 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 35-46 Sexuality and Health: A Study of Tanzanian Men’s Experiences of Living with HIV/AIDS Sexualité et santé : étude sur l’expérience des hommes tanzaniens séropositifs Balaile, Gunnel , Kayombo Jacob, Ransjo - Arvidson Anna - Berit, Hojer Bengt Kayombo, Jacobb B.A., Philosophy., HIV counselor Ransjö-Arvidson, Anna-Berita, d R.N.M, Ph.D., Associate Professor, Höjer, Bengt a, c, M.D., Ph.D., Professor, Code Number: rh08006 ABSTRACT The aim of this study was to explore Tanzanian men’s experiences regarding their health and sex life after they had been diagnosed with HIV. In-depth interviews were performed with a purposive sample of ten men living in an urban area in Tanzania and who had been HIV positive for more than one year. A phenomenological-hermeneutic approach was used for analyzing the transcribed interviews. Three themes emerged from the texts; “awareness of HIV infection”, “perceived and ideal health”, and “sex life a source of happiness and caring”. Living with HIV meant profound adjustments to daily life activities for the participants. HIV forced them to learn new ways of having sexual intercourse and new ways of acting as a man. The meaning of being a “real man” had changed from being a man with great sexual prowess to being a “caring man” within one relationship. KEY WORDS: HIV; sex life; phenomenological-hermeneutic method; interviewsRÉSUMÉ Cette étude avait pour objectif d’explorer les expériences des hommes tanzaniens à l’égard de leur santé et de leur vie sexuelle après avoir été diagnostiqués comme étant séropositifs. Des interviews en profondeur ont été recueillies à l’aide d’un échantillon calculé de dix hommes qui résident dans une région urbaine en Tanzanie et qui étaient séropositifs depuis plus d’un an. On s’est servi d’une approche herméneutique phenomenologique pour analyser les interviews transcrites. Trois thèmes sont sortis des textes ; «la conscience de l’infection VIH», «la santé perçue et idéale», et «la vie sexuellecomme une source de joie et d’affection». Être séropositif signifiait des ajustements profonds aux activités de la vie quotidienne pour les participants. Ils ont été obligés par le VIH d’apprendre les nouvelles manières d’avoir des rapports sexuels et de nouvelles façons de se comporter comme des hommes. Le sens attribué au fait d’être un «vrai homme» avait changé d’étant un homme à grande prouesse pour devenir un «homme plein d’affection», au sein d’une relation. Introduction More than twenty years have passed since the first outbreak in Africa of the human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS). The pandemic has had devastating consequences in sub-Saharan Africa, which has 64% of all HIV sero- positive people in the world. Tanzania bears a substantial share of the global epidemic, with an estimated HIV prevalence of 7% among adults aged 15 to 49. Women have a prevalence of 8%, while men have 6% prevalence. In cities and towns, the average HIV prevalence is 11%, which is twice the level found in rural areas1. In Dar es Salaam in 2001, 42% of STI clinic patients diagnosed with another sexually transmitted disease (STD) were also tested positive for HIV2. A report from the Tanzanian Commission for AIDS states that the predominant mode of transmission of HIV infection is unprotected heterosexual intercourse (77%). Mother-to-child transmission constitutes about 5%, and blood transfusion makes 0.5%. About 17% of the reported cases had no transmission mode stated3. In 2000, UNAIDS started a world campaign called Men Make a Difference. There were several reasons to focus on is; men’s behavior puts women at risk for HIV, and unprotected sex between men endangers both men and women. Instead of blaming the men efforts should be geared to encourage positive, responsible and informed behavior by including as many men as possible in the global struggle against HIV4. According to Connell5 the characteristics of being a man have generally included being physically strong, emotionally robust, daring, and virile. A standard or traditional view of men is hegemonic masculinity. Masculine hegemony does not mean total control; it is not automatic; and it may be disrupted, or even disrupt itself. In order to understand men’s sexuality, we need to understand the construction of masculinity, the social production of what it means to be a man, and that there are multiple masculinities5. Masculine sexuality is intimately linked to male gender identity. Successful physical performance of masculine sexuality is essential for the confirmation of men’s masculinity6. African men have their own visions of what a man should be, and they have discussed them actively for generations. Topics include marriage, fatherhood, domestic labor, and other things that define manhood. Even companionate marriage had a vital meaning to men during the Mau Mau rebellion in Kenya in the fifties, as described by White7. Those men who fought in the forest wanted companionate marriages, one wife with whom to share all they had experienced7. Social, economic, and legal changes brought by colonial rule gave women and younger men opportunities for autonomy from elder men who had gained or maintained political or economic power in relation to the colonial capitalist system, and who supported patriarchy in the home8. In post-colonial time in rural and urban East Africa, socioeconomic changes have made men increasingly disempowered, and many men are caught in a paradoxical and frustrating situation. They are the acknowledged