surveys, this paper undertook a detail analysis of knowledge of correct condom use and consistency of use, as well as their covariates, among adolescents in Burkina Faso, Ghana, Malawi and Uganda. The strongest predictor of knowledge of correct condom use among both male and female adolescents is exposure to a condom use demonstration. In Burkina Faso, Ghana and Uganda, adolescents who have seen a condom demonstration are 2 to 5 times as likely as those who have not to have good knowledge of correct condom use. Age, ever received sex education in school, ever attended school and exposure to the radio are also significant predictors of knowledge of correct use, particularly among men. As indicated by behavior among young men, the extent to which adolescents use the condom consistently varies across countries. Yet, it is nowhere near the required 100% level. The proportion reporting consistent use of the method in the 3 months preceding the survey is 38% in Burkina Faso, 47% in Ghana, 20% in Malawi and 36% in Uganda. Age difference between partners is a major determinant of consistent use of condoms: young men whose partner is 0-4 years younger are about two and a half times more likely to use condoms consistently than those who whose partner is 5-9 years younger. Other important predictors of consistent condom use are residence, education, living arrangement and exposure to mass media, specifically the radio and newspaper. Findings from this study point to areas that policy and program can address to provide adolescents access to the kinds of information and service they need to achieve healthy sexual and reproductive lives. Key Words: corret condom use, sex education, adolescents Résumé A l'aide des données recueillies des Enquêtes Nationales sur les Adolescents en 2004, cet article fait une analyse détaillée de la connaissance du bon mode d'emploi du préservatif et la consistence de son emploi aussi bien que ses co-variables, chez les adolescents au Burkina-Faso, au Ghana, au Malawi et en Ouganda. L'indice le plus fort de la connaissance du bon mode d'emploi du préservatif chez les adolescents et les adolescentes est de les exposer à une démonstration de l'emploi du préservatif. Au Burkina-Faso, au Ghana et en Ouganda les adolescents qui ont vu une démonstration du préservatif ont 2 à 5 fois plus la possibilité d'avoir une bonne connaissance que ceux qui n'ont pas vu la démonstration. L'âge, avoir jamais reçu les cours sur l'éducation sexuelle à l'école, avoir jamais fréquenté une école et l'exposition à la radio, constituent aussi des indices importants de la connaissance du bon mode d'emploi, surtout chez les hommes. Comme l'a indiqué le comportement chez les jeunes hommes, le point jusqu'à quel les adolescents utilisent constamment le préservatif varie de pays en pays. Pourtant, cela n'est pas proche du niveau de 100% requis. La proportion qui a signalé avoir constamment utilisé la méthode au cours des trois mois précédant l'enquête est 38% au Burkina-Faso, 47% au Ghana, 20% au Malawi et 36% en Ouganda. La disparité d'âge entre les partenaires est un déterminant important de l'usage constant des préservatifs. Les jeunes hommes dont les partenaires étaient plus jeunes de 0-4 ans ont environ deux fois et demi la possibilité d'utiliser constamment le préservatif que ceux dont les partenaires sont moins âgées de 5-9 ans. Autres indices importants de l'usage constant des préservatifs sont la résidence, l'instruction, la manière de se loger et l'exposition aux médias, en particulier la radio et le journal. Les résultats de cette étude signalent les domaines dont la politique et le programme doivent s'occuper pour fournir aux adolescents l'accès aux genres de renseignements et de services dont ils ont besoin pour accomplir la vie sexuelle et de reproduction saine. Key Words: corret condom use, sex education, adolescents Introduction HIV and AIDS are increasingly affecting youth worldwide, and Sub-Saharan Africa is the hardest hit with females having higher rates than males. In many parts of the world, new HIV infections are heavily concentrated among young people between 15 _ 24 years of age. Among adults 15 years and older, young people accounted for 40% of new HIV infections in 2006.1 Nevertheless, there are significant variations in the prevalence of HIV among the countries in the region. In 2005 the prevalence among young people aged 15-24 was estimated to be 4.3% for women and 1.5% for men.1(Annex 2) Among the four countries on which this paper focuses, the HIV prevalence rates in 2005 among people 15-24 years old ranged from 0.8 to 2.0 for women and 0.3 to 0.6 for men in Burkina Faso, 1.1 to 1.5 for women and 0.2 to 0.3 for men in Ghana, 3.9 to 16.8 for women and 1.4 to 5.9 for men in Malawi and 4.2 to 5.7 for women and 1.9 to 2.6 for men in Uganda.1(Annex 2) Unless young people adopt protective behaviors this trend may continue in the absence of a HIV and AIDS cure. Unintended pregnancy is also a major reproductive health problem among young people in Sub-Saharan Africa. Although birth rates are high in most of the countries in the region, substantial proportions of women and couples are becoming pregnant and having children when they want to limit childbearing or delay the birth of another child. Most sexually active adolescent women and men do not want to have children because they are in school, too young or not married, and therefore are prone to the risk of unintended pregnancy, unless they are using an effective method. For example, it has been estimated that, on average, there are about 8 years between the age at which men in the region initiate sexual activity and the age at which they have their first child.2 In the early 2000s, the proportions of recent births to adolescent women that were either mistimed or unwanted were 23% in Burkina Faso, 40% in Ghana, 40% in Malawi and 39% in Uganda.3 Improvements in the opportunity costs of having children (e.g. better education, non-agricultural employment etc) is likely to further motivate young people to postpone marriage and childbearing.4 However, despite these advances in opportunities for young people without adequate information and improved access to contraceptive services, young women in these countries will continue to experience unwanted pregnancy, and probably at higher rates. It is clear that both risks of HIV and unwanted pregnancy are real among adolescents in Sub-Saharan Africa. For young people who are sexually active, besides sex with one uninfected partner, the condom, is the only method that offers protection against HIV and some other STIs.5;6 Additionally, it has been shown that the condom is an effective method of preventing unwanted pregnancy, and it is certainly the most preferred method among unmarried young people.7 However, there is a caveat. A review of literature on condom promotion and use for HIV prevention in developing countries, found that only consistent use of the condom offers effective protection against HIV.8 The report noted that the effect of condoms may be mitigated by inconsistent use, low use among those at highest risk, and negative interactions with other strategies. Ttherefore, it recommended, among other things, the need to measure the rates of consistent condom use by type of partners. To date, very few studies have attempted to examine correct and consistent use of the method among sexually active people. Despite extensive efforts in promoting condom use, young people