 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
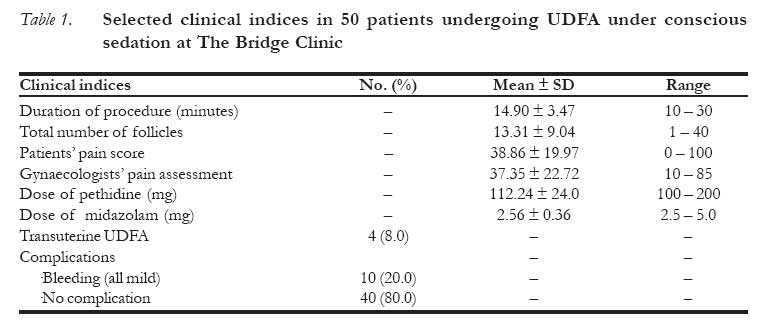
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 30-34 Experience with Conscious sedation for Oocyte Retrieval in Nigeria L’expérience avec la sédation consciente pour la récupération de l’ovocyte au Nigéria Fiebai PO*, Ogunmokun AA, Ajayi RA The Bridge Clinic, 41 A Evo Road, Phase II GRA, Port Harcourt Author for correspondence: e-mail: preye.fiebai@obgyn.net Code Number: rh08005 ABSTRACT Conscious sedation is the most common method of pain relief used during ultrasound-directed transvaginal follicle aspiration (UDFA) for in-vitro fertilisation/embryo transfer (IVF/ET). It is associated with minimal risks and facilitates early discharge following UDFA. The aim of this study was to assess clients’ pain experience, acceptance of conscious sedation and correlates of pain during oocyte retrieval for in vitro fertilisation (IVF) at The Bridge Clinic, Port Harcourt. It was a crosssectional survey conducted between May 1 and October 31 2004. Pain was assessed using a 100mm visual analog scale (VAS). Clients’ pain experience and correlates were evaluated using Pearson’s correlation and the student’s t-test. The mean pain score was low and the duration of the procedure did not significantly affect the severity of pain felt by the client. Most (69.0%) clients would prefer the same sedation and analgesia for any subsequent procedure. Conscious sedation and analgesia are one of several methods used to relieve pain during oocyte retrieval in IVF procedures. The information in this study is of value when considering the management of pain in patients undergoing oocyte retrieval procedures. (Afr Reprod Health 2008; 12[1]:30-34). KEY WORDS: Pain, Conscious sedation, In vitro fertilisation, Nigeria. RÉSUMÉ La sédation consciente est la méthode la plus commune de soulagement de la douleur dont l’on se sert au cours de l’aspiration folliculeuse transvaginale dirigée par l’ultrason (AFDU) pour la fécondation in vitro/le transfert de l’embryon (FIV/TE). Il est lie à des risques minimaux et ren facile la décharge précoce. L’objectif de cette étude est dévaluer l’expérience de la douleur, l’acceptation de la sédation consciente et les corrélats de la douleur pendant la récupération de l’ovocyte en vue de la fécondation in vitro à Bridge Clinic a Port-Harcourt. Il s’agissait d’une enquête transversale qui a été menée entre le Ier mai et le 31 octobre 2004. On a évalue la douleur à l’aide d’une échelle analogue visuelle (100mm) (EAV). L’expérience de la douleur ressentie par la cliente et ses corrélats ont été évalués à l’aide de la corrélation de Pearson et le test de ‘t’ de l’étudiant. La cotation moyenne de la douleur était faible et la durée du processus n’a pas affecté la sévérité de la douleur ressentie par la cliente. La plupart (69,0%) des clients préféreraient la même sédation et l’analgésie pour une procédure future. La sédation consciente et l’analgésie constituent une méthode parmi plusieurs dont on se sert pour soulager la douleur pendant la récupération de l’ovocyte dans les procédures. Les renseignements contenus dans cette étude ont une valeur quand on considère le traitement de la douleur chez les patientes qui subissent les procédures de la récupération de l’ovocyte. Introduction Oocytes used for in vitro fertilisation (IVF) are usually collected surgically after superovulation, and fertilised with prepared sperm in the laboratory. Historically, laparotomy was initially used for oocyte retrieval but abandoned because of the morbidity associated with the procedure.1 Laparoscopy became the standard procedure employed by IVF/ET programs worldwide, following Steptoe and Edwards’ IVF success using oocytes retrieved laparoscopically.2 This was an invasive technique requiring general anaesthesia and associated with some morbidity and rarely, mortality. Transvaginally oocyte retrieval sonographically controlled using an abdominal sector scanner was first reported by Gleicher et al in 1983.3 With the availability of endovaginal probes, the procedure is now carried out tranvaginally, with a needle attached to the probe. It is minimally invasive and has since then become the method most