heads of households, but they are often unemployed or their salaries are not high enough for them to fulfill their expected roles as men and husbands. Men’s social value, their self-esteem and masculinity has been hard hit and men have then to find new ways to manifest their masculinity. Many men seem to compensate for loss of social value and selfesteem by increased, often aggressive, sexual activity and by casual sex9. Various scientific studies have been conducted on sexual behavior. Comparatively few studies have focused on men’s experiences of living with HIV, and little has been written about what impact HIV has had on a person’s sex life. It has taken a long time to do a more in-depth study of infected people’s sexuality. Being an HIV carrier has typically been equivalent to having a death sentence. “Long-term survivors” is people who have lived with HIV for at least ten years without developing the disease. New treatments can prolong life expectancy of infected people; these treatments and prolonged life expectancy also bring fear of social exclusion to those infected. Because of this, sexual issues were not given top priority10. The aim of the present study was to explore Tanzanian men’s experiences of living with HIV in order to get a deeper understanding of their ways of thinking about and reflecting upon their health and sexual life. Method A qualitative methodology was selected phenomenological-hermeneutic interpretation that searches for detailed descriptions of the “life world” of the individual and met the criteria for elucidate the meaning of experiences living with HIV11 . Study setting and procedures This study was carried out in Dar es Salaam, Tanzania, during January and February 2004. Three study settings were chosen. One was an outpatient department in a governmental district hospital, and the others were clinics run by non governmental organizations (NGO) in the center of town. All the study settings provided HIV counseling by specially trained HIV counselors. According to the Tanzanian national policy for voluntary HIV testing, a pre-counseling session is given; and if HIV status is positive, the individual is registered and referred to special clinics for HIV counseling. Participants The sample was selected in order to obtain maximum variation. Our aim was to have a broad range of participants who would have a diversity of life experiences. All participants were men, they were present at the selected settings during the study days, and they fulfilled the inclusion criteria, i.e., they had known for more than one year that they were HIV positive. They were able to read and write in Kiswahili, and they were able to talk openly about their situation. Potential participants were informed about the aim of the study by HIV counselors. Those who agreed to participate were given a written and verbal explanation of the study, before signing the consent form. Illiterate men were not included in the study because we wanted all participants to be able to decide for themselves the value of the written consent information. All participants were also informed that they could withdraw from the study at any time, without being questioned or jeopardizing their future care within the health service. One client declined to participate without giving any reason. With respect for his integrity, no questions were asked. Ten men between 19 and 60 years of age volunteered to participate in the study. Of these, seven were between 35 and 44 years of age. Their level of education varied from 3 to 17 years. Six were Christians, and four Muslims. Four of the men were married, three were divorced or widowed, and three were single. Four of the men were long-term survivors. four of the men had known their sero-status four to six years, and two for one year. Interviews In-depth interviews were chosen as the method for data collection. All the interviews took place in privacy in the HIV counselor’s room in the respective study setting. The in-depth interviews were conducted in Kiswahili, and the participants were asked to talk freely starting from the following specific questions:
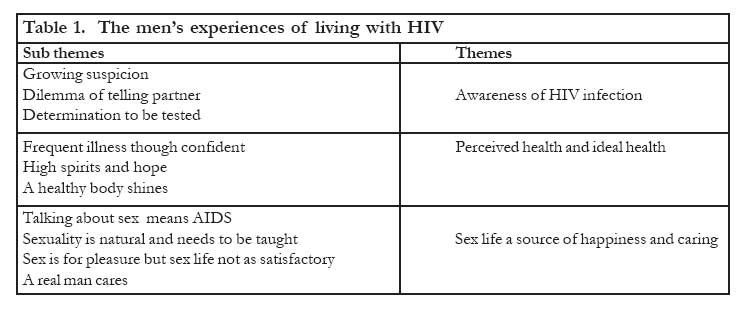
For each topic, additional questions were asked (probing) when the interviewer wanted the participants to develop their stories or if participants did not understand the questions or failed to express themselves or felt embarrassed. Each interview lasted about 60 minutes and was tape-recorded. During the interview, the first author made non-verbal observations, which were written down as field notes. Short demographic background information was collected from the interviewees. Data analysis The recorded interviews were transcribed verbatim. The interviewer thereafter translated the text from Kiswahili into English. A linguist specialist later checked the translation for its correctness and completeness. The transcribed and translated interview text was thereafter analyzed phase-by-phase using a phenomenologicalhermeneutic method, based on Ricoeur’s theory of text interpretation12, and further developed by Lindseth & Norberg13. The textual analysis involved three phases. In the first phase, the naïve reading, the text was read several times to obtain ideas about its sense and meaning and to obtain ideas about how to analyze it in detail during the structural analysis. The second phase, the structural analysis, was performed with the aim of identifying parts and patterns that had meaningful consistency and the explaining of the text including validation of the naïve reading. During