in Sub-Saharan Africa still engage in risky sexual behaviors and condom use remains relatively low. A multitude of factors may impede young people's ability to protect themselves by using condoms, including attitudes towards condoms and ineffective use of the method. Numerous studies have found that young people's perceptions of condoms tend to be negative.9;10 Studies have also documented that young people have concerns about condom safety and breakage, condom ineffectiveness (e.g., condoms have small holes or they can disappear into the vagina)13;14, the negative effect of condom use on sexual enjoyment11;15;16, the low quality of condoms16—especially condoms that are free14;17, and condom use signifying infidelity or having an STI.10;11 In a number of studies, trust in a sex partner was mentioned as a reason for not using condoms.16;18-20 Although a number of studies have looked at young people's perceptions of condoms, there is little data on the extent to which perceptions about condoms may mitigate condom use. Tackling misperceptions remains a challenge for programs and policies aimed at increasing condom use among sexually-active adolescents, and while the evidence continues to grow about how adolescents view condoms, very little information is available on whether adolescents' knowledge of how to use condoms is correct and whether they actually use condoms correctly and consistently. The evidence that condom use is increasing among young people in many Sub-Saharan countries is certainly encouraging, however, it has been argued that increasing condom use will not be fully effective in stemming HIV and STI transmission or preventing unwanted pregnancy if condoms are used inconsistently or incorrectly. Given the high vulnerability of young people to HIV and the risks of unintended pregnancy, it is of program and policy relevance to better understand condom use behavior and the barriers to effective use of the method among sexually-active adolescents in order to help young people lead healthy sexual and reproductive lives. This paper addresses gaps in understanding the dynamics of condom use among 15-19 year old adolescents using recently collected information from adolescent men and women. The surveys from which the data derive included questions on sexual activity and condom use that are rarely collected in national surveys, including the Demographic and Health Surveys (DHS). The paper presents new evidence on adolescent men's and women's level of knowledge about correct use of condoms and young men's experience with condom use consistency and the factors associated with both of them. Source of data and method of analysis Data source Data for this paper come from the 2004 National Survey of Adolescents carried out among 12-19 year old females and males in Burkina Faso, Ghana, Malawi and Uganda. The nationally-representative household surveys are part of an on going study titled "Protecting the Next Generation: Understanding the Sexual and Reproductive Health Needs of Young People", which is being undertaken by the Guttmacher Institute, in collaboration with Institut Superieur des Science de la Population in Burkina Faso, University of Cape Coast in Ghana, University of Malawi's Center for Social Research, Makerere Institute of Social Research in Uganda and African Population and Health Research Center in Kenya. The surveys were conducted on behalf of the project collaborators by Macro International Inc., in collaboration with its in-country partners. All four surveys were fielded between September 2003 and June 2004, beginning with Ghana. The samples for the surveys covered the population residing in private households in the country. A two-stage stratified sample design was used. First was household selection: 5,400; 9,445; 7,750; 7,106 households were selected and 5,162; 8037; 6,029; 6,182 were interviewed in Burkina Faso, Ghana, Malawi and Uganda, respectively. The response rates for households were 100% for Burkina Faso, 98% for Ghana, 99% for Malawi and 98% for Uganda. Second was the respondent selection: 6,268; 4,840; 4,506; 5,807 eligible adolescents, respectively, were identified and 5,986 were interviewed in Burkina Faso, 4,433 in Ghana, 4,042 in Malawi and 5,127 in Uganda. The corresponding response rates were 96% for Burkina Faso, 92% for Ghana, 90% for Malawi and 88%for Uganda. The overall response rates (household response rate x eligible adolescent response rate/100) for each country were: 95% for Burkina Faso; 89% for Ghana; 89% for Malawi; and 87% for Uganda. The adolescent questionnaire collected information about a wide range of aspects of adolescents' lives. The survey questionnaire is comprised of the following sections: respondent's background characteristics, family and social group contact information, reproductive experiences, pregnancy knowledge and sex education, contraceptive method knowledge, use and information and service sources, marriage/union formation and sexual activity (12-14 year olds were asked questions about other kinds of sexual activities in addition to sexual intercourse), sexual relationship history, HIV and AIDS knowledge, information sources and voluntary counseling and testing knowledge and experiences, sexually-transmitted infections (STI) knowledge, experiences of, and information and service sources, socio-cultural practices (includes experiences and timing of initiation rites, circumcision, recent experiences with injections, communication with family and others about sex-related matters and attitudes about sexual activity), worries about different types of risk that young people face, including HIV and AIDS, substance use and childhood background, physical and sexual abuse and anal sex (questions were asked only of one, randomly-chosen, eligible adolescent per household). Further detailed information about the survey samples and methodology is publicly available.21-24 This paper is based on the information collected from 15-19 year old women and men. The decision to restrict the analysis to women and men of this age group is based on the fact that much of the information relevant to the main subject of the paper were not obtained from the 12-14 year old adolescents since most of them were yet to initiate sexual intercourse. Method of analysis The measures of sexual activity reported in this paper are derived from standard DHS type questions, including whether or not the respondent has had intercourse and duration since the last. Based on responses to these questions, we summarized results for ever had sex, sex in the last 12 months and sex in the last 3 months. Measures of condom use were also constructed from DHS-type questions on ever use of condoms and use of the method at last intercourse. We also briefly summarized the findings to set the stage for the main focus of the paper. Young men's and women's knowledge about correct use of condoms was examined by analyzing responses to statements aimed at measuring this knowledge. Five questions were asked about correctness of condom use based on items from Indiana University's Kinsey Institute for Research in Sex, Gender and Reproduction's Condom Use Errors Survey for Adolescent Males (August 26, 2001 version) Out of the five statements included in the survey on this issue, we analyzed three that we believe more clearly depict knowledge of correct use. These are: "Condom should always be put on before sexual intercourse starts"; "condom should be put on the penis