commonly employed by assisted conception units worldwide. Anaesthetic options for transvaginal follicle aspiration include general and epidural anaesthesia, conscious sedation, local injection or no anaesthesia at all.4 The ideal pain relief during oocyte recovery by transvaginal follicle aspiration should be effective and safe, easy to administer and monitor, short acting, and readily reversible with few side effects.4 It should provide adequate analgesia, without being sedating to the point of airway compromise and should not reduce the chances of pregnancy. General anaesthetics traverse easily into follicular fluid and may have detrimental effects on cleavage rates of embryos and pregnancy rates, and as such are not popular in IVF.5-9 Conscious sedation is defined as a “minimally depressed level of consciousness that retains the patient’s ability to maintain a patent airway independently and continuously and to respond appropriately to physical stimulation and verbal commands”.10 It is the most common method of pain relief used for UDFA by IVF units worldwide. Conscious sedation is used for UDFA at The Bridge Clinic and affords the patient quick return to normal activity while avoiding the risks of anaesthesia. The aim of this study was to evaluate the clients’ pain experience, acceptance of conscious sedation and correlates of pain following UDFA. Methods This was a cross-sectional study carried out between May 1 and October 31 2004, at The Bridge Clinic, Port Harcourt. Infertile patients presenting for IVF/ET were recruited at UDFA. Subjects were randomly selected amongst all clients who underwent UDFA during the period. Informed consent was obtained from all clients who were also counselled before the procedure. Conscious sedation was achieved with 50mg of pethidine and 2.5mg of midazolam given intravenously. Sedation was adjusted with 50mg increments of pethidine and/or 2.5mg of midazolam based on the gynaecologist’s perception of the client’s response to pain during the procedure. UDFA was performed with the patient in lithotomy position using a 7.5mHz transvaginal ultrasound probe with a needle bracket attached. Oocyte retrieval was carried out with a 17 gauge Wallace needle attached to a suction trap system comprising a 14ml Falcon tube connected to a negative pressure suction pump. A self-administered questionnaire was filled by the client on full recovery after UDFA. Biosocial data and pain perception were recorded by the client while clinical indices and pain perception were entered by the gynaecologist who carried out the procedure. Pain levels were measured by a 100mm linear (0 = no pain to 100 = the most severe pain) visual analogue scale (VAS). Satisfaction with the procedure was assessed on a 5-point Likert-type scale (1 – Poor, 2 – Fair, 3 – Satisfactory, 4 – Very good, 5 – Excellent). Data collation and analysis was carried out with SPSS for Windows (version 11.0, SPSS Inc, Chicago, IL, USA) computer software. Pearson correlation and the student’s t-test were used as appropriate. Statistical significance was set at p - values of = 0.05. Results The patients’ mean age was 33.7 ± 4.9 (22 – 43) years, with 28 (56%) aged less than 35 years and 9 (18.4%) over 38 years. Majority 44(88%) were professionals or highly skilled workers. Forty-six (92%) had tertiary education while the rest had secondary education. The mean duration of UDFA was 14.90 ± 3.47 (range 10-30) minutes and an average of 13.31 ± 9.04 (1-40) oocytes were collected from the patients. The mean pain score reported by patients was 38.38 ± 19.97 (0-100) and that by the gynaecologist was 37.35 ± 22.72 (10 – 85). The mean dose of pethidine given was 112.24 ± 24.0 (100 – 200) mg while that of midazolam was 2.56 ± 0.36 (2.5 – 5.0) mg. Trans-uterine collections occurred in 4(8.0%) patients and mild bleeding from the oocyte retrieval needle puncture site was the only complication encountered in 10 (20.0%) of patients. Selected clinical indices are summarised in Table 1. There was significant correlation between the patients’ pain experience and their analgesic preference in future procedures (Pearson’s correlation (r) = 0.30, p = 0.006).The gynaecologists assessment of the patients pain response during