this phase, the transcripts were analyzed for themes by comparing and contrasting the emerging themes (Table 1). The third phase a critical comprehensive understanding of the text as a whole, where the naïve understanding, the findings of the structural analysis, the literature, and the researchers’ preunderstanding were brought together into a comprehensive understanding. Ethical approval Ethical approval was obtained from the Ethical Committees of the National Institute for Medical Research, Dar es Salaam, Tanzania (NIMR); the Tanzania Commission for Science and Technology (COSTECH); and the Ethical Committee of Karolinska Institutet, Stockholm, Sweden. Findings The findings of the interviews are presented according to the phases of analysis: naïve reading, structural analysis, and critical comprehensive understanding. Naïve reading The naïve reading of the text revealed that the men struggled to survive and to continue their lives as normally as possible despite being infected by HIV. The interpretation of the text suggests that the struggle of living with HIV was a hardship of illness, poverty, and social stigma. The men wished to live normal lives, but they were caught by worries and anxiety for their dependents, and at the same time, they feared their own imminent deaths. Their sex lives had become less active, and either they had less sexual desire or their wife/partners were sick. They were also concerned about the danger of spreading HIV to others. All of them expressed deep frustration over not being in control over their own lives; at the same time, they could not accept being seen as victims of HIV. Structural analysis During the structural analysis three main themes emerged regarding the men’s experiences of living with HIV and what impact their HIV status had on their perception of health and sexuality. These themes were (1) awareness of HIV infection, (2) perceived health and ideal health, and (3) sex life as a source of happiness and caring (Table 1). Theme 1: Awareness of HIV infection Through the men’s personal accounts of how they became aware of being HIV infected, three sub themes were identified (Table 1). Growing suspicion The men’s struggle with uncertainty about their HIV status and their worries about their partners’ possible illnesses increased their suspicion that they were infected with HIV. Some of the men said that when their wives had suffered from an illness for some time and not recovered as expected, their suspicions had continued to grow. When they had exhausted all other explanations for their wives’ symptoms, the only thing that remained was to be tested for HIV. One man’s story follows. “My wife was sick for a long time. Last year her condition changed; it became more serious, so we went to the hospital for investigations […] but there was no improvement achieved. She got medical treatment […] without any notable changes […] my in-laws - they told me to take my wife to traditional healers, I refused and I went to several other hospitals but nothing happened. I took her to her uncle in the village […] her condition was getting worse. She wrote a message to inform me that she could die anytime and she instructed me to take her home. I brought my wife home and she was very sick […]. My father came and told me about a traditional healer […] I convinced him that I should take my wife to hospital. After more struggle to find a hospital to be attended to, I was told that my wife had all the signs of AIDS. African Journal of Reproductive Health Vol. 12 No.1 April, 2008 I told my wife about taking a test, and we both agreed to go for testing and we found that we were both affected. Now her health has improved. I don’t have any problems, though the laboratory tests have shown that I am HIV positive Dilemma of telling wife/partner The majority of the men had started to feel weak, with fever, coughing and aching bodies. However, in spite of these signs, one man was stunned when he realized that he was HIV positive. “My body weight was decreasing, and my partner suffered from diarrhea and headache. I was tested for HIV after consulted a physician. When I got the results, my wife was pregnant, so telling her was difficult.” Determined to be tested To have an HIV test without having experienced any health problems was unusual, but the lifestyle and friends’ illness had increased the need for being tested. One man expressed himself this way. “I used to live near the mines, and at that time we were enjoying life; people had money. Due to the mines, there was a mixture of lifestyles and women of different categories, so you could go with anybody without knowing that your friend had already been with her. I had sex with one woman who fell ill and later on she died. After her death, I did not hesitate to test my health, and I was found to be HIV positive.” The men expressed strong emotions of fear, guilt, and shame when they had received the test results and their wife/partners were informed. The men expressed clear feelings of come to terms with being HIV positive, and they were also clear that they were not victims of it. Theme 2: Perceived health and ideal health The second theme that emerged was on how the men experienced their health. Three sub themes were identified (Table 1). Frequent illnesses though confident The men were confident, but troubled by frequent illnesses. Bodily changes were something that they experienced due to their weight loss. They described permanent problems, such as skin rashes; genitalia itching, which brought a constant need