only if the penis is fully erect or stiff"; and "condom can be used more than once". The respondent was expected to give one of the following responses: "agree", "disagree" or "don't know". Based on responses to the three statements, we constructed a four-category measure of correct knowledge of condom use by counting the number of times out of three that a respondent gave a correct answer to the statements. Those who correctly responded to all three statements were given the value of 3, those who did so for two or one of the state-ments received a value of 2 or 1, respectively and those who were unable to correctly respond to any of them was assigned a value of 0. We analyzed this summary measure as well as responses to the individual statements. Factors associated with correct knowledge of condom use were examined using the summary measure. Male respondents aged 15-19 were asked questions about their sexual activities in the last 3 months, including whether or not a condom was used at every intercourse in the 3 month period. We obtained the measure of consistency of condom use from this information. This involved obtaining a count of the number of sexual episodes a man had in the three month period and for each episode determining whether or not a condom was used. Specifically, among all adolescent men who reported having 2 or more sexual acts in the 3 months prior to the interview, we constructed a measure of consistency of condom use with 3 categories, namely, used all of the time, used some of the time and never used. With this categorization, each young man who had sex more than once in the 3 month period was classified as a "consistent user", an "occasional user" or a "never a user". By this definition the extent of consistent use of the condom among sexually active men with 2 or more sexual acts is the proportion of all men who were "consistent user". This analysis was limited to those who had at least 2 sexual episodes because at least two experiences are required to determine consistency. Two multivariate analyses were undertaken. The first was an analysis of the association between behavioral and sociodemographic characteristics and knowledge of correct condom use among women and men aged 15-19. The dependent variable was the summary measure of knowledge of correct condom use described above. It is a four-category ordinal variable with a value of 0 if the respondent correctly responded to none of three statements, 1 if she/he responded correctly to only one statement, 2 if she/he correctly responded to two statements or 3 if she/he correctly responded to all three statements. The explanatory variables included in the models for both sexes were exposure to condom demonstration and exposure to sex education in school. These two were assumed to be immediate determinants of knowledge of correct use. They are considered to be key factors in this analysis because of their program and policy relevance, and because they have been found in some other work to be important determinants of condom use.25 Exposure to condom demonstration was measured via responses to the following question: "Have you ever seen a male condom demon-stration? By a condom demonstration, I mean someone like a nurse, other adult, or peer showing people how a male condom is correctly used." Similarly, the measure of exposure to sex education in school derived from responses to the question: "Some schools have classes on family life education. Have any of your schools offered any classes or talks on family life education?" Respondents who answered "yes" to this question were then asked: "Did you ever attend any classes or talks on family life education?" While one may suppose that these two variables will be highly correlated, it is not so in this case. For example, in Ghana, where exposure to sex education is highest among our study countries, about half of adolescents aged 15-19 received sex education in school (data not shown). Of the one-half, 57% had seen condom use demonstration, while 39% of the remaining half who did not receive sex education in school had also seen condom use demonstration. Also included in the models are selected background characteristics that may directly or indirectly be associated with correct condom use knowledge, namely age, rural-urban residence, education, living arrangement, household wealth status, and exposure to mass media sources - radio, television and print media. Since the dependent variable is ordinal, ordered logistic regression models were preferred. This analysis was done for each country and two models were estimated for each sex. The first examined the relationship between the intermediate variables, exposure to condom demonstration and exposure to sex education in school, without controlling for any other variable. The second model included these two variables as well as the selected characteristic variables. This model allowed us to determine whether or not the associations found between knowledge of correct condom use and the two intermediate variables hold when the effects of the background variables are accounted for and to identify the background variables that are significantly related to knowledge of correct condom use. The second multivariate analysis was an examination of the relationship between behavioral and sociodemographic characteristics and consistency of condom use among adolescent men aged 15-19 who had two or more sexual acts in the 3 months preceding the survey. The dependent variable is the measure of consistency of use described above. It is an ordinal variable with a value of 0 if none of the sexual episodes a respondent had in the 3 months period was protected with condom use, 1 if some but not all of the sexual encounters were protected with condoms and 2 if all of the sexual episodes were protected with condoms. Two groups of explanatory variables were included in the analysis. The first is a set of behavioral and more proximate variables, namely, number of partners, relationship with the last sexual partner, alcohol use, age difference between partners and exposure to sex education. The first three of these variables are included because they are often considered as measures of risky behavior and those who engage in these behaviors have been found to be less likely to use condoms.26 Similarly, wider age difference between partners has been associated with lower condom use.27 Women who have sex with men who are older than them may lack the confidence to demand that their partners use the condom. The second set included the same selected background characteristic variables used in the model for knowledge of correct condom use. Because the sample of young men aged 15-19 with more than one sexual act is small for each country to allow separate analysis by country, this analysis used pooled data for three of the four countries, each of which contributed more than 150 observations to the analysis. Ghana was excluded because only 50 young men aged 15-19 had more than two sexual acts in the last 3 months. To account for possible differences among countries, we included a country variable in the analysis. Since the dependent variable is ordinal, we used ordered logistic regression models. Three models were estimated. Model 1 included only the five behavioral proximate explanatory variables and the country variable. Given that the country variable was significant at less than a 5% level in Model 1, Model 2 includes all variables