UDFA also correlated with the clients pain perception (Pearson’s correlation = 0.283, p = 0.05). Pain experienced by the patient did not however correlate with age, educational level, duration of the procedure, dose of sedation given, the number of follicles punctured, and the involvement of the uterus during UDFA (Table 2). Majority (64%) of the patients would prefer to have the same dose of conscious sedation in any subsequent UDFA, 30% would want increased sedation/analgesia and 6% would prefer no analgesia. None was in favour of general anaesthesia. Discussion The importance of pain relief during surgical procedures cannot be overemphasised. Few studies have addressed analgesia and anaesthesia in human reproduction4, and this report to the best of our knowledge, is the first from West Africa where assisted reproductive technology is still poorly developed.11 The visual analog scale (VAS) used for assessment of pain experience in this study has been reported as being highly reliable in the assessment of acute pain.12 The mean pain score was low (38.86 ± 19.97) ranging from no pain to the most severe pain (0-100). Interestingly, the client who experienced the most severe pain would still want conscious sedation in any subsequent UDFA albeit at increased doses. Ng et all reported lower pain scores in patients given conscious sedation and paracervical block with lignocaine for oocyte retrieval.13 Their patients however received much higher doses of conscious sedation than those in our study. Most clients in this study expressed satisfaction with conscious sedation used for analgesia during oocyte retrieval, with 94% indicating a preference for it in any subsequent procedure. This was not influenced by the previous anaesthetic experiences of 18(36%) who had undergone various operations including UDFA, laparoscopy and caesarean section, for which general anaesthesia is commonly employed. Information given to them on the possibility of general anaesthetics affecting fertilisation may have influenced their choice, but most preferred to be given the same dose indicating their satisfaction with the analgesia. UDFA is a short procedure rarely requiring prolonged administration of analgesia/ anaesthesia. Pethidine which was used for analgesia in these clients has an onset of 10-45 minutes and duration of action of 2-4 hours while midazolam given intravenously, has a rapid onset, relieves anxiety and reduces the patient’s memory of the procedure. The mean duration of the procedure in this study was about 15 minutes and these drugs provided adequate pain relief and sedation. The dose of conscious sedation is adjusted according to the patient’s response to pain. This is difficult to determine while the patient is sedated and is usually assessed by the perception of the gynaecologist from the patients’ reaction. There was a positive correlation between the gynaecologist’s and the patient’s assessment of pain during the procedure. Dose adjustment based on the gynaecologists’ perception was therefore appropriate. There was no correlation between the duration of the procedure, the number of oocytes collected and the pain experienced by the clients. The analgesic effect of pethidine during the short procedure was most likely adequate. Dose adjustment for patients with many follicles and oocytes may also have accounted for the satisfactory analgesia and sedation in them. Recovery was prompt in all cases and there were no side effects of the sedation. Minimal bleeding from the puncture sites in the vaginal fornices were the only complications reported and application of pressure to the bleeding points was adequate for haemostasis. Conscious sedation and analgesia are one of several methods used to relieve pain during oocyte retrieval in IVF procedures. The information in this study is of value when considering the management of pain in patients undergoing oocyte retrieval procedures. We conclude that conscious sedation is an acceptable method of pain relief in assisted conception and recommend its application for short term management of pain in oocyte retrieval by UDFA. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08005t2.jpg] [rh08005t1.jpg] |
| |||||||||

{kind=link}
{kind=link}