for washing; and other consequences of opportunistic infections. Their feelings were also surrounded by thoughts of death. What helped them in troubled times was the NGO activities, such as counseling meetings and doing some little physical exercises. They were aware of how the virus caused health problems. “Of course my body is not so bad, but sometimes, as you know my condition is not good. It is said that when your immune system decreases your condition becomes unfit and you become sick most of the time. Now my problems are my chest and feet. I also have leprosy problems. But it is not so bad that I can’t walk, I even carry out minor activities.” The men felt confident with the help they got from the HIV counselors. One of the men said, “I am somehow weak […] According to my counselor we can only live on hope. Yes I am satisfied somehow.” High spirits and hope Feelings of high spirits and living in hope encouraged normal daily living, such as being happy about children’s improvements in school, meetings at NGOs that brought awareness of “not being alone” with the HIV infection, and still being alive. Real meaning to being alive came from having a big family to care for, especially children. As head of the family, it was important to give directions and make plans for the future. For two of the participants with no family, their wish was to live long enough to have a family. A healthy body shines This sub theme reflected their thoughts about what health could be and how they experienced their own health. A healthy person is an energetic person with a good facial expression, who is neither fat nor skinny and has a body that shines. Food, exercise, and hygiene are all important to maintain good health. One man, whose wife was also infected by HIV, said, “We know how to live with the virus [...] Taking care of our health means food, sleep, clothing, and protective sex to avoid new transmission.” Those who had not yet got any symptoms of infection felt well and did not suffer from any bodily symptoms such as weakness or weight loss. One man said, “People do not believe that I have the virus.” They were confused by his physical status and could not distinguish between different stages in HIV-affected persons, so he had to educate them. Some of the participants had never experienced any problems with the body; they ate nutritious food and treated minor symptoms early. However, they expressed a concern that medicine for treatment of different problems was very much needed, and living with HIV gave rise to great demands for several drugs. Theme 3: Sex life a source of happiness and caring When the participants were asked to talk about sexuality and sexual matters, they had difficulties finding adequate ways to express themselves or understanding the questions that were asked. Talking about sexuality brought feelings of anxiety. Four sub themes emerged (Table 1). Talking about sex means AIDS The men revealed that if they had to talk about sex, this meant AIDS. To discuss sexual matters was generally not a natural thing for them, which is something to keep in mind while reading about the findings. Talking about sexuality was simply something “one did not do”. If one did, as one man said, it is because “it’s my duty to do so.” One of the participants, however, was talkative about sexual matters. He spoke openly and straightforwardly about the topic, as both he and his wife had lived with HIV for a long time. The virus had changed their lives in many aspects, and they had become more used to talk about sexual matters. This man emphasized the need to educate the community on general sexual issues, to prevent the spread of HIV infection. “It is not easy to speak with your sisters about sex, but at this juncture, where AIDS is a threat, there is no shamefulness, as everybody knows that AIDS is transmitted through sex in almost 95% of the cases, so talking about sex matters means AIDS.” Another man talked very openly about how the sex act was carried out. He said, “We have a very big task: to talk about sex. We talk about it almost all the time.” Still, resistance to the question “Do you talk about sexual matters with your fellow friends?” was strong. The answers were “not yet”, “never”, or “I do not have such habits.” Those who talked about sex said that the most frequent topic was the use of condoms during sexual intercourse, in order to prevent further infection. One reason for not talking about sexual matters was that “the African tradition does not favor such talk, especially not between brothers and sisters.” Before knowing about their problems with HIV infection, there had been almost no discussion about sexuality. Sexuality is natural and needs to be taught It was not common among the men to search for more knowledge about sexuality. They had neither read books nor watched films or TV about sexuality, after they had been infected by HIV. Some of the men revealed that they had no new ways to search for more knowledge about sexuality, but this did not mean that their sex lives were just as they were before. When this topic was discussed one man answered, “Love must be there, love affairs have been there since the world started, and sex and love do not make any distinction between before and after being infected by HIV”. “The problem,” as one man said, “HIV and sexuality, they have a direct connection, as people have contracted the HIV disease through sexual intercourse”. For this man “his lack of knowledge” was the cause for his HIV status, and he was not pleased with this conclusion. He