in Model 1 plus the interaction terms between the behavioral variables that are significant in Model 1 and the country variable. Model 3 included the variables in Model 2 plus the background characteristic variables. Since the country variable was not significant in Model 3 we did not include interaction terms between it and the significant characteristic variables. All estimates shown in this paper, with the exception of the regression analysis of consistency of condom use (based on pooled data), are weighted national estimates. For proportions and coefficients from the regression analyses using weighted data, the standard errors of all estimates were computed in Stata taking into account the complex sampling techniques used in conducting the adolescents surveys. Significance tests were also undertaken for the results to ascertain the statistical significance of the difference in proportions as well as the effects of covariates. Significance is indicated at the 0.01 and 0.05 and using two-tailed tests. Results Characteristics of respondents About two-thirds of the women aged 15-19 were between the ages of 15-17 in all four countries (Table 1, Columns 1-4). With the exception of Ghana, where half of young women lived in urban areas, most of the respondents were rural residents: 70% in Burkina Faso, 76% in Malawi and 86% in Uganda. Roughly one half of the young women were currently in school in three of the countries. Burkina Faso, the country not in this group, had a much lower proportion of young women (16%) in school. Again, in terms of educational attainment, Burkina Faso stands out as the only country where the vast majority (64%) of young women had never attended school. This proportion is 10% or less in the other three countries. On the other hand, young women in Ghana significantly had higher education than their counterparts in the other three countries: 66% of women 15-19 had at least some secondary education in Ghana compared to 15% in Burkina Faso, 23% in Malawi and 27% in Uganda. In all four countries, the majority of young women were living with at least one biological parent. However, while only a slight variation exists across the four countries in the proportion living with both parents, substantially more adolescent women were living with only their mothers in Ghana, Malawi and Uganda than in Burkina Faso. Among adolescents who were not living with a parent, higher proportions were in union in Burkina Faso and Uganda. There is little or no variation across all four countries in the wealth status of the households adolescent women came from. On the other hand, adolescents in Ghana tended to have the greatest access to mass media. The characteristics of young men in these countries closely mirror those of their female counterparts (Table 1, Columns 5-8). For example, two out of three were 15-17 years old and most lived in the rural areas in all countries, with the exception of Ghana where almost one half lived in the urban areas. Similarly, the vast majority of them (67-71%) were currently in school in Ghana, Malawi and Uganda, compared to only 22% in Burkina Faso. However, in all countries, including Burkina Faso, higher proportions of adolescent men than women were currently in school. In all four countries, the vast majority (67-77%) of adolescent men were living with at least one parent, although this proportion is higher in Burkina Faso and Ghana than in the other two countries. As in the case of women, young men who were living with only one parent were more likely to be living with their mother than their father. On the other hand, unlike their female counterparts, nearly all adolescent men in all four countries who were not living with a parent were not in union. As in the case of women, the households in which adolescent men live show little or no variations with respect to their wealth status. Finally, young men in Ghana were the most exposed to mass media, followed by their counterparts in Malawi, but in all countries, adolescent men were more likely to be exposed than women of the same age. Sexual activity and condom use Sexual activity The level of sexual activity is fairly high among adolescents in all four countries. Among women aged 15-19, 29% in Ghana, 37% in Malawi, 45% in Burkina Faso and 48% in Uganda have had sexual intercourse. Among adolescent men aged 15-19 this proportion was 34% in Burkina Faso, only 15% in Ghana, 60% in Malawi and 49% in Uganda.21-24(Table 4.2). Thus, the proportion ever sexually active is considerably lower among young men in Burkina Faso and Ghana than observed among young women. On the other hand, it is higher in Malawi and about the same in Uganda. Current sexual activity, as measured by the proportion of 15-19-year-olds who had sex in the 12 months preceding the survey, is not trivial either (Figure 1). Among all females, 39% in Burkina Faso, 38% in Uganda, 28% in Malawi, and 21% in Ghana, are sexually active. Current sexual activity is lower among young men aged 15-19 in Burkina Faso, Ghana and Uganda and higher in Malawi than among their female counterparts. Nevertheless, with the exception of Ghana where 10% reported being sexually active in the past year, the proportions in the other countries are 25% or higher. Condom use Ever use of the condom among ever sexually active adolescents aged 15-19 is moderately high. Among adolescent females, this proportion is 32% in Burkina Faso and 43-48% in Ghana, Malawi and Uganda. As is commonly found in similar studies, adolescent males tend to report more condom use than their female counterparts. The same is true in the present study, as ever use of the condom is reported by 50-53% of sexually active young men in Burkina Faso, Ghana and Uganda. This proportion is 46 in Malawi.21-24(Table 5.4). With respect to current use of the condom, currently sexually active adolescents, particularly women, have a long way to go to adequately protect themselves. Among women aged 15-19 who had sex in the 12 months prior to the survey, 23-27% in Burkina Faso, Malawi and Uganda and 37% in Ghana used condoms at last intercourse (Figure 2). These proportions are much higher among their male counterparts. Almost one half of young men reported use of the method in Burkina Faso, Ghana and Uganda (46-49%). In Malawi, this proportion is 35%. Adolescents who had sex in the last 12 months and did not use a condom at last intercourse were asked why they did not use the method. The two most important reasons given by the 15-19-year-old males are that they "felt safe" and "didn't have condom".21-24(Table 8.2) In Burkina Faso, 28% and 30% gave these reasons, respectively. The corresponding proportions were 35% and 24% in Ghana, 45% and 37% in Malawi and 35% and 24% in Uganda. Among the 15-19 year old females, wanting to become pregnant was the most important reason given in Burkina Faso (29%) and Ghana (22%). But in Malawi and Uganda, the most important reason females gave for not using a condom at last sex was that they "felt safe" 53% and Uganda respectively. Knowledge of correct condom use Most of young women 15-19 were aware of condoms: this proportion is 83-86% in Burkina Faso and Malawi and 93-95% in Ghana and Uganda (Table 2). Among young men of the same age, the proportions who knew about the condom are even higher in all four countries : 90-94% in Burkina Faso and Malawi and 96-98% in Ghana and Uganda. In all countries, adolescent males reported greater awareness of the condom than females. While reports of awareness of the condom is generally high, it does not necessarily signify the existence of good or deep knowledge about the method. Responses to the following factual statements about correct use of condoms are better measures of knowledge about the method beyond awareness. "Condom should always be put on before sexual intercourse starts" Responses to this statement among young women show a high level of knowledge about the condom, with 75-81% responding in agreement with the statement (Table 2). Among adolescent men, this proportion is even higher in each country, ranging from 84% in Ghana and Uganda, to 88-89% in Burkina Faso and Malawi. In all countries, young men's reported agreement with the statement is significantly higher than that of their female counterparts. "Condom should be put on the penis only if the penis is fully erect or stiff" Among young women and men, knowledge of the condom implied by the responses to this statement is also high, although not as high as indicated by the responses to the first statement above. For adolescent women the proportion responding affirmatively to this statement is lowest in Ghana (52%) and ranges from 63-65% in Burkina Faso and Malawi and 72% in Uganda (Table 2). Among young men, although the proportion varied quite widely across the four countries, it is higher than that observed among adolescent women. The proportion is highest (91%) in Uganda, 81-85% in Burkina Faso and Malawi and 76% in Ghana. As in the case of the first statement above, adolescent men were more likely to agree with this statement than adolescent women. "Condom can be used more than once" Responses to this statement also show a high level of knowledge among young women, although wide variations are observable across countries. Based on the proportion that indicated disagreement with this statement, the proportion demonstrating accurate knowledge about the condom is 50% in Malawi, 64% in Uganda and 69-74% in Ghana and Burkina Faso (Table 2). As in the case of women, knowledge of the condom is high and variable among adolescent men. This proportion is 68-69% in Ghana and Malawi, 76% in Uganda and 84% in Burkina Faso (Table 2). Thus, in all countries but one (Ghana), the proportions of young men indicating good knowledge about the condom by responding negatively to this statement is higher than that of their female counterparts. Summary measure of knowledge of correct use When responses to all three statements were considered together, findings show that much lower proportions of adolescents have very good knowledge about how to use condoms correctly (Table 2). Among women 15-19-year-olds, 26% in Malawi, 40% in Ghana, 43% in Uganda and about 50% in Burkina Faso responded correctly to all three of the statements. In all four countries, however, adolescent males tended to have better knowledge of correct use of the method than their female counterparts. The proportion with correct responses to all three statements range from 50% in Ghana to 68% in Burkina Faso. The difference is particularly pronounced in Malawi (about 28 percentage points). That young men demonstrated considerably better knowledge of correct use of condoms is partly due to the fact that the condom is a male method. Determinants of knowledge of correct condom use Table 3 presents, among adolescent men aged 15-19, the results of the ordered logistic regression of the likelihood of knowing how to use condoms correctly on two intermediate educational factors (i.e. having seen condom demonstration and exposure to sex education in school) and selected characteristic variables. Without controlling for background characteristics, having seen a condom demonstration and having received sex education both came up as significant predictors of knowledge of correct condom use in three of the four countries - the only exception is Malawi (Model 1). Having seen a condom use demonstration increased the odds of knowing how to use the method correctly by 2.9 times in Burkina Faso, 1.6 times in Ghana and 1.3 times in Uganda. Similarly, adolescent males who received sex education were 1.3-1.7 times as likely to know how to use condoms correctly as those who were not exposed to sex education. When the effects of background characteristics were accounted for, having seen a condom use demonstration remained a significant predictor of knowledge of correct condom use in the three countries (Burkina Faso, Ghana and Uganda) and the inclusion of the controls does not appear to alter the strength of the association (Model 2). On the other hand, with the inclusion of the characteristics variables, the effect of having received sex education in school, which was marginally significant in Burkina Faso, was wiped out. However, the variable remained a strong predictor of knowledge of correct condom use among young men in Ghana and Uganda, although the strength of the effect was slightly diminished in both cases. The effects of the characteristic variables were not as consistent across the four countries, with the exception of age which emerged as a significant predictor of knowledge of correct condom use in three of the countries (Burkina Faso, Ghana and Uganda). In these three countries young men aged 18-19 were 30-37% more likely to know how to use condoms correctly than younger adolescents 15-17 years of age. In Burkina Faso and Malawi, adolescents from middle class households were about 1.5 times as likely as those from poor household to have knowledge of correct condom use. In Burkina Faso, this effect was significant, though marginally, for adolescent males who lived in wealthy households compared to those in poor households. Young men who were exposed to the radio regularly in Burkina Faso and Uganda were also 1.4 and 1.5 times respectively, as likely to know how to use condoms correctly as those who did not have such exposure. The effect of urban residence was significant only in Malawi with the odds ratio of 1.83. Also in Burkina Faso, adolescent males who read news papers regularly were 43% less likely to have knowledge of correct condom use compared to their counterparts who did not. This counter intuitive finding may be associated with small number of respondents who are able to read. As shown in Table 1, literacy rate, even among adolescents, is very low in Burkina Faso. For young women aged 15-19, the results of the ordered logistic regression of the likelihood of knowing how to use condoms correctly on the two intermediate educational factors (i.e. having seen a condom demonstration and exposure to sex education) and selected characteristics variables are shown in Table 4. Without controlling for the effects of background variables, both having seen condom use demonstration and having received sex education in school emerged as significant predictors of knowledge of correct condom use among adolescent women in Burkina Faso, Ghana and Uganda (Model 1). When the effects of background characteristics were accounted for, the strength of the relationship between having seen a condom use demonstration and knowledge of correct use of condoms remained largely stable (Model 2). In these three countries, the odds of knowing how to correctly use the method among those who have seen condom use demonstration was 3.6, 3.0 and 1.7 times higher, respectively, than the odds among those who have not seen condom use demonstration. Among the three countries where having received sex education in school