believed that “sex must be given attention so that happiness can be attained at all costs”. Another young man had little knowledge about sexual matters, and he said that he had few sexual experiences. His perception about sex was that it could not be controlled. For other participants, knowledge about sexuality was mainly about the physical act. They knew very well how women functioned with monthly periods and pregnancies. Referring to sexual rights as a husband, one man stated that he had arranged the frequency of meetings with his wife. “I have the right to have sex with my wife by using protective gear […] but when you think of life expenses there is no need for another child, although we know that there are drugs as niverapine which can protect a child from infection.” The men’s knowledge about sexual matters was generally not deep apart from their knowledge that sex had some hazards. Their point of view was that sexual education should be provided widely. One man said, “Apart from making sex I know nothing.” Sex is for pleasure but sex life not as satisfactory Some of the participants expressed that in love affairs each one should be satisfied, but said that love now had become a source of disease instead of procreation. Sexual satisfaction was not like it had been before they knew they were infected with HIV. It had been possible to have sex two or three times a day or week. At present, due to their partners’ infection and indisposition, sexual intercourse was maybe possible once in two or three months. One man, whose wife was also infected by HIV, said, “I have to wait until she feels OK, so I don’t get it when I need it.” Participants expressed that sex was for pleasure and that they wanted sexual satisfaction. However, “the virus” interfered and the men felt “it” to be a barrier. As one man said, “For myself there is no question of enjoyment because of the problem I have, and after being educated by the NGO, my wife and I understand and we have no such feelings”. The topic “sexual matters” had even been “forgotten” due to the virus. When the men had explained that they had no possibility for sexual satisfaction within a relationship, the probing question was asked, “To what extent do you practice masturbation?” Two men said they did masturbate occasionally, only when their feelings of desire were great; but the topic was very embarrassing, and in spite of the probing questions, the topic could not be moved further. For some men, satisfaction meant the same as agreeing to have sexual intercourse. Once the partner had agreed to have sex, it meant she was satisfied. Another way of knowing if the woman was content with their sexual life was simply to observe her, and by long experience it was possible to know one’s partner’s satisfaction. In general, the men believed that abstaining from sex was not possible for a normal man. As one man stated, “To abstain from sex can cause psychological problems and is not what a man should do; a man with ability does not expect such a thing”. One man admitted that he had no thoughts of abstaining from sex, but when his wife died he had to accept living without sex. A real man cares According to the men’s descriptions, a caring man was a perfect man who was not involved with his past sexual practices and, if he still was, he had regulations or demarcations, or had to use protective gear. For one man, a caring man had to use condoms but he himself had not cared because he had not used condoms. Now he blamed himself for that. It was generally easy to blame others for not caring, and the opinion was that the social environment and the nature of people were such that nothing influenced them. Another man thought that only AIDS victims care about preventing the spread of the virus. “The only person who takes care is the one who has been infected and has undergone continued education and training to take care, otherwise no one does.” Caring could also mean to be a man who needs sex and is able to satisfy his partner. However, for most of the men, a caring man considered the partner’s health and used condoms to prevent transmission of a sexual disease. To use a condom was thus a caring act in its real sense. In order to be able to care, however, the men said they needed knowledge and information about sexual matters; if information was lacking, it was not possible to care, as they did not understand what to do. The men stressed that it is most important for them to care for their families and for their family members to be there for one another. To be a couple means caring for each other. It also means that being close to one’s wife will protect the man from other women’s interference, which will help the man to keep his distance from other women. A woman who cares stays close to her husband. Where trust exists, there is no need to use condoms. As a man stated, “Because I don’t sleep around at random, my wife and I trust each other, so I can’t get a sexual disease”. A typical answer to the question about protective methods was, “I didn’t use any, and I trusted my partners”. The only acceptable rationale for the participants to use condoms was to prevent pregnancy. But to suggest condom use was a sign of “not loving the person”, and that would cause problems in the relationship. When a woman could no longer conceive, there was no need for any protection. A man stated that he did not sleep with anyone outside his marriage. He used to distribute condoms in his office, since he worked as a counselor, but he had never used a condom himself. He also declared