showed up as a significant determinant of knowledge of correct condom use before the background factors were included in the model, only in Uganda did that the effect remain significant after the introduction of the background variables. On the other hand, in Malawi, having had sex education in school became a significant determinant of knowledge of correct condom use only when the effects of the characteristic variables were accounted for. A number of the characteristic variables also emerged as important predictors of knowledge of correct condom use among adolescent females aged 15-19 (Model 2). The effect of age was significant in Ghana, Malawi and Uganda. In all three countries young women aged 18-19 were 1.3-1.5 times as likely to know how to use condoms correctly as younger adolescents 15-17 years of age. In Ghana and Malawi, place of residence was also an important factor, but the effect was not unidirectional: in Ghana, urban resident adolescents were more likely to exhibit knowledge of correct condom use than their rural counterparts, while the reverse was the case in Uganda. Young women who have ever attended school in Ghana, Malawi and Uganda tended to exhibit a greater knowledge of correct condom use than their counterparts who have never been to school. The effect was particularly strong in Malawi where the former were about 2.6 times as likely as the latter to have such knowledge. Being exposed to radio regularly in Burkina Faso, Malawi and Uganda also predisposed young women to being more likely to know how to use condoms correctly than those who did not have such exposure. The effect of this variable was only marginally significant in Malawi and Uganda. Malawian young women who have secondary school education or more were 1.4 times as likely as those who have less than secondary education to know how to correctly use condoms. Similarly, adolescents who came from middle class households were 82% more likely than those from poor household to have knowledge of correct condom use. Consistency of condom use As noted in the introduction, it is not only important that young people use condoms in order to protect against STIs, including HIV, and unwanted pregnancy, it is also necessary that they use the method correctly and consistently. Only consistent use of the condom has been found to offer effective protection against HIV infection. However, due to paucity of data, little is known about how consistently young people use the condom. The National Survey of Adolescents provides a golden opportunity to examine this important subject. Men aged 15-19 who had intercourse in the last 3 months were asked to indicate how many times they had intercourse and whether or not condoms were used in each of the cases. From responses to these questions, the extent to which adolescent men used the condom consistently in the 3 month prior to the survey is examined. Percent of adolescent men who used condoms consistently: Table 5 presents the proportion of adolescent men 15-19 who had intercourse at least two times in the last 3 months and used condoms consistently (i.e. at every act of sexual intercourse). This proportion is moderately high but nowhere near the desired level of 100% for truly effective protection. It was 38% in Burkina Faso, 47% in Ghana, 20% in Malawi and 36% in Uganda (Table 5). About 19-22% of adolescent men in Burkina Faso and Ghana and 28-30% in Malawi and Uganda used the method during some of their sexual acts in the last 3 months and between 32% and 50% did not use at all. In all four countries, there are significant sub-group differences. For example, in both Malawi and Uganda, older adolescents reported more consistent use of condoms than their younger counterparts (Table 5). The reverse is the case for Ghana (55% versus 43%). With the exception of Malawi, adolescent men who lived in urban areas and those who were currently in school reported more consistent use of the condom than those who lived in the rural areas and those who were not in school. The level of education is positively associated with consistent use of the condom in all countries but one (Malawi). In Burkina Faso and Uganda, household wealth status is also positively associated with consistent use of the condom, but the pattern does not seem to be unidirectional in Ghana and Malawi. In all countries but Malawi, the number of media sources (radio, television and print media) that adolescent men were regularly exposed to tended to be positively associated with consistent use of the condom. With the exception of Burkina Faso, young men who had 2 or more sexual partners in the last 12 months tended to be less likely to report consistent use of the condom in all countries. Determinants of consistent use of condoms Table 6 shows the results of ordered logistic regression models of the effects of behavioral and characteristic variables on the likelihood of using the condom consistently in the last 3 months, among sexually active adolescent men aged 15-19. Of the four behavioral variables included in the model, age difference between partners and exposure to sex education in school emerged as significant predictors of consistent condom use in the 3 months preceding the survey (Model 1). With respect to age difference between partners, young men whose last intercourse was with a woman about the same age as themselves were 84% more likely to use the condom all of the times compared to those whose last partner was 5 or more years younger or whose partner was younger but the age difference was not known. Similarly, adolescent men who received sex education in school were almost twice as likely as those who did not to use condoms consistently in the last 3 months. Since this model was estimated using pooled data for three countries (Burkina Faso, Malawi and Uganda), we included in the Model a variable to measure country effect. The result shows that Malawian adolescents were significantly less likely (36%) to use condoms consistently than their Burkinabe counterparts. The inclusion of interaction between the country variable and the two behavioral factors that were significant in Model 1, show two results with respect to the effect of age difference between partners (Model 2). First, the main effects of age difference between partners became stronger: adolescents whose partner was about the same age as themselves were now about 1.7 times more likely than those whose partner was 5-9 years younger to use condoms consistently. Second, the effect of age difference between partners was indeed country specific. Ugandan adolescent men whose partners were about the same age as themselves were about 56% less likely to use the condoms consistently than adolescent men in Burkina Faso who had sex with women about the same age as themselves. With the inclusion of background variables (Model 3), exposure to sex education ceased to be a significant determinant of consistent condom use. The presence of education, which showed up as a strong predictor of consistent condom use, may partly be responsible for this change. On the other hand, both the main effect and the interaction effect of age difference between partners remained unaltered. Adolescents who had sex with partners about the same age as themselves were more likely to use the condom consistently than those whose partner was 5-9 years younger and the effect of age difference was more prevalent in Burkina Faso than in Uganda. Among the background characteristics included in the model, age, residence, education, living arrangement, exposure to radio and exposure to print media all emerged as significant predictors of consistent condom use among adolescent men (Model 3). Net of age difference between partners and other correlates, age of the respondent exerts a marginal effect (significant at 10% level) on the likelihood of consistent condom use. Adolescents who lived in urban areas were slightly more than two times as likely to use condoms consistently as those in the rural areas. This may be due to better access to the method and/or better knowledge about it in the urban areas. Similarly, the odds of using the condom consistently among adolescents who had at least secondary education was almost two times as high as the odds among those who had less than secondary school. Adolescent men who lived with their biological mother only were about 75% more likely to use condoms consistently than their counterparts who lived with no biological parents. Both listening to the radio and reading newspapers regularly predisposed adolescent men to being almost twice as likely to use the condom consistently as those who were not so exposed. However, exposure to television and household wealth status were not significant predictors of consistent condom use. Summary and conclusion As they go through the process of maturation, which includes becoming sexually active, adolescents in Sub-Saharan Africa are confronted with the risk of HIV and AIDS and unplanned pregnancy. How they negotiate their journey through this critical stage of adolescence with respect to their degree of success in protecting themselves against the dual risk is crucial for their health and well-being as well as those of their offspring. Their success or lack of it in this regard also has implications for the health and well being of the future productive and reproductive population of their respective countries and the region as a whole. It is for these reasons that, young people must be supported and enabled to successfully confront the challenges of STIs, including HIV, and unplanned pregnancy. Because of the unique dual protection it offers, for sexually active people, the condom has become a popular method being promoted for meeting these challenges. For young people, many of who do not have sex regularly, the method is particularly appropriate because it is coital dependent. However, while the condom can provide effective protection against these risks, research has shown that only correct and consistent use of the method can achieve this goal. It is therefore not enough to encourage young people to use condoms, it is equally important to help them to be effective users of the method. This paper examined knowledge of correct condom use and the consistency of use of the method among adolescents aged 15-19 in four Sub-Saharan African countries; Burkina Faso, Ghana, Malawi and Uganda. The results show that in most of the four countries included in this study, many adolescent women and men aged 15-19, are sexual active, although there is a wide variation across countries. Of the four countries, Ghanaian adolescents are considerably the least likely to have had sex in the last 12 months. Awareness of the condom among adolescent women and men aged 15-19 is very high in all four countries. However, when it comes to exactly what they know about the method, knowledge does not equate awareness, with the former being much lower. The proportion who ever heard about the condom tends to be higher among all adolescents in Ghana and Uganda than among their counterparts in Burkina Faso and Malawi. Young people in the first two countries may either have paid more attention to programs promoting the methods or they may have remembered having heard about the method through such efforts more than their counterparts in Burkina Faso and Malawi. Many sexually active adolescent women and men have used condoms at one time or the other in their life. This is particularly the case among young men than women. This differential by sex is very well known, as many studies have shown that men often tend to report more condom use than women even among those in marital relationships. However, it is still unclear whether this is due to actual difference in use or reporting error, as it may be argued that women may fail to report condom use because their partner, not they, put on the device. Furthermore, while most of the young men who reported ever use of the method used it at last intercourse, among women, reported use of the method at last sex is substantially lower than ever use. This is partly associated with the faster changing marital status for women than men. Research has demonstrated that condom use is not at all popular in marriage. While many young women aged 15-19 are already married, virtually none of the young men the same age have done so. Knowledge of correct condom use among adolescents aged 15-19 lags substantially behind awareness about the condom. An examination of young people's responses to individual indicators of knowledge of correct use of the method, shows that their knowledge varies from high to moderate with males demonstrating a higher knowledge of correct use of the method than females. When the responses are aggregated by developing an index measure of knowledge of correct use, the result shows that young people's knowledge of correct condom use is only about half as high as it could be. This suggests that there is room for improvement in this area if we are to expect adolescents to use the method correctly. In all countries, male adolescents are significantly more likely to have higher knowledge of correct use of the method than females. This is encouraging since men are the ones who actually use the method. Nevertheless, it is equally important and more advantageous to help improve knowledge of correct use of the method among adolescent females as well. Education, especially practical education, is a major determinant of knowledge of correct condom use. One form of practical education considered in this study is exposure to a condom use demonstration. This variable is a consistent and strong predictor of knowledge of correct use in all of the countries, with the exception of Malawi. This suggests that programs that aim at promoting condom use should include condom use demonstrations as a way of promoting correct use of the method. In the current study, evidence shows that the majority of the 15-19-year-old adolescents who know about the condom have not seen a demonstration of its use in all four countries. With the exception of Uganda, exposure to this practical education is much lower among young women than men _ 35% versus 49% in Burkina Faso, 48% compared to 57% in Ghana, 20% versus 30% in Malawi and 58% compared to 52% in Uganda.21-24(Table 8.4) As the evidence suggests, adolescents in Malawi are particularly in need of this training. Ever received sex education in school predicts knowledge of correct condom use in two countries, Ghana and Uganda. Its effect was only marginally significant in Burkina Faso before controlling for the effects of background characteristics. With the exception of female adolescents in Malawi, 75-93% of 15-19-years old adolescents who reported that their schools offered sex education also reported that they had received the instruction. However, while this statistic is impressive, in all countries, much lower proportions of adolescents who