that “condoms were the last alternative when all other means had failed. We normally insist on abstinence. We can’t advertise condoms as a protective measure […] because the majority has no knowledge on how to use them [...] that’s why I can’t regard it as protection.” Not all of the participants lacked experiences of using condoms. One man expressed, “During sex I use condoms. I can’t perform without protection gear.” Even so, he did not regard condoms as 100% safe, and it was apparent that none of the participants fully trusted condoms. Some of them did not have an active sex life and therefore thought there was no need for protection. Others lived in stable relationships where both were infected and felt that the need for protection was no longer necessary. This made condom use rare, and few of the men had experience of continuous use, which would increase in knowledgeable persons. As one man said”, I started to use condom when I heard about AIDS, but by then it was too late.” None of the participants had used condoms before they knew about HIV or knew about their own disease status. After the fear of what might happen had already occurred, the motivation to use condoms ceased. Comprehensive Understanding and Discussion In the last phase of the interpretation, the text was viewed as a whole. The naïve understanding and findings of the structural analysis, the literature, the field notes written during interviews, and the authors’ pre-understanding were brought together into a comprehensive understanding, which was discussed and agreed upon. The meaning of health and sexuality when being infected by HIV and the experiences of living with an incurable disease can be described as a process; which, on the whole, reflects the complexity involved in men’s awareness of being infected and their adjustment of coming to terms with the new situation. Despite altering health, the men perceived their health in a realistic way and could deal with difficult feelings and felt optimistic. Their feelings of hope made daily life struggles possible to overcome. The HIV infection had in every aspect changed the men’s lives. Their thoughts and reflections showed a deep concern and awareness over their situation. They expressed their feelings with responsibility by being more helpful and empathetic, and they showed more sensitivity towards their wives and children. For some of the men, living with HIV meant living alone or abstaining from sex. Continuing with a sex life was only possible for the participants with a wife/ partner also infected with HIV. All participants understood well that they had to change their sex lives and their relationships to their wife/partner to prevent further infection. They wanted to be close and share intimacy with their partners. Sharing intimacy with a partner meant, for example, talking about sexuality, which was a new experience and created expectations that required new knowledge about how to act as a man. Each participant in the study had accepted the notion to be with “one partner” from now on and regarded themselves as a “caring man within one relationship”. Having an active sex life was still important for nearly all of the men, but sexuality had lost it procreative meaning. Basic knowledge about HIV and other sexually transmitted infections had been taught in the NGO support group. Before that, none of the participants had considered themselves to have been a “caring man”. Reflections in relation to other research Awareness of HIV infection. When the correct diagnosis was finally recognized, the message was not difficult for some of the men to accept, because they had gone through a period of growing suspicions, which had turned into reality. Their main worries were about their partners, which surpassed any other feelings. They felt stunned with a dilemma when they had to tell their partners about their test results. Other studies have shown that disclosing sero- positive status to one’s partner is not an easy thing to do14, but those who have the courage to talk, also talk to a greater extent about safe sex15. Being tested for HIV meant acting courageously, and voluntary testing has increased along with the demands for counseling services, despite people’s fears of being positive16. The participants’ perceived and ideal health as well as their sex life changed when they were found to be infected with HIV. From now on, they had to boost their immune system and conduct intercourse with greater care to avoid re-infection. Their new knowledge about health care gave them hope to live for many more years. The men’s stories were about their struggle to cope with frequent illnesses and their worries about not being able to support and care for their families. To be there for their loved ones was something they highly valued. At the same time, their worries and their happiness had brought meaning to “being alive”. Their strong will to live had resulted in high spirits and living in hope; this strong will also brought feelings of optimism, not only to survive but also to “live a good life”. Other studies have shown that similar, spiritual feelings contribute greatly to well-being for people living with HIV17,18,19. A study from southern Finland20 describes hope as a basic resource in life and finds that believing in life makes it worth living at present and in the future. Hope helps people deal with difficult life situations and gives strength to live. In the present study, participants expressed the importance of having hope, and this was supported by their counselors. Sex