have attended school reported that their schools offered the instruction.21-24(Table 9.2) The above evidence shows that when sex education is available in schools, most young people get it (except female adolescents in Malawi). The main obstacle to receiving the instruction is unavailability of the program in school. Therefore, effort should be made to introduce age appropriate sex education in schools so that young people can receive relevant instructions before they become sexually active. For those who are no longer in school, there is need for out of school programs aimed at meeting this need. The mass media and community based organizations, such as youth clubs, can serve as sources of reliable sexual and reproductive health instructions for out of school youths. Evidence on consistency of condom use is available only for adolescent males. The findings show that in general adolescents are not doing particularly well in this respect. In all countries, less than one half of adolescent males aged 15-19 who had sex more than once in the 3 months before the survey used the condom consistently (i.e. in all sexual acts). However, there is hope as the results for some of the countries show that the situation could be better. Consistent condom use is most evident among adolescents in Ghana, where close to half of the young men reportedly used the method consistently and least so in Malawi, where only 20% reported consistent use of the method. These results are consistent with what is known about young people's access to sexual and reproductive health information in the countries. For example, as shown above, among these four countries, Ghana leads the way with respect to young people's exposure to sex education and having seen condom use demonstration. On the other hand, Malawi came last both in terms of young people's access to sex education in general and having seen a demonstration of condom use. Age difference between partners is often considered as a measure of female autonomy and ability to negotiate reproductive outcome, including condom use.28 Precisely, women who have sex with older men are believed to be less likely to request that the partner uses condoms compared to those who have sex with their peers. This study confirms that position with respect to consistency of condom use. Young men who have sex with women about the same age as them are more likely to use condoms consistently than those whose partners are 5-9 years younger than them. Also, although the effect is not significant, the sign of the odds ratio of consistent condom use for adolescent men whose partners are older is in the expected direction. Thus, a wide age gap between partners in favor of the male partner tends to preclude consistent condom use, thereby putting the partners at risk of STIs, including HIV, and unplanned pregnancy. This finding is worrisome. Programs that encourage sexual relationship among peers as well as those that help young women to develop high self-esteem and confidence to effectively negotiate condom use will help adolescents to live healthy sexual and reproductive lives. Sex education is another important predictor of consistent condom use. Independent of the effects of other factors, adolescent men who received sex education in school are significantly more likely to use condoms consistently compared to those who did not. Although the exact timing of the sex education is not known, most of the adolescents who received the instruction in school reported that they received it before becoming sexually active.21-24 Also, while the detail of what was taught in such sex education is not known, the fact that it is strongly associated with consistent condom use is encouraging. It suggests that there is something young people are learning from the instruction that is impacting their use of condoms positively. Again, this points to the need for sex education to prepare young people for healthy sexual and reproductive relationships. The program should include explicit instruction about correct and consistent use of the condom. The effects of urban residence, higher level of education, listening to the radio regularly and reading the newspaper regularly on consistent condom use are strong and in the expected direction. In all cases, these effects may be operating on the likelihood of consistency of condom use through greater access to information and contraceptive methods, particularly condoms. The findings about adolescents living arrangement is worthy of some attention. Adolescent males who lived with their biological mother only are more likely to use the condom consistently than those who lived with no biological parent. Also, although the effects are not statistically significant, the sign of the odds ratio of consistent condom use for adolescents who lived with a biological father only and those who lived with both biological parents are in the right direction. In general, living with biological parents, especially the biological mother, tends to be protective by promoting consistent condom use. Evidence from a recent study using the same data used in this study suggests that these effects operate not through parent-child communications but rather through parental monitoring.29 In other words, adolescents whose parents know what they are doing are more likely to protect themselves than those whose parents know little or nothing about their activities. Naturally, parental monitoring is more feasible when adolescents live with their parent. In conclusion, sexually active adolescent women and men are making efforts to protect themselves against the risk of HIV and unplanned pregnancy through condom use. Use of the method among this group is fairly high. Many of them have a good knowledge of how to use the method correctly and many are actually using it consistently. However, to achieve the desired protection there is substantial room for improve-ment in all areas _ level of condom use, knowledge of correct use of the method and consistency of use. To attain this goal, young people as well as their adult gatekeepers must join efforts. While young men and women must make greater efforts to improve their protective behaviors, findings from this study point to areas that policies and programs can address to provide adolescents access to the kinds of information and services they need to achieve healthy sexual and reproductive lives. For example, as noted earlier, one of the two main reasons adolescents in this study gave for not using condom at last intercourse is that they "didn't have condoms". This suggests that adolescents lack adequate access to the method. While, lack of supply may not be the only cause of this, it has been shown that condom supply is grossly inadequate in Sub-Saharan Africa.30 There is need to address this situation and to ensure that young people who need the method have easy access to it. Acknowledgements The authors would like to thank Ann Biddlecom and the anonymous reviewers for comments on earlier drafts of this paper. This research was supported by The Bill and Melinda Gates Foundation, The Rockefeller Foundation, and the National Institute of Child Health and Human Development (Grant#5 R24 HD043610). Reference
© Copyright 2007 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh07043t3.jpg] [rh07043f2.jpg] [rh07043f1.jpg] [rh07043t2.jpg] [rh07043t1.jpg] [rh07043t4.jpg] [rh07043t5.jpg] [rh07043t6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}