life a source of happiness and caring. For many participants, talking about sex was the same as talking about AIDS. The men said that they were able to talk about sexuality even if it was something new, and some of the men had no difficulties in discussing topics such as condom use or sexual intercourse with their partners. Discussing extramarital affairs was more difficult; and when they answered questions on these issues, they showed feelings of unease and hesitation. Although extramarital affairs are rather common21, it was usually hard to admit and discuss. If both husband and wife were affected, the virus put an extra strain on and endangered their relationship. In order to continue to live together, they had to move beyond questions of guilt and had to reflect on consideration and caring for one another. The men’s views of sexuality had changed into seeing sex solely as a pleasurable activity and no longer as a procreation method. Having children was still a wish but no longer an acceptable reality. Traditionally, success and virility meant having many wives and fathering many children22. HIV/AIDS has forced the men to take on new views about sexuality and manhood. These new views were not easily accepted; because sexuality was connected with their own identity as men, the message impinged on personal integrity and self-esteem. To cope with this new way of looking at sexuality brought mixed feelings for some participants. According to Mbiti23, sexuality is seen as sacred in African cultures. Several religious and social aspects of sex are held sacred and respectable. “If there is a breach of them, these are taken very seriously […] and show clearly that Africans consider the proper uses of sex to be sacred and must therefore be safeguarded” (p 144)23. The men’s reluctance to talk about using condoms implied that a condom interfered with a sacred act. For these men, sexual intercourse is more for procreation than for recreation; because condoms interfere with sex performance, the men are anxious and afraid of failing24, 25 . Impotence is feared among men, and it has a similar psychological and moral effect on men as barrenness has on women26. The participants in this study considered a real man in the first place as a man with the ability to perform during intercourse, but also as a man who cares within a relationship. This perspective of looking upon manhood might open up the transcendence of gender barriers. The new knowledge the participants acquired from counseling and group sessions and at their NGO settings helped them cope better with this new life. Their knowledge was a hard lesson they had learned by living with the virus. The men’s thoughts and reflections showed a deep concern and awareness over their situation. They acted with responsibility by being more helpful and empathetic, and they showed more sensitivity towards their wives and children. For some of the men, living with HIV meant living alone or abstaining from sex. Continuing with a sex life was only possible for the participants with a wife/ partner also infected with HIV. Basic knowledge about HIV and other sexually transmitted infections had been taught in the NGO support group. Before that, none of the participants had considered themselves to have been a “caring man”. Methodological reflections It should be noted that this study was limited to ten Tanzanian men living with HIV and does not aim to reach generalizable findings, but rather to get a deeper understanding and shed light on peoples’ lived experiences. Findings in hermeneutic studies cannot be generalized but should be seen as arguments in an ongoing discourse12. The interviewer tried to protect the participants’ integrity by being sensitive to their reactions during the interviews. Maybe for this reason, none of the participants refused to answer the questions asked. The impression of the observer (first author) was that the participants were in an open and straightforward atmosphere and therefore spoke in an open and straightforward manner through the whole interview. Being the focus of the interview gave the participants an opportunity to express their troubled feelings, which could be helpful in their process of coping with their difficulties related to HIV infection. Feelings of shame and guilt might even have felt easier to deal with. Conclusion From interviews with ten men and the subsequent phenomenological-hermeneutic analysis, we conclude that the complex situation of being a man and becoming aware of carrying the virus was felt as a threat to the identity of being a man. However, the men had managed to cope with the situation and felt hope and optimism and they strived for living a normal life. That meant seeking a different kind of relationship with their partner/ wife and made it possible to continue with a sex life that confirms their identity as men. This new situation creates challenges for caregivers to understand the men’s narratives about struggling for meaning of their experiences of living with HIV. The men had learnt to take care of their health and knew how to prevent further spread the virus. It was a hard way of learning to become “a caring man”, but could be useful for other men and caregivers as model in the struggle of HIV preventive work. Acknowledgments This study was supported by grants from the Nordic Africa Institute, in Uppsala, Sweden; Dalarna University, Falun, Sweden; and Karolinska Institutet, Stockholm, Sweden. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08006t1.jpg] |
| |||||||||

{kind=link}